Diagnosis of HIV Delay: Lost Opportunities
198
in the hospital database to know the number of times that
the patient had consulted a doctor in the emergency area,
general practitioners and sp ecialized consultation s during
the previous year to the diagnosis and the motifs of that
consultation. Furthermore, we analyzed patients that had
attended one or several healthcare lev els. As to the range
of frequency of attention, we called low attendance to
those patients that came between one and three times to
any level of healthcare and high attendance to tho se who
came over 4 times. With this information a database was
performed and the data was analyzed with the SPSS 18.0
statistical programme.
3. Results
In the period of time between 2005 and 2011, 107 cases
were diagnosed. In our series the global percentage of di-
agnosis delay was 61.7% of the cases (66 patients). From
these, 45.38% (30 patients) fulfilled the criteria of ad-
vanced disease.
It was possible to find information about the existence
of sanitary assistance in the previous year to the diagno-
sis in 59 patients (45 men and 14 women). The median of
age found was 40 years-old. From these, 34 were diag-
nosed with delay (58%), fulfilling the criteria of ad-
vanced disease in 16 (27%). The main way of infection
was the sexual one: 49% heterosexual and 47% homo-
sexual. The use of intravenous drugs meant 3% of the
cases.
As to the cultural level 54% did not have any studies
or just primary studies and 36% had medium or higher
education. 35 patients attended an only healthcare level
(60% GPs, 23 Emergencies and 17% specialized consul-
tations), 19 to two levels and 5 patients to the three
healthcare levels. In relation to the frequency of atten-
dance, 52% of patients had low attendance and 47.5%
went over three times. They applied for a total of 274
consultations, among which we highlight: 14.6% due to
febrile syndromes without apparent focus, 11.7% for
constitutional syndrome, 10.6% for diarrhea, 9.8% had
any sexually transmitted d isease (STD), 8.8% respiratory
symptoms with or without fever and 8.4% for derma-
tological lesions.
4. Discussion
The objective of our present work is to transfer some re-
flections after checking some clinical facts in the daily
routine practice of an infectious disease consultation that
has concerned us. The HIV outbreak is not under con-
trol in Spain [1,3]. Several thousands new people are in-
fected each year, despite consciousness raising cam-
paigns and the information transmitted to the population
and the affected organizations. In the last 6 years, in the
Infectious Diseases Clinical Management Unit, we have
diagnosed 107 new cases of infected people by HIV,
mainly male (74.8%) and in 90.7% of cases the way of
transmission was the sexual one.
The diagnosis delay g oes on being a reality both in the
rest of the Span ish series (45% - 67%) [1,4 ,5] and in ours,
with unacceptable percentages. There exists another da-
tum even more worrying, which is that more than 25% of
the cases had the criteria of an advance disease or even
that 1 of each 4 cases had been diagnosed coinciding with
an opportunistic disease of AIDS [1,4]. Our results were
even a bit higher: 61.7% of diagnosis delay and from
these, 45.38% presented with advanced disease criteria.
What attracts our attention is that from 59 p atients that
in any occasion had asked for medical assistance previ-
ously, 58% were diagnosed with delay, fulfilling crite-
rion of advance disease in 27%. Furthermore we find that
almost half of the cases (44.7%) had attended any doctor
from 4 to 14 times or even in the three healthcare levels.
However, it should be marked that the study being retro-
spective is a limitation, since it is difficult to get all the
data, and some cases could have been underestimated
due to private centres attendance, which have not been
taken into account. In our series a total of 274 consulta-
tions were made, in many cases with symptoms that cli-
nically were suggestive of HVI infection.
