 International Journal of Otolaryngology and Head & Neck Surgery, 2013, 2, 165-173 http://dx.doi.org/10.4236/ijohns.2013.25036 Published Online September 2013 (http://www.scirp.org/journal/ijohns) Adenoid Cy s tic Carci noma of the H ead and Neck: Epidemiology and Predictors of Prognosis Daniel Monteiro1*, João Lino1, Teresa Bernardo1, João Fernandes2, Eurico Monteiro2 1Department of Otorhinolaryngology and Head and Neck Surgery, Saint Antonio Hospital, Porto, Portugal 2Department of Otorhinolaryngology and Head and Neck Surgery, Portuguese Institute of Oncology, Porto, Portugal Email: orietnomdaniel@gmail.com Received June 8, 2013; revised July 3, 2013; accepted July 23, 2013 Copyright © 2013 Daniel Monteiro et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. ABSTRACT Objectives: The biologic behavior of the adenoid cystic carcinoma (ACC) and the factors predicting outcome for these tumors are still poorly understood. Our objective is to analy ze the predictin g factors and the value of differen t treatment possibilities, since none sole treatment has been stan dardized. Methods: A retrospective analysis of the epidemiologic, clinical and histologic aspects of ACC, as well as treatment options and o ther pr ognostic factors of all the cases of ACC of the head and neck treated at this In stitution were analyzed. From 1974 until 2011, 152 patien ts were diagnosed with ACC and treated at the Portuguese Institute of Oncology (Porto Centre). Main outco me measures: overall survival, local recurrence and distant metastasis were calculated by the Kaplan-Meier method. Factors predictive of outcome were identified by univariate and multivariate analysis. Results: The mean age at diagnosis was 55.8 years (range, 19 - 83 years). Incidence was higher in the female population, with a female to male ratio of 1.7:1 respectively. The primary tumor location was hard palate and submandibular region in 56 cases, 28 in each location (24.6%), parotid gland (17 cases, 14.9%) and oral cavity excluding palate (16 cases, 14%).Distributions according to T stage were: T1 (29.8%); T2 (30.7%); T3 (17.5%); T4 (22%). The overall 1-year, 5-year and 10-year survival for all patients were 94.6%, 60.5%, 41.6%, respectively. Conclusions: Univariate survival analysis revealed that age older than 60 years (p = 0.002), solid histologic subtype (p = 0.042), advanced clinical stage (p < 0.001) and the presence of perineural invasion (p = 0.036) were correlated with a poor survival. Multivariate analysis confirmed that age and advanced clinical stage were worst independent predicators of overall survival as well as perineural invasion for local recurrence and distant metastasis. In our analysis, radiotherapy did not have a relevant impact on survival, except in cases of solid histologic subtype. To analyze distant metastatic capacity, long term follow-up was necessary, since distant metastasis way occurs even after 10 years, which has the case with 4 patients. Keywords: Adenoid Cystic Carcinoma; Head and Neck Cancer; Prognostic Factors 1. Introduction Adenoid cystic carcinoma (ACC), also known as cylin- droma, a rare adenocarcinoma arising within secretory glands, occurs mainly in the minor salivary glands of the palate, and in the major glands [1-5]. Besides the oral ca- vity, other locations may be affected in accordance to the anatomical distribution of the minor salivary glands, as for example nasal cavity, paranasal sinus, pharynx, eso- phagus, larynx, tracheobronchial tree, eye and external auditory canal [1,3]. ACC of the head and neck is re- sponsible for 0.5% - 1% of malignancies in this area and for 7.5% - 10% of salivary gland tumors [1-3,6]. In fact, the largest epidemiological study that included 2611 cases from European countries, found an ACC (ICD-0-2 Code 8200) inciden ce of 0.5% [2]. The biological behavior of ACC of head and neck is clinically represented by a slow and indolent growth gen- erally in sub mucosal localization, making these tumors hard to diagnose [1,4,6]. It is frequ ently associated w ith a late recurrence rate and distant metastasis, especially to the