Characterization of Candida Species Isolated from Cases of Lower Respiratory
Tracr Infection among HIV/AIDS Patients in Calabar, Nigera
Copyright © 2013 SciRes. WJA
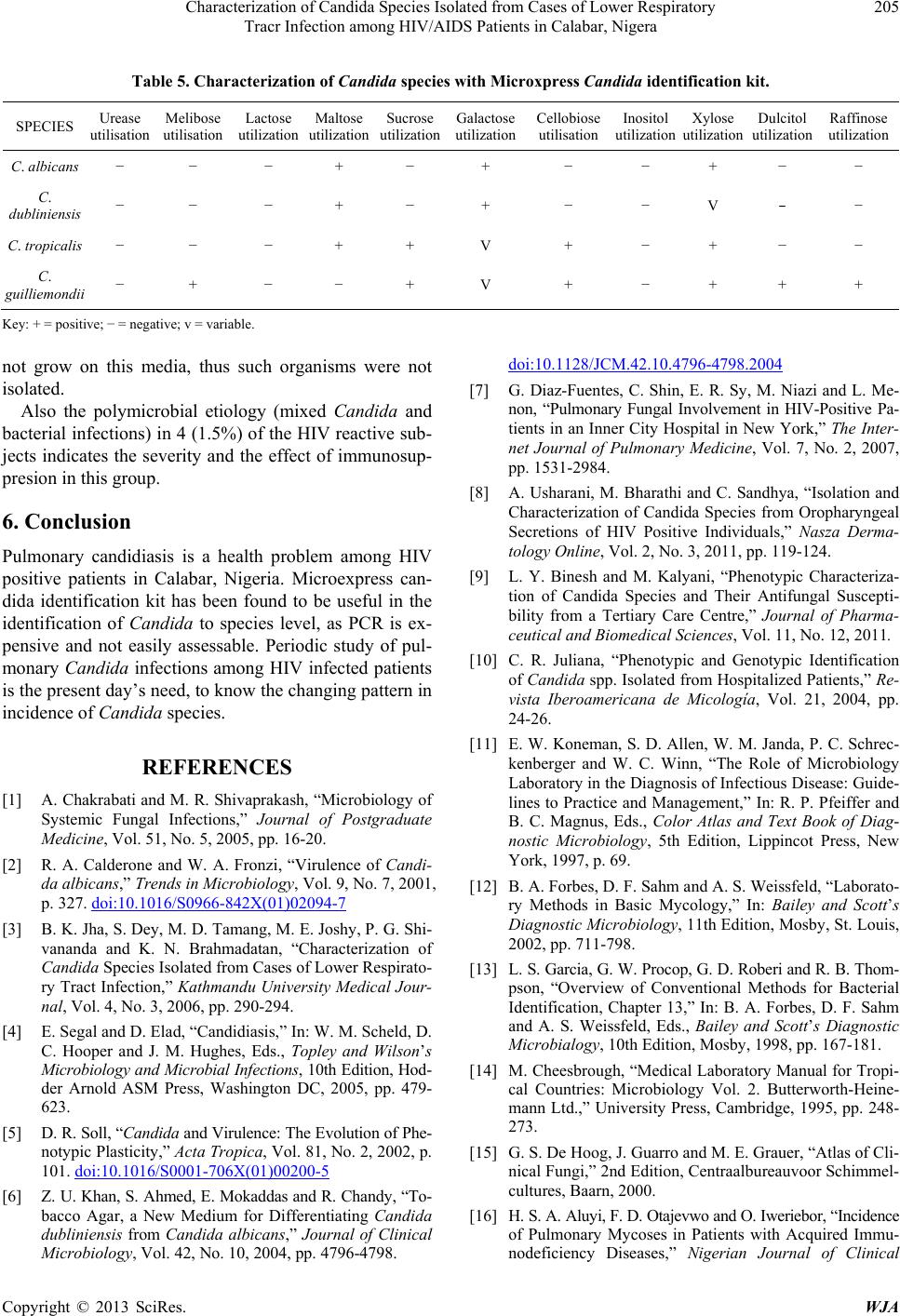
Table 5. Characterization of Candida species with Microxpress Candida identifi cation kit.
SPECIES Urease
utilisation Melibose
utilisation Lactose
utilization
utilization Sucrose
utilization Galactose
utilization Cellobiose
utilisation Inositol
utilization Xylose
utilization Dulcitol
utilization Raffinose
utilization
C. albicans − − − + − + − − + − −
C.
dubliniensis − − − + − + − − V − −
C. tropicalis − − − + + V + − + − −
C.
guilliemondii − + − − + V + − + + +
Key: + = positive; − = negative; v = variable.
not grow on this media, thus such organisms were not
isolated.
Also the polymicrobial etiology (mixed Candida and
bacterial infections) in 4 (1.5%) of the HIV reactive sub-
jects indicates the severity and the effect of immunosup-
presion in this group.
