C. K. CHAI ET AL.
Copyright © 2013 SciRes. IJOHNS
159
inadequate to detect tumour recurrence in this context.
Malignancy is another main concern, which makes long-
term follow-up necessary, with the risk of malignant
transformation ranging from 5% to 21% as well as the
mean duration of 52 months to develop carcinoma, re-
ported in many other literatures [3,7,13]. Currently there
are no universal guidelines for follow-up regime after
surgery. Nevertheless, some authors had suggested for
quarterly follow-up in the first two years, six monthly in
the subsequent two years and yearly thereafter [3]. In
other words, long-term follow up is mandatory and ad-
herence to follow-up should always be emphasized to all
patients [10].
5. Conclusion
Endoscopic medial maxillectomy is a well-accepted ap-
proach in treating inverted papilloma. Nevertheless, open
surgery still plays an important role in extensiv e diseases
and in cases of malignancy. Unilateral nasal obstruction
is the most important symptom. Repeated pre-operative
biopsy or perhaps a frozen section of intraoperative biop-
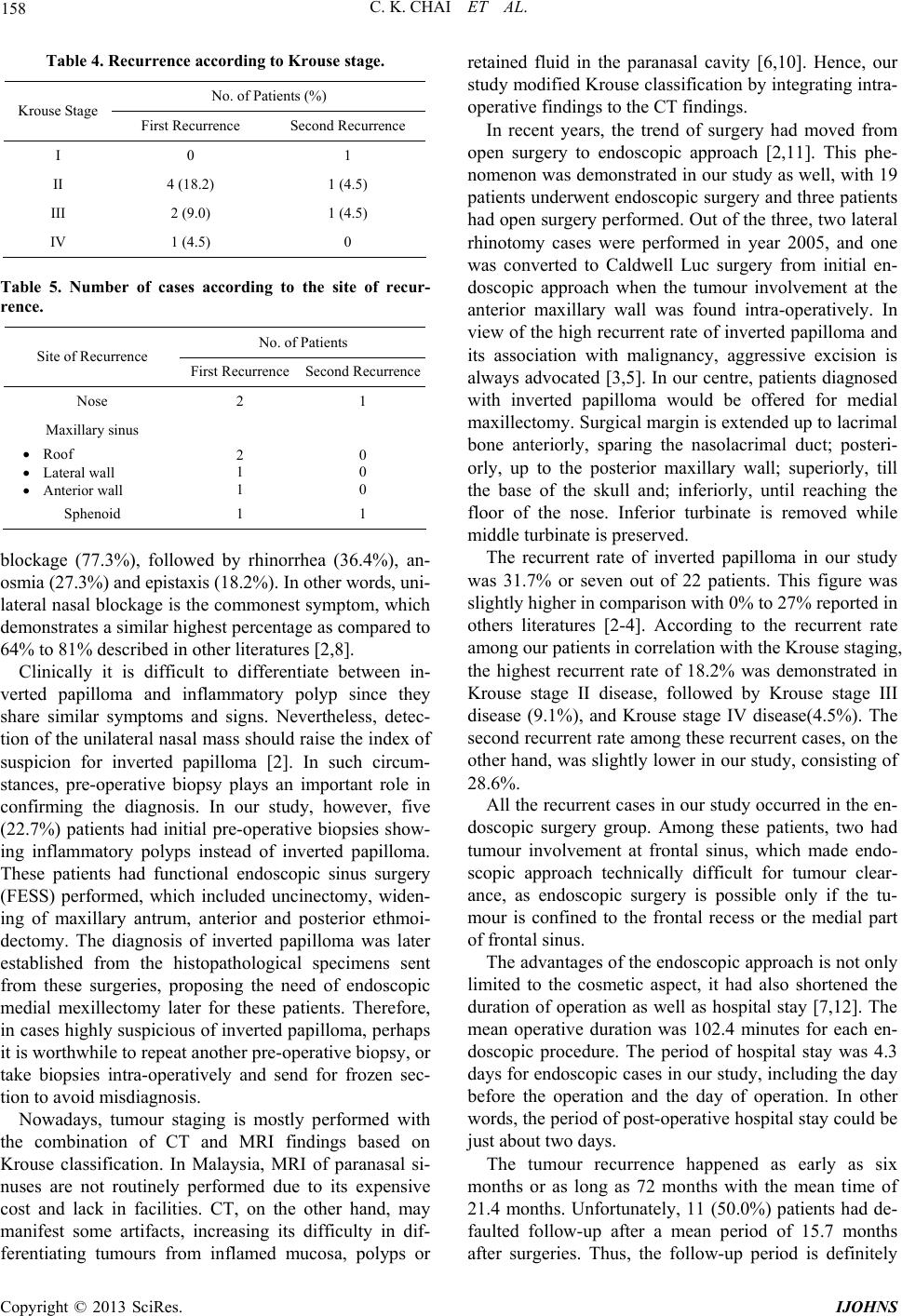
sies is necessary to avoid misdiagnosis. Krouse stage II
disease showed the highest recurrent rate of 18.2%. Life-
long follow-up and emphasis on adherence is mandatory
for early detection of recurrence and malignant transfor-
mation.
