Open Journal of Radiology, 2013, 3, 130-132
http://dx.doi.org/10.4236/ojrad.2013.33021 Published Online September 2013 (http://www.scirp.org/journal/ojrad)
Right Hemisphere Cerebr al Infarction Due to Air
Embolism from Percutaneous Lung Biopsy: A Case Report
Chaitanya Ahuja1*, Yama Kharoti1, Jeffery J. Critchfield2, Meghna Chadha2
1Dotter Institute, Oregon Health & Science University, Portland, USA
2Wayne State University, Detroit, USA
Email: *drchaitanyaahuja@gmail.com
Received April 18, 2013; revised May 18, 2013; accepted May 25, 2013
Copyright © 2013 Chaitanya Ahuja et al. This is an open access article distributed under the Creative Commons Attribution License,
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
Percutaneous transthoracic needle biopsy is a common procedure in interventional radiology. Systemic arterial air em-
bolism causing cerebral infarction is a rare but much feared complication of percutaneous lung biopsy. We present a
comprehensive review of iatrogenic air embolism post-lung biopsy, a complication that is often sub optimally managed.
Patho-physiology, clinical features, and risk factors and management are reviewed.
Keywords: Air Embolism; Lung Biopsy; Cerebral Infarction; Computed Tomography (CT) Guidance
1. Introduction
A CT-guided need le lung biopsy is a common interven e-
tional radiology procedure. Percutaneous lung biopsy is