lungs, and they are associated with poor progno sis [1, 3,6]. Histologically, three subtypes of ACC (cribriform, tu- bular and solid) have been described, with tubular sub- types having a better prognosis in contrast to solid pat- tern histolo gy [ 1,3]. Standard treatment for patients diagnosed with ACC is surgical, in some cases associated with radiotherapy, al- *Corresponding author. C opyright © 2013 SciRes. IJOHNS  D. MONTEIRO ET AL. 166 though the benefit of this last option has not been un- equivocally proven [1,3]. Radiotherapy has been consid- ered for patients with criteria of poor prognosis, as per- ineural invasion, positive margins and advanced stages [7,8]. Albeit ACC has been the subject of many epidemiol- ogical studies on several populations, predictive and prognostic factors in this type of cancer are scarce. The objective of this retrospective study was to characterize epidemiologically your population of patients in a tertiary cancer-institution, and analyze factors involved in local control, treatment failure, distant metastasis and other prognostic variables associated with overall survival. 2. Material and Methods 2.1. Patients A retrospective analysis including all patients with ACC diagnosed and treated at the Oporto Oncologic Institute between 1974 and 2011 was conducted. This study was approved by the Institution’s Ethics Committee. Of the 152 ACC patients initially identified, 38 were excluded due to insufficien t clinical data (Figure 1). Demographic and clinical in formation (age, gender, initial symptoms and its duration, histologic subtype, location of primary, perineural invasion, distant metastasis, staging and treat- ment options) was obtained from the remaining 114 pa- tients. Anatomical distribution of these tumors was grouped as tumors with origin in minor or major glands, though different locations were registered. Staging was per- formed in accordance with the 2010 American Joint Committee on Cancer (AJCC) staging system. In some cases, there were more than one histologic subtype in the tumor, but the characterization has been made according to the most predominant subtype. Margin statuses after surgery were not analyzed in all patients due to in suffi- cient information in clinical charts. Only 101 patients submitted to surgery followed or not by radiotherapy were subject to further analysis. Primary and secondary end-points analyzed were overall survival (OS), defined as the time from diagnosis until death or last clinical visit, and disease free survival, defined as the time-to-locore- gional recurrence (TTR), or time-to-distant metastasis (TTM) determined as the time interval, in months, be- tween diagnosis and local recurrence or distant metasta- sis. 2.2. Statistical Analysis Global analysis included only 101 patients, those that were submitted to surgery followed or not by radiother- apy. Tertiles of age at diagnosis were used for analyses. For time-to-event analyses, univ ariate Kaplan-Meier with Submitted to Surgery or Surgery followed by Radiotherapy =101 cases Hospital Database (1974-2011) 152 cases of A CCH Cases analyzed for clinical and pathologic variations N = 114 13 cases excluded due to having been submitted to exclus ively QT, RT, symptomatic or refused treatment 38 cas es ex cluded du e to insufficient data Figure 1. Diagram depicting the analysis criteria of the population. log-rank tests and multivariate Cox proportional hazards model were used, to identify predictors of overall survi- val, local recurrence and distant metastasis. Hazard ratios (HR) and 95% confidence intervals (CIs) were used for estimating the association between clinical and patho- logical characteristics with each of the outcomes of in- terest. Selection of variables to include in the multivari- ate model was submitted to empirical evaluation through univariate analysis. Variables with p-values lower than 0.10 on univariate analysis were included in the multi- variate model. SPSS version 17 was used for statistical analysis. 