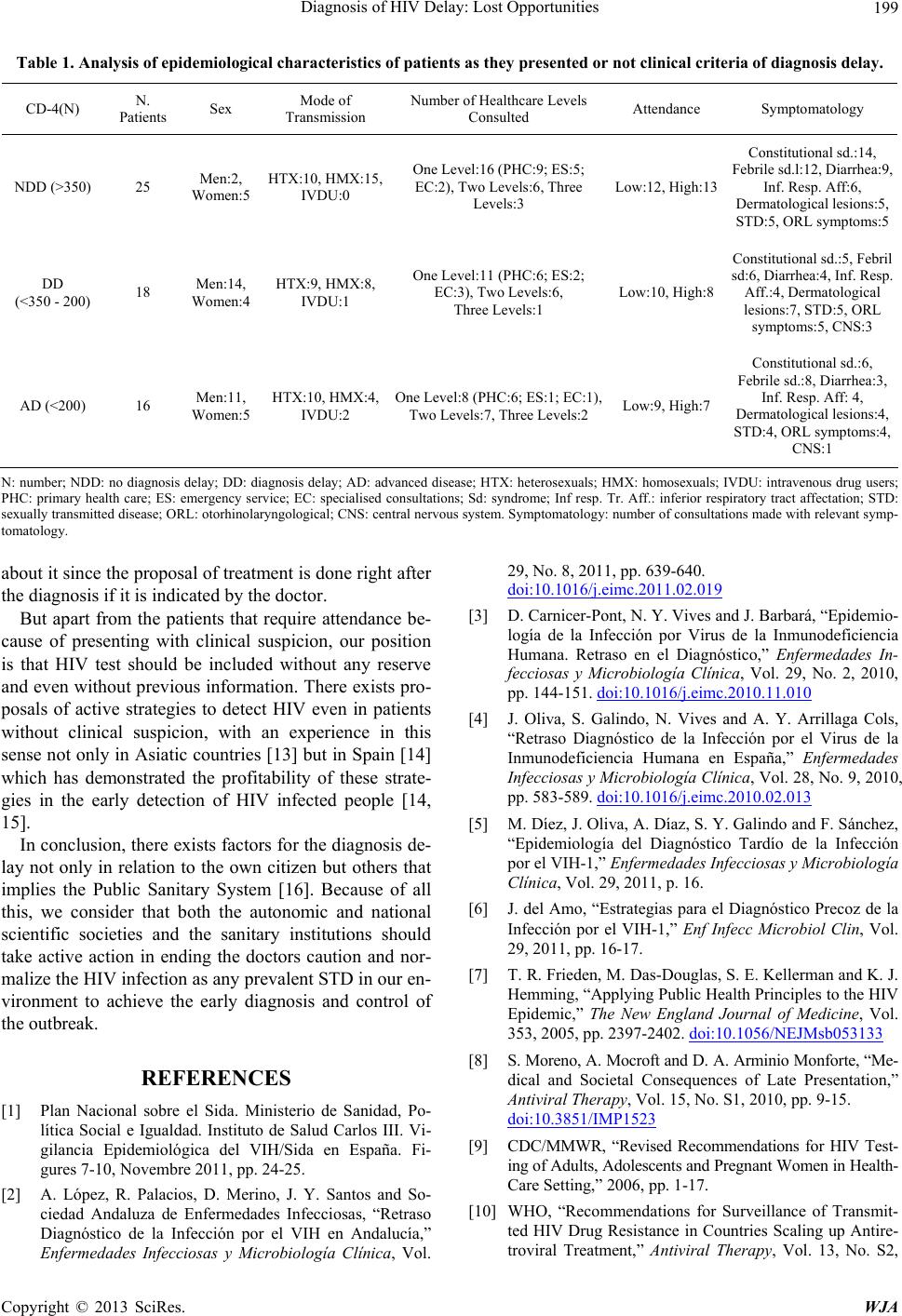
Patients diagnosed with delay had mainly consulted
for constitutional syndromes, febrile syndromes without
apparent focus, diarrhoea, sexually transmitted diseases,
dermatological lesions, respiratory infections and otorhi-
nolaryngological symptoms in one and multiple occa-
sions without anyone asking for an HIV detection test.
(Table 1).
In our opinion, the explanation of this phenomenon
go es over the simple knowledge of the diagnosis criterions
and lies on the fact that some professionals go on having
queries about an adequate performance. The HIV infec-
tion was treated in a different way from other infections
during the 80s and 90s, because of the consequences of
marginalization and the impact it had, which has been
known as “AIDS excepcionalism” [6,7]. Since then this
approach has changed a lot but it has probably not been
correctly conveyed to professionals, even in the intern-
ship formation. Since 2005, at least, there exists argu-
ments against this uniqueness [6,7]: there exists HART
which is not used due to delayed diagnosis, a sufficient
mobimortality reduction and mother-child transmission
[8]. In 2006 the specific Guideline CDC made upwards
recommendations to increase the offer to these HIV-test
in homosexual, IV drug users, p eop le with a high number
of couples or immigrants from countries with the high
prevalence [9]. All publications, advices and recommen-
dations, from then, went in the same direction : to support
the HIV test active offer not only for the diagnosis but to
propose treatment [10-12]. In Spain there are no doubts
Copyright © 2013 SciRes. WJA