A. D. P. Bankoff et al. / Open Journal of Preventive Medicine 3 (2013) 413-419
418
for group 1, taking into account the results presented,
they are able to enter and start physical activities to im-
prove the levels found, specifically weight, BMI, HR,
SBP and DBP.
[23,24] postulate that every adult individual should
accumulate at least 30 minutes of physical activity at
least 5 days a week, or if possible the entire week, of
moderate intensity, which can be performed continuously
or accumulated. However, the group of women consid-
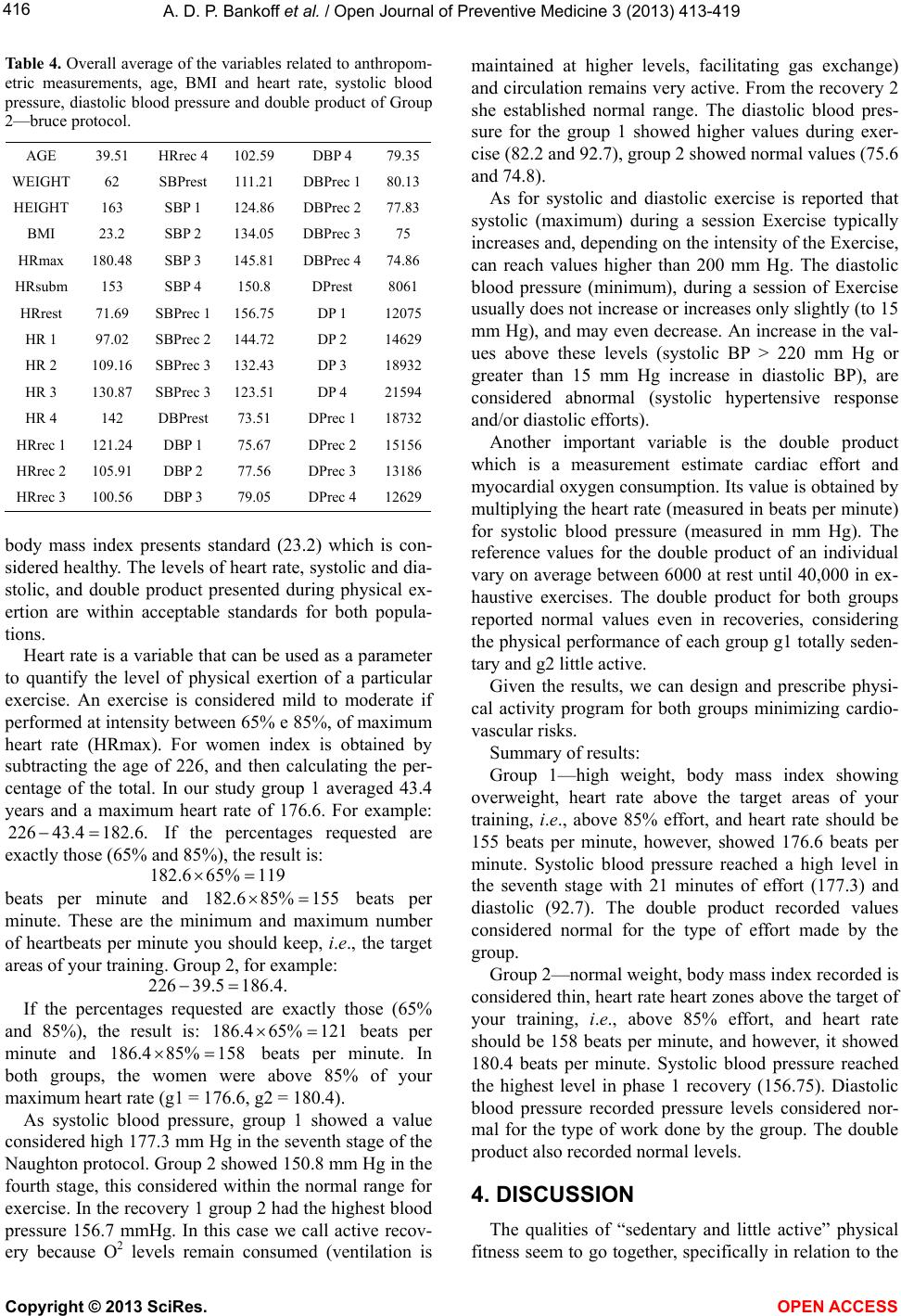
ered little active completed the stress test by the Bruce
protocol in the 4th stage with the following specifica-
tions: 4.2 mph, 16% incline, VO2Max 45, 13 METs and
already amounted 10 minutes of test performance, which
can be considered good for a exercise testing, consider-
ing the physical fitness of the “little active” women. The
women in group 1 that “self-declared” completely sed-
entary, completed the exercise testing by the Naughton
protocol on stage 7 with the following specifications: 02
Mph, 17.5% incline, VO2 Max 24.5, 7 METs and already
amounted 21 minutes of test performance and yet, for the
variables of the events of the cardiac cycle in accordance
with the statistical analysis, the results were not different
between groups 1 and 2 in most of the variables, as
shown in Table 2.