REFERENCES
[1] E. Pasquini, V. Sciarretta, G. Farneti, G. C. Modugno and
A. R. Ceroni, “Inverted Papilloma: Report of 89 Cases,”
American Journal of Otolaryngology, Vol. 25, No. 3,
2004, pp. 178-185. doi:10.1016/j.amjoto.2004.01.004
[2] M. A. Thorp, M. F. Oyarzabal-Amiqo, J. H. du Plessis
and S. L. Sellars, “Inverted Papilloma: A Review of 53
Cases,” Laryngoscope, Vol. 111, No. 8, 2001, pp. 1401-
1405. doi:10.1097/00005537-200108000-00016
[3] S. G. Wolfe, R. J. Schlosser, W. E. Bolger, D. C. Lanza
and D. W. Kennedy, “Endoscopic and Endoscope-As-
sisted Resections of Inverted Sinonasal Papillomas,”
Otolaryngology—Head and Neck Surgery, Vol. 131, No.
3, 2004, pp. 174-179. doi:10.1016/j.otohns.2004.05.011
[4] H. Katori and M. Tsukuda, “Staging of Surgical Ap-
proach of Sinonasal Inverted Papilloma,” Auris Nasus
Larynx, Vol. 32, No. 3, 2005, pp. 257-263.
doi:10.1016/j.anl.2005.03.015
[5] R. J. Schlosser, J. C. Mason and C. W. Gross, “Aggres-
sive Endoscopic Resection of Inverted Papilloma: An Up-
date,” Otolaryngology—Head and Neck Surgery, Vol.
125, No. 1, 2001, pp. 49-53.
doi:10.1067/mhn.2001.116789
[6] T. J. Lee, S. F. Huang, L. A. Lee and C. C. Huang, “En-
doscopic Surgery for Recurrent Inverted Papilloma,” La-
ryngoscope, Vol. 114, No. 1, 2004, pp. 106-112.
doi:10.1097/00005537-200401000-00019
[7] J. M. Busquets and P. H. Hwang, “Endoscopic Resection
of Sinonasal Inveted Papilloma: A Meta-Analysis,” Oto-
laryngology—Head and Neck Surgery, Vol. 134, No. 3,
2006, pp. 476-482. doi:10.1016/j.otohns.2005.11.038
[8] W. Lawson and Z. M. Patel, “The Evolution of Manage-
ment for Inverted Papilloma: An Analysis of 200 Cases,”
Otolaryngology—Head and Neck Surgery, Vol. 140, No.
3, 2009, pp. 330-335. doi:10.1016/j.otohns.2008.11.010
[9] W. M. Mendenhall, R. W. Hinerman, R. S. Malyapa, J. W.
Werning, R. J. Amdur, D. B. Villaret and N. P. Men-
denhall, “Inverted Papilloma of Nasal Cavity and Para-
nasal Sinuses,” American Journal of Clinical Oncology,
Vol. 30, No. 5, 2007, pp. 560-563.
doi:10.1097/COC.0b013e318064c711
[10] G. Eggers, J. Muhling and S. Hassfeld, “Inverted Papil-
loma of Paranasal Sinuses,” Journal of Cranio-Maxillo-
facial Surgery, Vol. 35, No. 1, 2007, pp. 21-29.
doi:10.1016/j.jcms.2006.10.003
[11] F. Carta, B. Verillaud and P. Herman, “Role of Endo-
scopic Approach in the Management of Inverted Papil-
loma,” Current Opinion in Otolaryngology & Head and
Neck Surgery, Vol. 19, No. 1, 2011, pp. 21-24.
doi:10.1097/MOO.0b013e3283425213
[12] P. Peng and G. Har-El, “Management of Inverted Papil-
lomas of the Nose and Paranasal Sinuses,” American
Journal of Otolaryngology, Vol. 27, No. 4, 2006, pp. 233-
237. doi:10.1016/j.amjoto.2005.11.005
[13] C. von Buchwald and P. J. Bradley, “Risk of Malignancy
in Inverted Papilloma of the Nose and Paranasal Sin u s es,”
Current Opinion in Otolaryngology & Head and Neck
Surgery, Vol. 15, No. 2, 2007, pp. 95-98.
doi:10.1097/MOO.0b013e3280803d9b