3. Results 3.1. Clinical Features Table 1 outlines the clinical characteristics of the 114 pa- tients. Mean age at diagnosis was 55.8 years (range 19 to 83 years). The incidence in the female gender was higher than in men, 63.2% and 36.8% respectively. The main symptom at the time of diagnosis was a no- dular mass (52.6%), followed by pain associated to a no- dule (18.4%), nasal symptoms (14%) (nasal obstruction, hemorrhagic rhinorrhea). Other symptoms less frequent were dyspnea, odynophagia, otalgia, facial paralysis and hearing impairment. Median time elapsed between onset of symptoms and diagnosis was 10 months, with a minimum of 0 months and a maximum of 144 months. Eighty one percent of the patients were diagnosed in the first 24 months after- symptom initiation. ACC was diagnosed less frequently in major salivary glands (39.5%) than in anatomic loca- tions where minor salivary glands are represented ( 60 .5 %) . The most common location was the oral cavity with 44 cases (38.6%), 28 cases of which in the hard palate. The Copyright © 2013 SciRes. IJOHNS  D. MONTEIRO ET AL. 167 second most frequent location was the submandibular gland with 28 cases (24.6%), followed by the parotid gland (17 cases, 14.9%), the paranasal sinus (12 cases, 10.5%) and the larynx (7 cases, 6.1%). Other locations seldom involved include the parapharyngeal space, the scalp, the external auditory meatus and the nasopharynx (Table 1). 3.2. Pathologic Characteristics The pathologic characteristics of the ACC resected are outlined in Table 2. Histologic sub classification was only determined in 68 patients, 29.4% were predomi- nantly tubular, 44.1% primarily cribriform and 26.5% mainly solid. Sixty one patients (53.5%) had perineural invasion of Table 1. Population characteristics. Cases Percent Age <52 years 40 35.1 52 until 64 years 32 28.1 >64 years 42 36.8 Gender Female 72 63.2 Male 42 36.8 Initial symptom Nodular mass 60 52.6 Nodular mass and pain 21 18.4 Nasal symptoms 16 14.0 Dyspnea and dysphonia 6 5.3 Odynophagia 4 3.5 Cervical adenopathy 2 1.8 Otalgia 2 1.8 Facial Paralysis a nd nodular mass 2 1.8 Hipoacusis 1 0.9 Location Hard Palate 28 24.6 Submandibular 28 24.6 Parotid 17 14.9 Sublingual glands and minor glands of the oral cavity 16 14.0 Paranasal sinus 12 10.5 Larynx 7 6.1 Others (scalp 2, p a rapharyngeal space 2, external acoustic meatus 1, nasopharynx 1) 6 5.3 Table 2. Pathologic chara cterist ics. Cases Percent Histology Tubular 20 29.4 Cribriform 30 44.1 Solid 18 26.5 Total 68 100.0 Invasion Perineural invasion 61 53.5 No invasion 48 42.1 No Perineural invasion but with other type of invasion (lymphatic, vascular, bone) 5 4.4 Total 114 100 which 32 cases had exclusive perineural invasion and in the remaining, vascular (18 cases), lymphatic (18 cases) and bone invasion (11 cases) were also present. Perineu- ral invasion was present more frequently in tumors of major salivary glands (30/43) than in minor glands (28/ 58) a finding with statistical significance (p = 0.031). 3.3. Staging TNM classification and stages can be observed in Table 3. Of all tumors, 10.5% had regional metastasis and only 6.1% had distant metastases at the time of diagnosis (lungs in 5 cases and bone in 1 case). Approximately half of the patients were diagnosed at an initial stage (I and II). 3.4. Treatment The distribution of patients according to treatment op- tions is shown in Ta ble 4. Of the 114 patients, 4 refused treatment and 9 were considered inoperable and were selected for supportive care or palliative treatment with radiotherapy or chemotherapy. These 13 patients were excluded from further analysis. Of the 101 patients sub- mitted to surgery, 58 cases were proposed for subsequent radiotherapy (RT). Many factors interfered with the deci- sion of post-operative RT such as the surgeon’s option, location, presence of positive margins and perineural invasion. The average time from diagnosis until surgery was 2.3 mont h s . 