5. CONCLUSIONS
Participants in group 1 are able to particip ate in urgent
and need physical activity programs from the results
presented, specifically due to body weight, BMI, heart
rate and blood pres s ure;
Participants from group 2 require more days of prac-
tice of physical activities and longer hours to improve the
levels of heart rate and blood pressure;
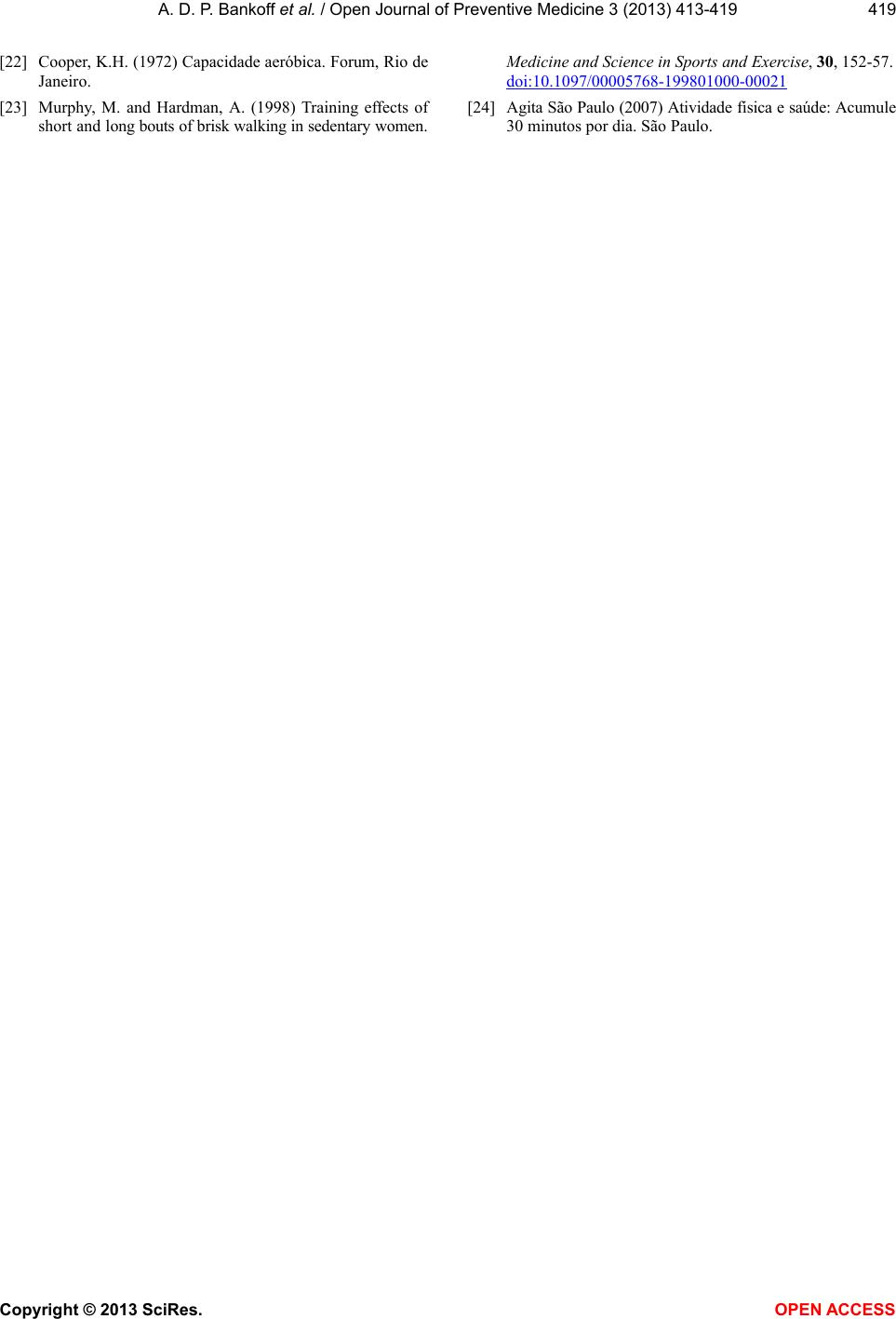