6. Conclusion
Pulmonary candidiasis is a health problem among HIV
positive patients in Calabar, Nigeria. Microexpress can-
dida identification kit has been found to be useful in the
identification of Candida to species level, as PCR is ex-
pensive and not easily assessable. Periodic study of pul-
monary Candida infections among HIV infected patients
is the present day’s need, to know the changing pattern in
incidence of Candida species.
REFERENCES
[1] A. Chakrabati and M. R. Shivaprakash, “Microbiology of
Systemic Fungal Infections,” Journal of Postgraduate
Medicine, Vol. 51, No. 5, 2005, pp. 16-20 .
[2] R. A. Calderone and W. A. Fronzi, “Virulence of Candi-
da albicans,” Trends in Microbiology, Vol. 9, No. 7, 2001,
p. 327. doi:10.1016/S0966-842X(01)02094-7
[3] B. K. Jha, S. Dey, M. D. Tamang, M. E. Joshy, P. G. Shi-
vananda and K. N. Brahmadatan, “Characterization of
Candida Species Isolated from Cases of Lower Respirato-
ry Tract Infection,” Kathmandu University Medical Jour-
nal, Vol. 4, No. 3, 2006, pp. 290-294.
[4] E. Segal and D. Elad, “Candidiasis,” In: W. M. Scheld, D.
C. Hooper and J. M. Hughes, Eds., Topley and Wilson’s
Microbiology and Mic robial Infections, 10th Edition, Hod-
der Arnold ASM Press, Washington DC, 2005, pp. 479-
623.
[5] D. R. Soll, “Candida and Virulence: The Evolution of Phe-
notypic Plasticity,” Acta Tropica, Vol. 81, No. 2, 2002, p.
101. doi:10.1016/S0001-706X(01)00200-5
[6] Z. U. Khan, S. Ahmed, E. Mokaddas and R. Chandy, “To-
bacco Agar, a New Medium for Differentiating Candida
dubliniensis from Candida albicans,” Journal of Clinical
Microbiology, Vol. 42, No. 10, 2004, pp. 4796-4798.
doi:10.1128/JCM.42.10.4796-4798.2004
[7] G. Diaz-Fuentes, C. Shin, E. R. Sy, M. Niazi and L. Me-
non, “Pulmonary Fungal Involvement in HIV-Positive Pa-
tients in an Inner City Hospital in New York,” The Inter-
net Journal of Pulmonary Medicine, Vol. 7, No. 2, 2007,
pp. 1531-2984.
[8] A. Usharani, M. Bharathi and C. Sandhya, “Isolation and
Characterization of Candida Species from Oropharyngeal
Secretions of HIV Positive Individuals,” Nasza Derma-
tology Online, Vol. 2, No. 3, 2011, pp. 119-124.
[9] L. Y. Binesh and M. Kalyani, “Phenotypic Characteriza-
tion of Candida Species and Their Antifungal Suscepti-
bility from a Tertiary Care Centre,” Journal of Pharma-
ceutical and Biomedical Sciences, Vol. 11, No. 12, 2011.
[10] C. R. Juliana, “Phenotypic and Genotypic Identification
of Candida spp. Isolated from Hospitalized Patients,” Re-
vista Iberoamericana de Micología, Vol. 21, 2004, pp.
24-26.
[11] E. W. Koneman, S. D. Allen, W. M. Janda, P. C . Schrec-
kenberger and W. C. Winn, “The Role of Microbiology
Laboratory in the Diagnosis of Infectious Disease: Guide-
lines to Practice and Management,” In: R. P. Pfeiffer and
B. C. Magnus, Eds., Color Atlas and Text Book of Diag-
nostic Microbiology, 5th Edition, Lippincot Press, New
York, 1997, p. 69.
[12] B. A. Forbes, D. F. Sahm and A. S. Weissfeld, “Laborato-
ry Methods in Basic Mycology,” In: Bailey and Scott’s
Diagnostic Microbiology, 11th Edition, Mosby, St. L ouis,
2002, pp. 711-798.
[13] L. S. Garcia, G. W. Procop, G. D. Roberi a nd R. B. Thom-
pson, “Overview of Conventional Methods for Bacterial
Identification, Chapter 13,” In: B. A. Forbes, D. F. Sahm
and A. S. Weissfeld, Eds., Bailey and Scott’s Diagnostic
Microbialogy, 10th Edition, Mosby, 1998, pp. 167-181.
[14] M. Cheesbrough, “Medical Laboratory Manual for Tropi-
cal Countries: Microbiology Vol. 2. Butterworth-Heine-
mann Ltd.,” University Press, Cambridge, 1995, pp. 248-
273.
[15] G. S. De Hoog, J. Guarro and M. E. Grauer, “Atlas of Cli-
nical Fungi,” 2nd Edition, Centraalbureauvoor Schimmel-
cultures, Baarn, 2000.
[16] H. S. A. Aluyi, F. D. Otajev wo and O. Iweriebor, “Incidence
of Pulmonary Mycoses in Patients with Acquired Immu-
nodeficiency Diseases,” Nigerian Journal of Clinical