3.5. Univariate and Multivariate Survival Analysis for Overall Survival Univariate analysis of the clinical, epidemiologic and pathologic variables analyzed for overall survival (Table 5) revealed that older patient’s had a worse outcome. Copyright © 2013 SciRes. IJOHNS 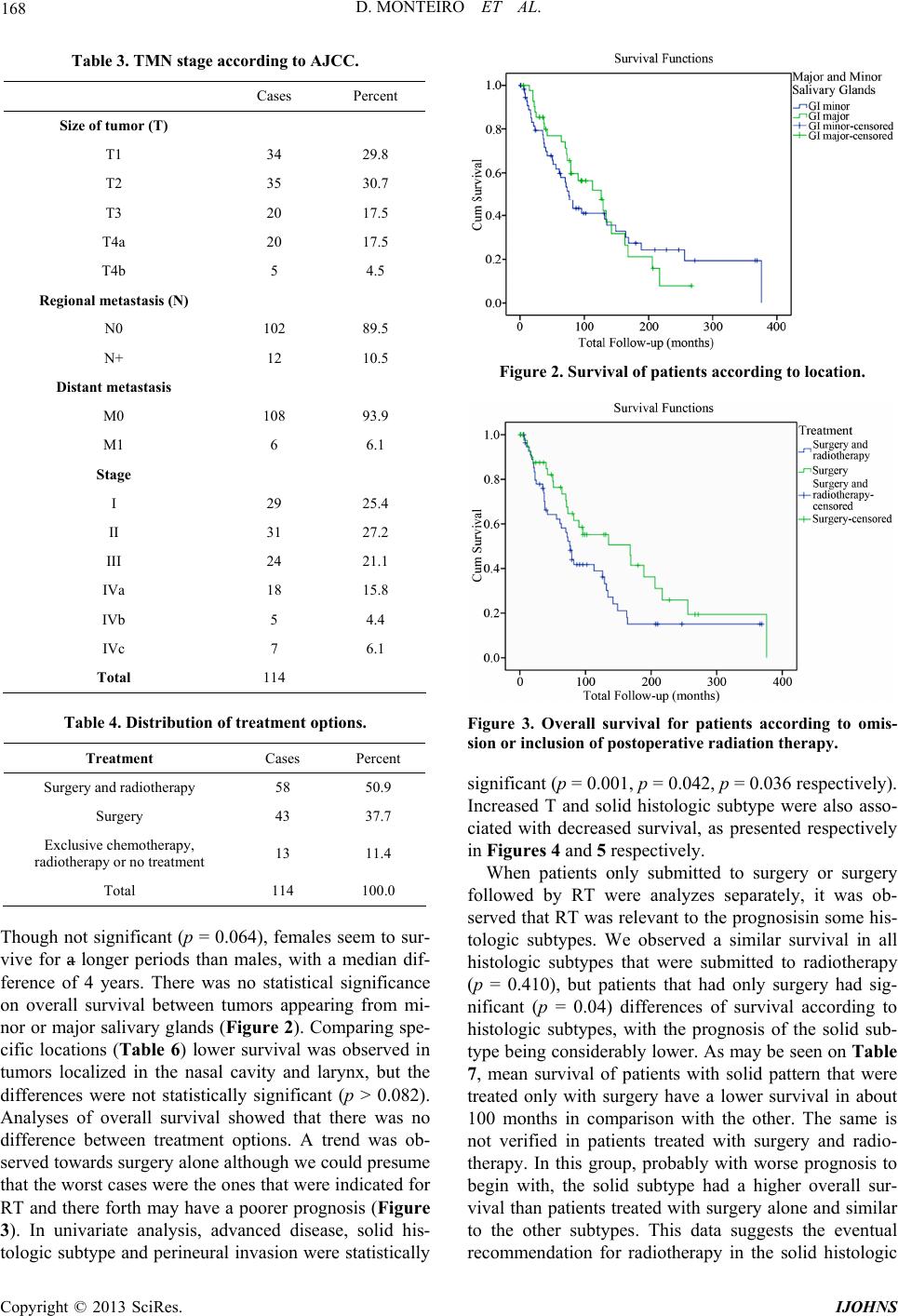 D. MONTEIRO ET AL. 168 Table 3. TMN stage according to AJCC. Cases Percent Size of tumor (T) T1 34 29.8 T2 35 30.7 T3 20 17.5 T4a 20 17.5 T4b 5 4.5 Regional metastasis (N) N0 102 89.5 N+ 12 10.5 Distant metastasis M0 108 93.9 M1 6 6.1 Stage I 29 25.4 II 31 27.2 III 24 21.1 IVa 18 15.8 IVb 5 4.4 IVc 7 6.1 Total 114 Table 4. Distribution of treatment options. Treatment Cases Percent Surgery and radiotherapy 58 50.9 Surgery 43 37.7 Exclusive chemotherapy, radiotherapy or no treatment 13 11.4 Total 114 100.0 Though not significant (p = 0.064), females seem to sur- vive for a longer periods than males, with a median dif- ference of 4 years. There was no statistical significance on overall survival between tumors appearing from mi- nor or major salivary glands (Figure 2). Comparing spe- cific locations (Table 6) lower survival was observed in tumors localized in the nasal cavity and larynx, but the differences were not statistically significant (p > 0.082). Analyses of overall survival showed that there was no difference between treatment options. A trend was ob- served towards surgery alone although we could presume that the worst cases were the ones that were indicated for RT and there forth may have a poorer prognosis (Figure 3). In univariate analysis, advanced disease, solid his- tologic subtype and perineural invasion were statistically Figure 2. Survival of patients according to location. Figure 3. Overall survival for patients according to omis- sion or inclusion of postoperative radiation therapy. significant (p = 0.001, p = 0.042, p = 0.036 respectively). Increased T and solid histologic subtype were also asso- ciated with decreased survival, as presented respectively in Figures 4 and 5 resp ectively. When patients only submitted to surgery or surgery followed by RT were analyzes separately, it was ob- served that RT was relevant to the prognosisin some his- tologic subtypes. We observed a similar survival in all histologic subtypes that were submitted to radiotherapy (p = 0.410), but patients that had only surgery had sig- nificant (p = 0.04) differences of survival according to histologic subtypes, with the prognosis of the solid sub- type being considerably lower. As may be seen on Table 7, mean survival of patients with solid pattern that were treated only with surgery have a lower survival in about 100 months in comparison with the other. The same is not verified in patients treated with surgery and radio- therapy. In this group, probably with worse prognosis to begin with, the solid subtype had a higher overall sur- vival than patients treated with surgery alone and similar to the other subtypes. This data suggests the eventual recommendation for radiotherapy in the solid histologic Copyright © 2013 SciRes. IJOHNS 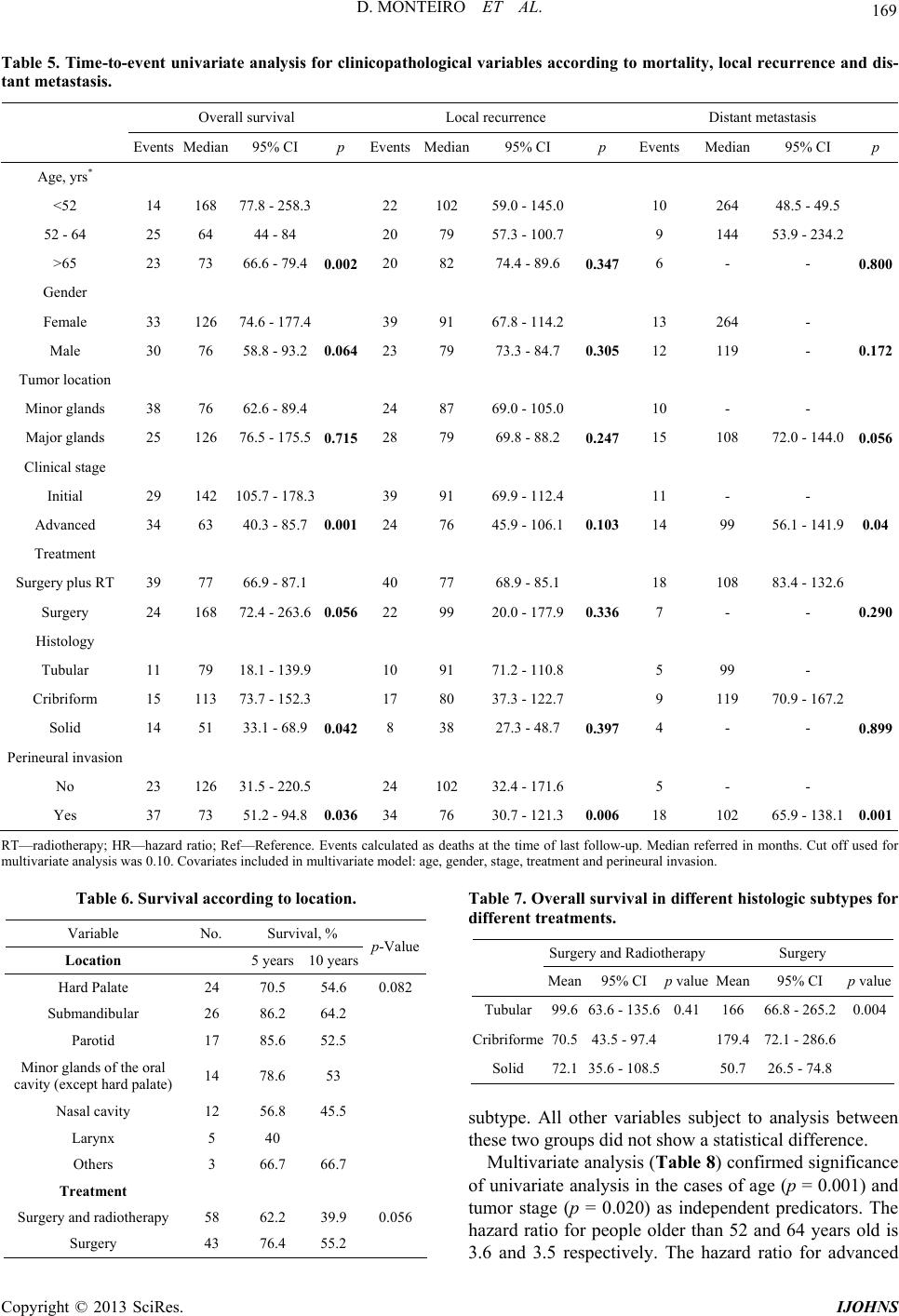 D. MONTEIRO ET AL. Copyright © 2013 SciRes. IJOHNS 169 Table 5. Time-to-event univariate analysis for clinicopathological variables according to mortality, local recurrence and dis- tant metastasis. Overall survival Local recurrence Distant metastasis Events Median95% CI p EventsMedian95% CI p Events Median 95% CI p Age, yrs* <52 14 168 77.8 - 258.3 22 102 59.0 - 145.0 10 264 48.5 - 49.5 52 - 64 25 64 44 - 84 20 79 57.3 - 100.7 9 144 53.9 - 234.2 >65 23 73 66.6 - 79.4 0.002 20 82 74.4 - 89.6 0.347 6 - - 0.800 Gender Female 33 126 74.6 - 177.4 39 91 67.8 - 114.2 13 264 - Male 30 76 58.8 - 93 .2 0.064 23 79 73.3 - 84.7 0.305 12 119 - 0.172 Tumor location Minor glands 38 76 62.6 - 89.4 24 87 69.0 - 105.0 10 - - Major glands 25 126 76.5 - 175.5 0.715 28 79 69.8 - 88.2 0.247 15 108 72.0 - 144.00.056 Clinical stage Initial 29 142 105.7 - 178.3 39 91 69.9 - 112.4 11 - - Advanced 34 63 40.3 - 8 5.7 0.001 24 76 45.9 - 106.10.103 14 99 56.1 - 141.90.04 Treatment Surgery plus RT 39 77 66.9 - 87.1 40 77 68.9 - 85.1 18 108 83.4 - 132.6 Surgery 24 168 72.4 - 263.6 0.056 22 99 20.0 - 177.90.336 7 - - 0.290 Histology Tubular 11 79 18.1 - 139.9 10 91 71.2 - 110.8 5 99 - Cribriform 15 113 73.7 - 152.3 17 80 37.3 - 122.7 9 119 70.9 - 167.2 Solid 14 51 33.1 - 68.9 