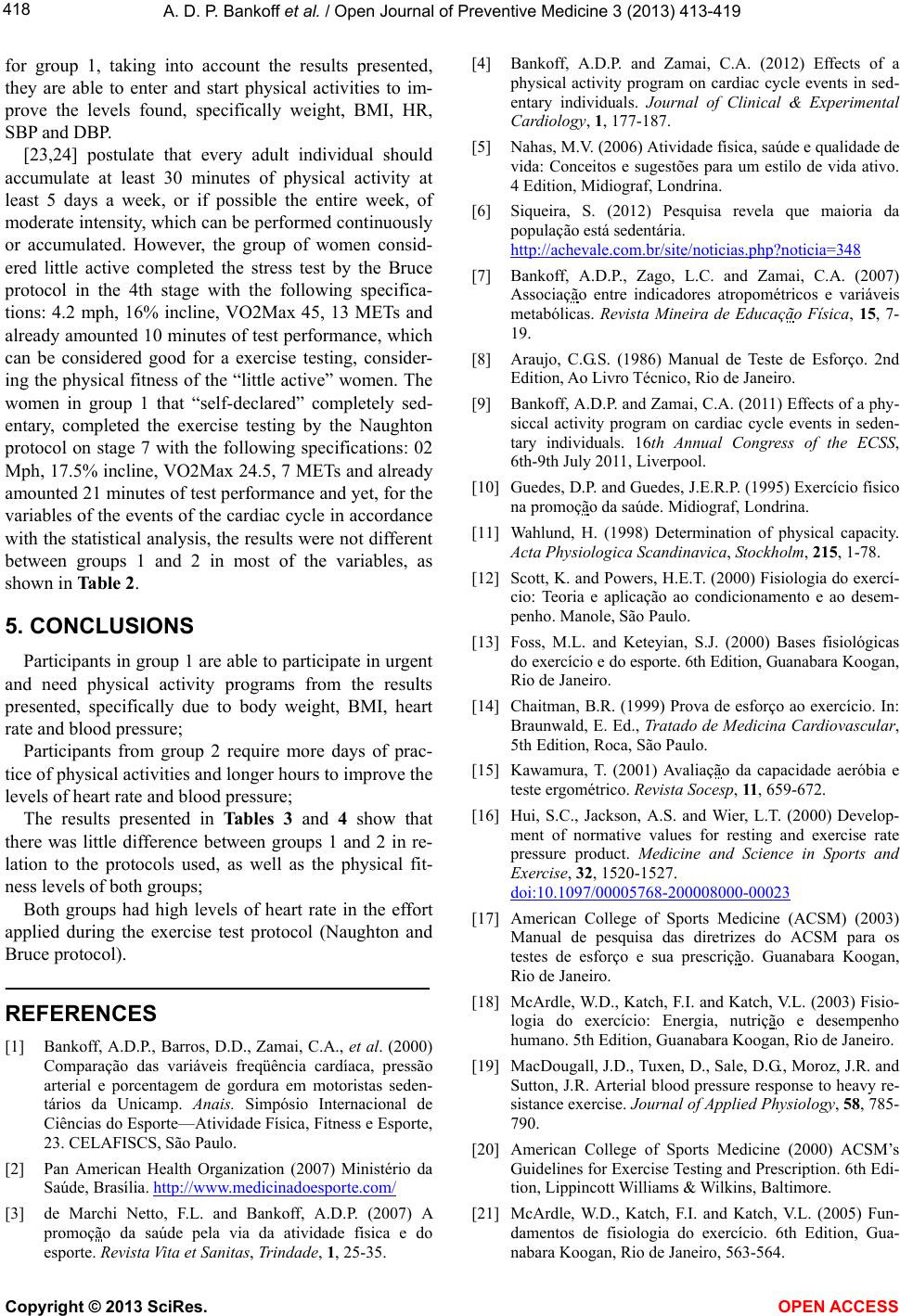
The results presented in Tables 3 and 4 show that
there was little difference between groups 1 and 2 in re-
lation to the protocols used, as well as the physical fit-
ness levels of both groups;
Both groups had high levels of heart rate in the effort
applied during the exercise test protocol (Naughton and
Bruce protocol).