considered as a safe and effective method for obtaining a
tissue diagnosis in patients with lung masses. Reported
complications include pneumothorax, intrapulmonary he-
morrhage, hemoptysis, air embolism, seeding of the bi-
opsy tract, and death. The most common complication,
pneumothorax, is easily treated by radiologists and is
typically associated with no long-term sequela. Air em-
bolism as a complication is extremely rare; however it
can become fatal when it happens. Early diagnosis and
rapid application of hyperbaric oxygen therapy are the
mainstay of treatment.
2. Case Summary
An elderly gentleman with a known esophag eal mass and
multiple pulmonary nodules was referred for a CT
guided FNA biopsy of a pulmonary nodule. The patient
was placed in left lateral decubitus position on the CT
table. A 19 gauge needle was advanced under CT fluo-
roscopy into a righ t pulmonary nodule and FNA samples
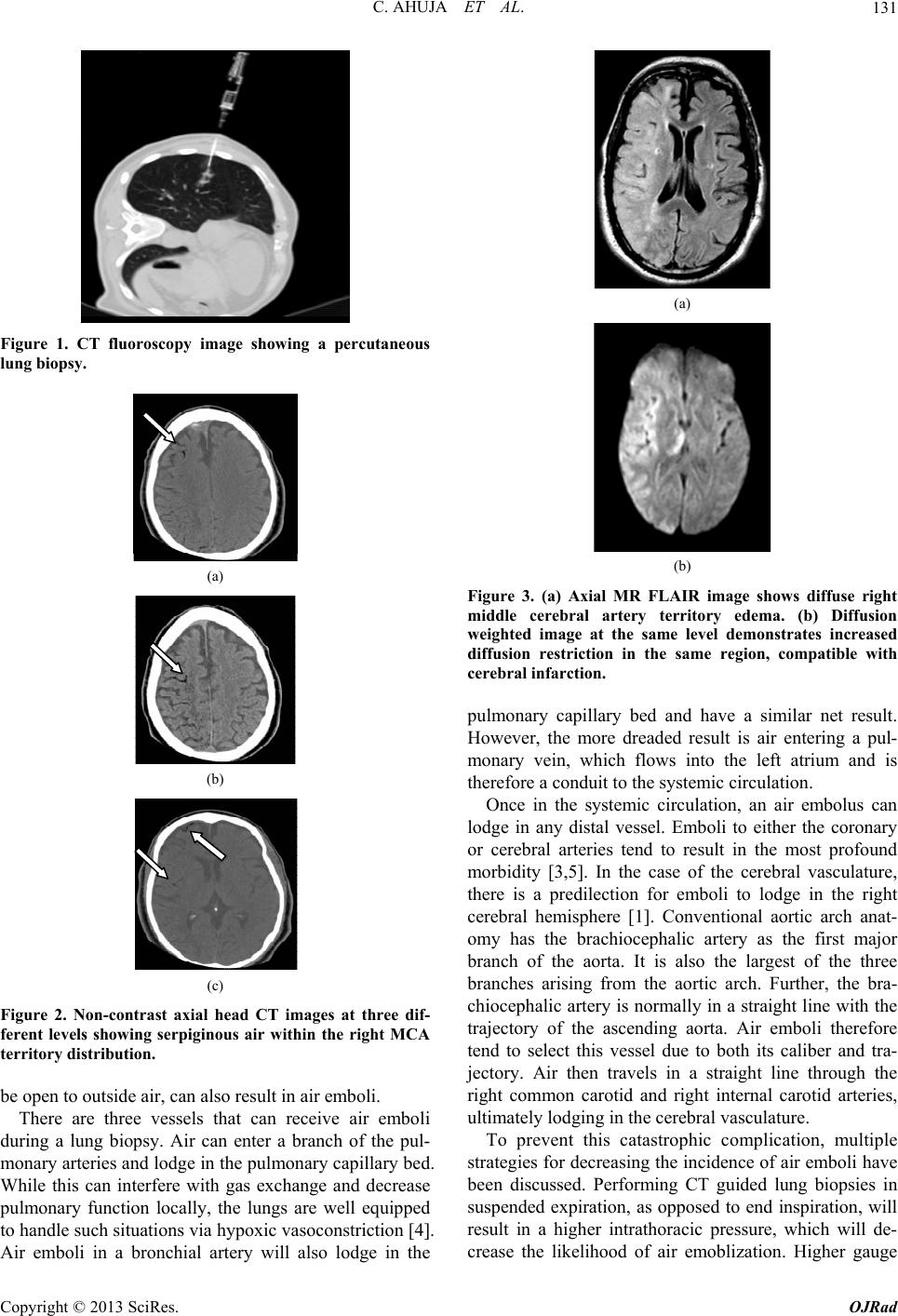
were obtained in end inspiration (Figure 1). During the
procedure the patient became verbally unresponsive and
rapidly developed left sided hemiplegia. Subsequently, a
partial seizure was witnessed on the CT table. The pro-
cedure was concluded and a non contrast head CT was
obtained (Figure 2). The head CT showed gas within the
right MCA (Middle Cerebral Artery) territory vessels.
Hyperbaric oxygen therapy was initiated as per the insti-