0.042 8 38 27.3 - 48.7 0.397 4 - - 0.899 Perineural invasion No 23 126 31.5 - 220.5 24 102 32.4 - 171.6 5 - - Yes 37 73 51.2 - 94.8 0.036 34 76 30.7 - 121.30.006 18 102 65.9 - 138.10.001 RT—radioth erapy; HR—hazard rati o; Ref—Reference. Ev ents calculated as deaths at the ti me of last follo w-up. Median referred in months. Cut off used for multivaria te analysis was 0.10. Covariates included in multivariate model: age, gender, stage, treatment and pe rineural inva sion. Table 6. Survival according to location. Variable No. Survival, % Location 5 years 10 yearsp-Value Hard Palate 24 70.5 54.6 0.082 Submandibular 26 86.2 64.2 Parotid 17 85.6 52.5 Minor glands of the oral cavity (except hard palate) 14 78.6 53 Nasal cavity 12 56.8 45.5 Larynx 5 40 Others 3 66.7 66.7 Treatment Surgery and radiotherapy 58 62.2 39.9 0.056 Surgery 43 76.4 55.2 Table 7. Overall survival in different histologic subtypes for different treatments. Surgery and Radiotherapy Surgery Mean95% CI p value Mean 95% CI p value Tubular99.663.6 - 135.60.41 166 66.8 - 265.20.004 Cribriforme70.543.5 - 97.4 179.4 72.1 - 286.6 Solid 72. 135.6 - 108.5 50.7 26.5 - 74.8 subtype. All other variables subject to analysis between these two groups did not show a statistical difference. Multivariate analysis (Table 8 ) confirmed significance of univariate analysis in th e cases of age (p = 0.001) an d tumor stage (p = 0.020) as independent predicators. The hazard ratio for people older than 52 and 64 years old is 3.6 and 3.5 respectively. The hazard ratio for advanced  D. MONTEIRO ET AL. 170 Table 8. Multivariate analysis with predictive variables for mortality, local recurrence and distant metastasis. Overall survival Local recurrence Distant metastasis HR 95% CI p HR 95%CI p HR 95% CI p Age, yrs * <52 Referent Referent Referent 52 - 64 3.6 1.7 - 7.6 0.0011.4 0.7 - 2.8 0.318- - - >65 3.5 - 0.0021.7 0.8 - 3.4 0.138- - - Gender Female Referent Referent Referent - - Male 1.2 0.7 - 2.1 0.4501.1 0.6 - 1.9 0.864 Tumor location Minor glands Referent 1.3 1.7 - 2.4 1.6 0.7 - 3.9 0.293 Major glands 1.0 0.6 - 1.8 0.987Referent 0.493Referent Clinical stage Initial Referent 1.2 1.8 Advanced 2.0 1.1 - 3. 6 0.020Referent 0.7 - 2.4 0.493Referent 0.8 - 4.3 0.185 Treatment Surgery plus RT Referent 1. 0 Surgery 1.0 0.5 - 1 .7 0.864Referent 0.6 - 1.9 0.9 49Referent - - Histology Tubular Cribriform - - - Solid - - - - - - Perineural invasion No Referent 2.1 1.1 - 3.9 0.028Referent Yes 1.6 0.9 - 2.8 0.107Referent 3.5 1.2 - 10.3 0.025 Cut off used for multivariate analysis was 0.10. Covariates included in multivariate model: Age, gender, stage, treatment, perineural invasion. Histology sub- types not included due to low number. Figure 4. Overall survival according to T. Figure 5. Survival rates according to histologic type (gradin g). Copyright © 2013 SciRes. IJOHNS  D. MONTEIRO ET AL. 171 stage is 2.0 with a 95% confidence interval of 1.1 to 3.6. 3.6. Follow-Up and Global Survival Rates No definite policy on follow-up was observed, but the median follow-up period was 90 months (95% CI 42.7 - 137.3). The overall su rvival rates were 68.2%, 45.7% and 19.4% for 5 years, 10 years and 20 years respectively. The disease free survival rates for 5 years and 10 years was 52.9% and 34.4%.Surv ival at 5 and 10 years dep end- ing on variables (gender, perineural invasion, stage and treatment) and the results can be observed in Table 9. 3.7. Univariate and Multivariate Survival Analysis of Local Recurrence and Distant Metastasis Following the initial treatment, four patients had persis- tent disease and have been submitted to chemotherapy or supportive treatment. Thirty-five patients (34.7%) had lo- cal recurrence after a mean time of 42.2 months. Patients were selected for palliative treatment (5 cases), chemo- therapy (5 cases) and surgery with or without radiother- apy (25 cases) and, survival following treatment was 51.6 months, 40.4 months and 63.4 months, respectively. These results suggest that chemotherapy has no indica- tion in the recurrence of ACC and the treatment should be secondary surgery followed or not by radiotherapy when