REFERENCES
[1] Bankoff, A.D.P., Barros, D.D., Zamai, C.A., et al. (2000)
Comparação das variáveis freqüência cardíaca, pressão
arterial e porcentagem de gordura em motoristas seden-
tários da Unicamp. Anais. Simpósio Internacional de
Ciências do Esporte—Atividade Física, Fitness e Esporte,
23. CELAFISCS, São Paulo.
[2] Pan American Health Organization (2007) Ministério da
Saúde, Brasília. http://www.medicinadoesporte.com/
[3] de Marchi Netto, F.L. and Bankoff, A.D.P. (2007) A
promoção da saúde pela via da atividade física e do
esporte. Revista Vita et Sanitas, Trindade, 1, 25-35.
[4] Bankoff, A.D.P. and Zamai, C.A. (2012) Effects of a
physical activity program on cardiac cycle events in sed-
entary individuals. Journal of Clinical & Experimental
Cardiology, 1, 177-187.
[5] Nahas, M.V. (2006) Atividade física, saúde e qualidade de
vida: Conceitos e sugestões para um estilo de vida ativo.
4 Edition, Midiograf, Londrina.
[6] Siqueira, S. (2012) Pesquisa revela que maioria da
população está seden t á r ia .
http://achevale.com.br/site/noticias.php?noticia=348
[7] Bankoff, A.D.P., Zago, L.C. and Zamai, C.A. (2007)
Associação entre indicadores atropométricos e variáveis
metabólicas. Revista Mineira de Educação Física, 15, 7-
19.
[8] Araujo, C.G.S. (1986) Manual de Teste de Esforço. 2nd
Edition, Ao Livro Técnico, Rio de Janeiro.
[9] Bankoff, A.D.P. and Zamai, C.A. (2011) Effects of a phy-
siccal activity program on cardiac cycle events in seden-
tary individuals. 16th Annual Congress of the ECSS,
6th-9th July 2011, Liverpool.
[10] Guedes, D.P. and Guedes, J.E.R.P. (1995) Exercício físico
na promoção da saúde. Midiograf, Londrina.
[11] Wahlund, H. (1998) Determination of physical capacity.
Acta Physiologica Scandinavica, Stockholm, 215, 1-78.
[12] Scott, K. and Powers, H.E.T. (2000) Fisiologia do exercí-
cio: Teoria e aplicação ao condicionamento e ao desem-
penho. Manole, São Paulo.
[13] Foss, M.L. and Keteyian, S.J. (2000) Bases fisiológicas
do exercício e do esporte. 6th Edition, Guanabara Koogan,
Rio de Janeiro.
[14] Chaitman, B.R. (1999) Prova de esforço ao exercício. In:
Braunwald, E. Ed., Tratado de Medicina Cardiovascular,
5th Edition, Roca, São Paulo.
[15] Kawamura, T. (2001) Avaliação da capacidade aeróbia e
teste ergométrico. Revista Socesp, 11, 659-672.
[16] Hui, S.C., Jackson, A.S. and Wier, L.T. (2000) Develop-
ment of normative values for resting and exercise rate
pressure product. Medicine and Science in Sports and
Exercise, 32, 1520-1527.
doi:10.1097/00005768-200008000-00023
[17] American College of Sports Medicine (ACSM) (2003)
Manual de pesquisa das diretrizes do ACSM para os
testes de esforço e sua prescrição. Guanabara Koogan,
Rio de Janeiro.
[18] McArdle, W.D., Katch, F.I. and Katch, V.L. (2003) Fisio-
logia do exercício: Energia, nutrição e desempenho
humano. 5th Edition, Guanabara Koogan, Rio de Janeiro.
[19] MacDougall, J.D., Tuxen, D., Sale, D.G., Moroz, J.R. and
Sutton, J.R. Arterial blood pressure response to heavy re-
sistance exercise. Journal of Applied Physiology, 58, 785-
790.
[20] American College of Sports Medicine (2000) ACSM’s
Guidelines for Exercise Testing and Prescription. 6th Edi-
tion, Lippincott Williams & Wilkins, Baltimore.
[21] McArdle, W.D., Katch, F.I. and Katch, V.L. (2005) Fun-
damentos de fisiologia do exercício. 6th Edition, Gua-
nabara Koogan, Rio de Janeiro, 563-564.
Copyright © 2013 SciRes. OPEN A CCESS