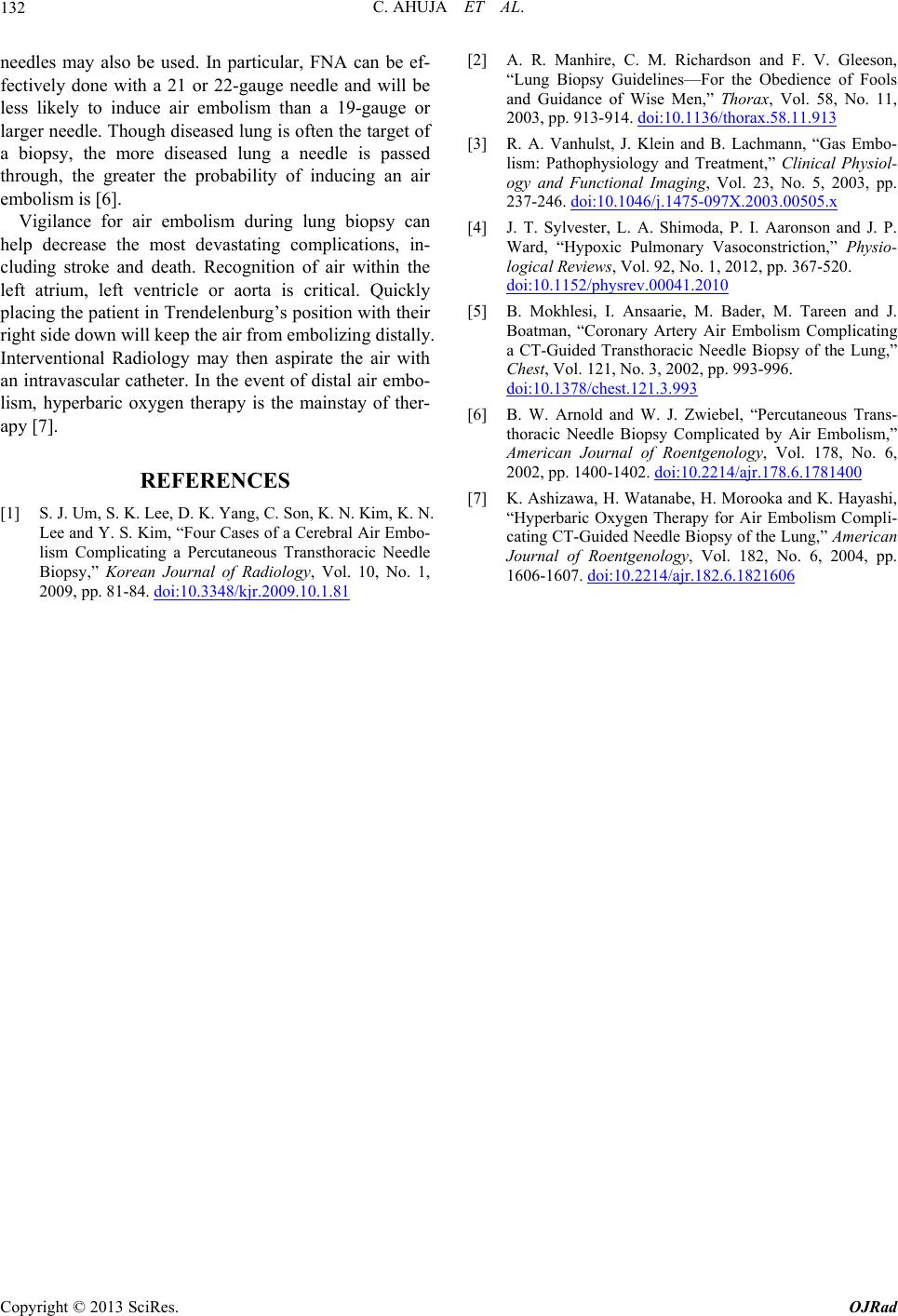
tutional air embolism protocol. A subsequent brain MR
showed T2/FLAIR hyperintensity in the right MCA ter-
ritory along with diffusion restriction, compatible with
cerebral infarction (Figure 3). The patient developed
permanent disability as a result.
3. Discussion
Percutaneous lung biopsy is one of the most common
procedures performed in radiology departments. It is the
minimally invasive gold standard for the histopathologic
investigation of lung masses. Compared with other per-
cutaneous biopsy procedures, lung biopsy carries a higher
risk of potential complications, including occasional re-
ports of death. Very few case reports have been de-
scribed in literature relating to cerebral infarction due to
air embolism from percutaneous lung biopsy. The largest
series of four cases has been reported from Korea [1].
Though rare, air embolization from percutaneous lung
biopsy is a known and potentially devastating complica-
tion. Indeed, the few cases of death reported from this
procedure are most often due to air embolism. It can
cause subsequent myocardial infarction, intractable ar-
rhythmia or stroke [2]. The primary mechanism for in-
troduction of air embolism is the creation of an air-
way-pulmonary vessel fistula during the procedure [3].
Issues with technique, such as allowing the needle hub to
*Corresponding author.
C
opyright © 2013 SciRes. OJRad