possible. Twenty five patients (24.8%) had distant metastasis after a mean time of 67.6 months (median of 48 months). Twenty one of these patients had lung metastasis) and in 5 of these, there were also metastasis to other locations namely, liver (2 cases), bone, kidney and brain with one each. In the remaining 4 patients, 1 had bone metastasis, 1 had liver metastasis and 2 had both these locations. Even though distant metastasis was observed, patients had prolonged survival after their identification, with a mean time survival of 40 months (range 3 - 133 months). Survival times were similar in spite of different metasta- sis location. The 5 patients that had metastasis in more than 1 location had a mean survival time of 61 months. When comparing treatment of distant metastasis, secon- dary surgery followed or not by radiotherapy prolonged lifetime for an average of 70 months, while only chemo- therapy prolonged life for 36 months and patients only treated symptomatically survived on an average of 20 months. This finding supports the need for treatment of distant metastasis with surgery followed or not by radio- therapy. Univariate and multivariate analyses for local recur- rence and distant metastasis revealed that perineural in- vasion was significantly associated with local recurrence rate and distant metastasis (Tables 5 and 7). In univariate analysis, advanced disease was statistically (p = 0.04) as- Table 9. Survival at 5 and 10 years (gender, perineural in- vasion, clinical stage, treatment). Variable Survival, % 5 years 10 years Gender Female 72.1 52.4 Male 62.7 35.9 Perineural invasion Yes 58.2 40.5 No 77.9 52.4 Clinical stage I and II 79.3 63.3 III and IV (a e b) 53.1 23.3 Treatment Surgery + RT 62.2 39.0 Surgery 76.4 55.2 sociated to a poorer prognosis with earlier distant me- tastasis. Distant metastasis developed in all histologic subtypes with no statistical difference between them, but is important to note that the solid histologic subtype re- curs much earlier than the other 2 subtypes of ACC (me- dian 38 mont h s ). The main reason for death in these patients was local- recurrence and distant dissemination, but location of the primary was not relevant neither for local recurrence nor for distant metastasis. Local recurrence occurred in 7 pa- tients after 5 years and in 2 patients after 10 years. Con- sidering distant metastasis 12 cases occurred after 5 years and 2 after 10 years. 4. Discussion There are doubts that the prevalence of ACC is gender related, none the less some studies claim a higher fre- quency and better prognosis in the female population, has was found in our series [1,2,4,9,10]. According to the literature available, there is a great variability on the age of onset, from 10 to 99 years, with more frequency above the age of 64 years, which is coherent with our findings. [2,4,6,11]. Symptoms in [12] most cases are unspecific and vary in accordance to the location of the tumor [6]. Manifestations in cases of oral and major salivary glands tumors are nodular mass, often associated with pain, which is usually related to perineural invasion [1]. The most frequent location is the hard palate (34%) due to the greater number of minor salivary glands, followed by the submandibular and the parotid glands, concordant to our series [4,8,10]. The median time from the first complain until diagno- Copyright © 2013 SciRes. IJOHNS  D. MONTEIRO ET AL. 172 sis was 10 months, nonetheless, as shown in our findings, some cases may take several years to be diagnosed due to slow and indolent growth pattern of these tumors. In spite of delayed diagnosis, in our series, patients rarely had regional or distant metastasis at the time of diagnosis, as reported by other investigators [13]. It was verified that tubular and cribriform subtypes had a greater time interval between first symptom and diagnosis than the so lid subtype, probably due to a faster growth pattern or a greater invasive capacity. Tubular subtype is expected to have a better prognosis, although our data demonstrated a greater median survival time for the cribriform subtype [1,3,4,14]. This aspect may be at- tributed to different percentages of the histologic sub- types in the tumors, emphasizing the importance of a cor- rect histologic classification. Different prognosis and be- havior patterns have been referred between histologies, however subtypes are often not registered by pathologists. Cribriform subtype was the most common in our series (44.1%), coherent with the literature, that states that this subtypeis responsible for 50% of the cases and the tubu- lar and the solid patterns for 25% each [1,3,13]. Our data suggests that all cases of solid histologic subtype should be submitted to radiotherapy, due to the finding of simi- lar life expectancy in patients of different histologic sub- types, treated with surgery followed by radiotherapy as opposed to patients treated exclusively with surgery, which had differences of 100 mont h s. The most important prognostic factors of poor overall survival referred in literature are advanced initial stage, advanced age, histologic subtype (solid), location and in- complete surgical resection [1-3,12 ,14]. We found in our series that the first two were statistically significant (p = 0.001 and p = 0.002 respectively). Concerning the loca- tion, a large overall survival difference was observed be- tween sites, namely for the larynx and paranasal sinus with a poorer survival, which results are coherent with the study of Ciccolallo, although in our series the results did not achieve statistical significance due to the scarce number of cases (Table 6). Accepted factors predicting recurrence are tumor stage at the time of diagnosis, posi- tive surgical margins and perineural invasion [2,3,8,12]. Perineural invasion was observed in 53.5% of our pa- tients, confirming the reported neurotropism of this tu- mor [1,3]. Our study emphasizes the importance of per- ineural invasion, which was considered an independent prognostic factor for all outcomes. In our series other re- ferred prognostic factors did not achieve significance value due maybe to small amount of patients analyzed. Our exclusion of some cases (152-to-101) was made in an attempt to eliminate in sufficient data and selection bias for treatment modalities, since patients with ad- vanced or unresectable disease tend to be treated with palliative measures. Our findings suggest that th ere is no benefit in submitting patients to post-operative radiother- apy (p = 0.056) which is coherent with the studies pub- lished by Silverman et al. (2004) e Chen A.M. et al. (2006), with the exception of patients with solid histolo- gic subtype [5,7,8,15]. The best treatment option is sur- gery with wide safe margins, with special attention to sub mucosal expansion, perineural and lympho-vascular in- vasion [3,6,8,12-14,16]. Chemotherapy in ACC has not been proved as beneficial [12]. Recurrence disease in our population (34.7%) was not as rare as described in the literature (10% - 20%) [3,11]. Concerning distant metastasis these may occur in 16% - 35% of the cases, which is similar to our results (2 7.7%) [3,13]. Distant metastasis are located predominantly in the lungs (78.6% in our series), in few patients in the liver and bones (21% each in our series) and rarely in the kidneys and brain (3.5% each) [1,3,4,6,12,14]. Tumor as- sociated survival was poor, with a 15 - 20 year prognosis inferior to 20% [1,7,1 7]. Du e to the tu moral behavior and the possibility of late recurrences and of distant metasta- sis after many years, it is important to have a longer fol- low-up peri od [1 3, 1 4,18]. 5. Conclusion In summary, increased age and advanced clinical stage were independent significant prognostic factors for over- all survival in our series. Perineural invasion was an in- dependent significant prognostic factor for local recur- rence and distant metastasis. Our study advises clinicians to request different subtype characterization from the pa- thologist, due to different growth patterns and survivals. We recommend radiotherapy only in patients with solid histologic subtypes. Our findings indicate that patients with local recurrence and/or distant metastasis survive longer if submitted to secondary surgery followed or not by radiotherapy, so we recommend salvage surgery for all possible cases. Multi-center studies are necessary in order to determine with certainty which are the b est treat- ment options. REFERENCES [1] D. C. Perez, F. A. Alves, I. N. Nishimoto, O. P. Almeida, et al., “Prognostic Factors in Head and Neck Adenoid Cystic Carcinoma,” Oral Oncology, Vol. 42, No. 2, 2006, pp. 139-146. [2] L. Ciccolallo, L. Licitra, G. Cantú, G. Gatta, et al., “Sur- vival from Salivary Glands Adenoid Cystic Carcinoma in European Population,” Oral Oncology, Vol. 45, No. 8, 2009, pp. 669-674. doi:10.1016/j.oraloncology.2008.10.010 [3] S. Chummun, N. R. McLean, C. G. Kelly, P. J. Dawas, et al., “Adenoid Cystic Carcinoma of the Head and Neck,” British Journal of Plastic Surgery, Vol. 54, No. 6, 2001, pp. 476-480. doi:10.1054/bjps.2001.3636 Copyright © 2013 SciRes. IJOHNS  D. MONTEIRO ET AL. Copyright © 2013 SciRes. IJOHNS 173 [4] N. M. Rodriguez, I. L. Berrocal, L. R. Alonso, O. A. Irimia, et al., “Epidemiology and Treatment of Adenoid Cystic Carcinoma of the Minor Salivary Glands: A Meta- Analytic Study,” Medicina Oral Patologia Oral y Cirugia Bucal, Vol. 16, No. 7, 2011, pp. 884-889. doi:10.4317/medoral.17200 [5] A. J. Khan, M. P. DiGiovanna, D. A. Ross, C. T. Sasaki, et al., “Adenoid Cystic Carcinoma: A Retrospective Cli- nical Review,” Radiation Oncology Investigations, Vol. 96, No. 3, 2001, pp. 149-158. [6] H. Wang, L. Xu and F. Li, “Subglottic Adenoid Cystic Carcinoma Mistaken for Asthma,” Journal of Zhejiang University Science B, Vol. 10, No. 9, 2009, pp. 707-710. doi:10.1631/jzus.B0920071 [7] A. M. Chen, M. K. Bucci, V. Weinberg, J. Garcia, et al., “Adenoid Cystic Carcinoma of the Head and Neck Treated by Surgery with or without Postoperative Ra- diotion Therapy: Prognostic Features of Recurrence,” In- ternational Journal of Radiation Oncology Biology Phys- ics, Vol. 66, No. 1, 2006, pp. 152-159. [8] N. G. Iyer, L. Kim, I. J. Nixon, F. Palmer, et al., “Fac- tores Predicting Outcome in Malignant Minor Salivary Gland Tumors of the Oropharynx,” Archives of Otolar- yngology—Head and Neck Surgery, Vol. 136, No. 12, 2010, pp. 1240-1247. [9] C. L. Ellington, M. Goodman, S. A. Kono, W. Grist, et al., “Adenoid Cystic Carcinoma of the Head and Neck: Inci- dence and Survival Trends Based on 1973-2007 Surveil- lance, Epidemiologym and End Resuls Data,” Cancer, Vol. 118, 2012, pp. 4444-4451. doi:10.1002/cncr.27408 [10] F. A. Oliveira, E. C. B. Duarte, C. T. Taveira, A. A. Máximo, et al., “Salivary Gland Tumor: A Review of 599 Cases in a Brazilian Population,” Head and Neck Pa- thology, Vol. 3, No. 4, 2009, pp. 271-275. doi:10.1007/s12105-009-0139-9 [11] R. Srivastava and N. Bhatia, “Adenoid Cystic Carcinoma of Larynx,” IJO & HNS, Vol. 49, No. 3, 1997, pp. 280- 281. [12] P. B. Zald, M. W. Weber and J. Schindler, “Adenoid Cy- stic Carcinoma of Subglotic Larynx: A Case Report and Review of the Literature,” Ear Nose Throat Journal, Vol. 89, No. 4, 2010, p. E27. [13] A. D. Negro, E. Ichihara, A. J. Tncani and A. Altemani, “Laryngeal Adenoid Cystic Carcinoma: Case Report,” São Paulo Medical Journal, Vol. 125, No. 5, 2007, pp. 295-296. doi:10.1590/S1516-31802007000500010 [14] E. Zvrko and M. Golubovic, “Laryngeal Adenoid Cystic Carcinoma,” Acta Otorhinolaryngologica Italica, Vol. 29, No. 5, 2009, pp. 279-282. [15] D. A. Silverman, T. P. Carlson, D. Khuntia, et al., “Role for Postoperative Radiation Therapy in Adenoid Cystic Carcinoma of the Head and Neck,” Laryngoscope, Vol. 114, No. 7, 2004, pp. 1194-1199. doi:10.1097/00005537-200407000-00012 [16] A. T. N. N. Alves, F. D. Soares, A. S. Junior, Medeiros, et al., “Carcinoma Adenóide Cístico: Revisão da Litera- tura e Relato de Caso Clínico,” Brasileiro de Patologia e Medicina Laboratorial, Vol. 40, 2004, pp. 421-424. [17] S. C. Lee and J. T. Johnson, “Salivary Glands Neo- plasms,” eMedicine Specialties, 2009. http://emedicine.medscape.com/article/852373-overview [18] www.cancer.net. http://www.cancer.net/patient/Cancer+Types/Adenoid+C ystic+Carcinoma?sectionTitle=Overview
|