F. Akin et al. / Case Reports in Clinical Medicine 2 (201 3) 338-340 339
moglobulin, 8 g/dL; platelets, 357 × 103/mL; sedimenta-
tion rate, 98 mm/s; CRP, 115 mg/L, serum immunog-
lobulin (Ig)G, IgA and IgM levels, 145 (normal range:
340 - 1200), 26 (30 - 230), and 29 (40 - 200) mg/dL,
respectively. Markedly reduced levels of B cells (CD 19+
cells) in the peripheral circulation (0.06%) were observed
by flow cytometric analysis. Biochemical and urine ana l y-
sis were within normal levels. Antibodies against viral
pathogens including cytomegalovirus, herpes simplex
virus, rubella, toxoplasma, parvovirus B19 and hepatitis
A, B, C viruses were negative. The results of the cu ltures
of blood, sputum, throat and urine were also negative.
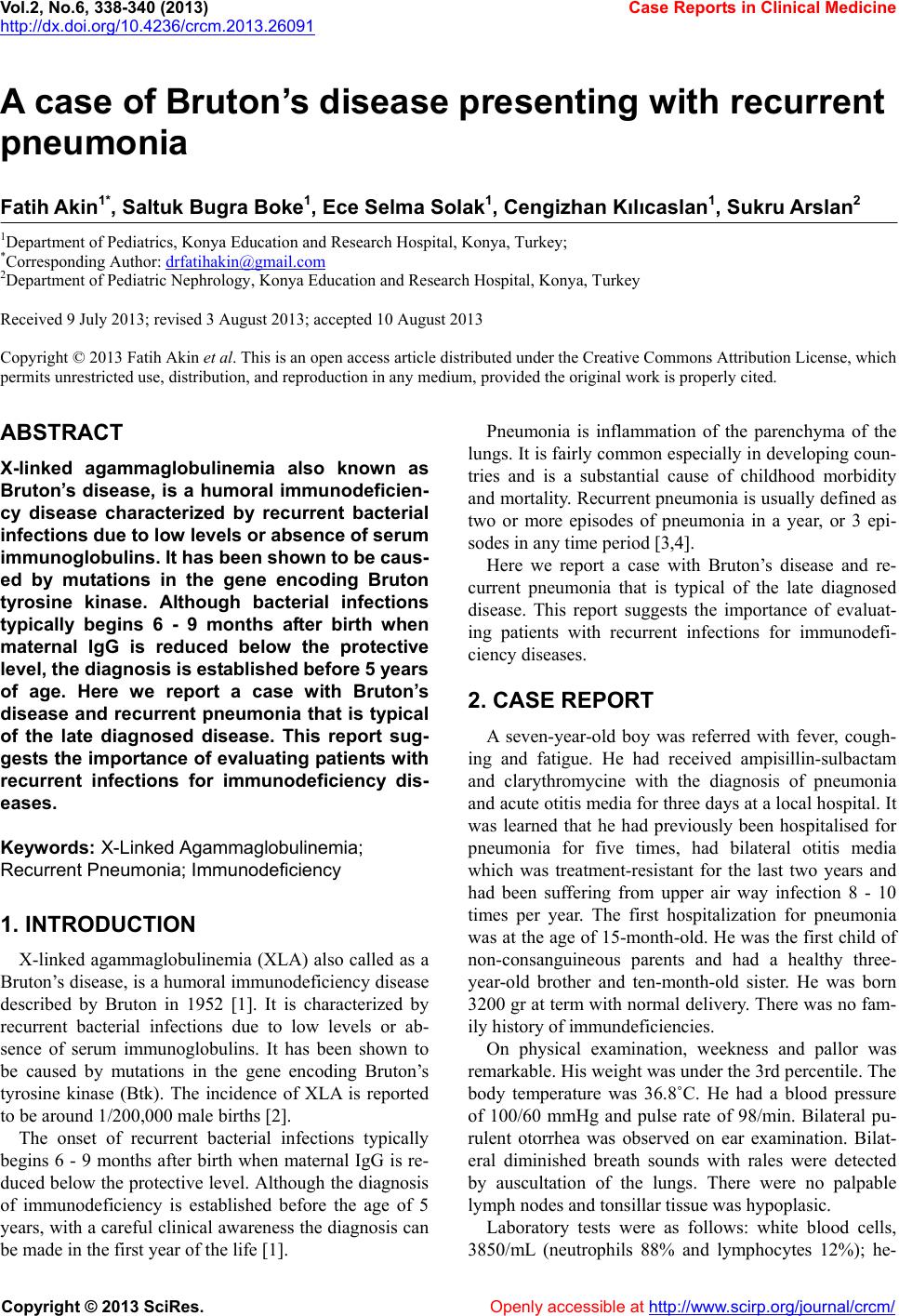
His chest radiography and computed tomography find-
ings revealed bilateral infiltrations, consolidations and a
small amount of left pleural effusion (Figure 1). Sweat
testing and mutation analysis were negative for cystic
fibrosis. Echocardiographic examination for congenital
heart diseases was normal.
After admission to the hospital cefoperazone/sulbac-
tame and teicoplanin were started in travenously. The his-
tory of recurrent pneumonias requiring hospitalization
and recurrent otitis media, h ypogammaglobu lin emia with
the deficiency of CD19 B cells, absence of palpable lymph
nodes and hypoplasic tonsils suggested that our patient
had XLA. On the third day of the hospitalization intra-
venous immunoglobulin (IVIG) 2 gr/kg was given in two
days. On the fourteenth day of admission the patient was
totally recovered and discharged with a treatment sched-
ule of monthly gammaglobulin injections in dosages of
0.4 gr/kg.
3. DISCUSSION
Almost 60% of patients with XLA are diagnosed when
they develop a severe infection. The most common in-
fections seen in XLA patients include recurrent pneu-
monia, empyema, sinusitis, recurrent otitis, sepsis, re-
current meningitis or septic arthritis [1,5,6]. Although
bacterial infections typically begins 6 - 9 months after
birth when maternal IgG is reduced below the protective
level, the diagnosis of XLA is established before 5 years
of age [1]. Present case is a late diagnosed one at the ag e
of seven years old.
Recurrent pneumonia is defined as two or more epi-
Figure 1. Chest radiography and computed tomography show-
ing bilateral infiltrations and consolidations.
sodes of pneumonia in a year, or 3 or more ever [3,4].
Patients with re current pneumonia sho uld be evaluated for
underlying diseases including asthma, congenital heart
disease, gastroesophageal reflux, foreign body aspiration,
structural anomalies, cystic fibrosis and immunodefi-
ciency. Owayed et al. and Lodha et al. reported that 10%
and 15.7% of the patients with recurrent pneumonia had
an underlying disease of immunodeficiency, respectively
[3,4]. A study conducted in Turkey demonstrated that
10% of 71 cases with recurrent pneumonia had immu-
nodeficiency [7]. Chun et al. reported that 68.4% and
31.4% of 19 patients with XLA had pneumonia and acute
otitis media leading to hospitalization [5]. Our case also
had a history of recurrent pneumonia and treatment-re-
sistant otitis media suggesting the necessity of evaluating
patients with recurrent infections for immunodeficiency
diseases.
XLA is a rare genetic disorder in which the develop-
ment of B cells is arrested during differentiation. The
gene responsible for this order was identified in 1993 as
Btk [8]. Althoug h ear ly diagnosis h as be en made possible
by genetic analysis o f th e Btk, id en tifyin g mutatio n is no t
absolutely necessary for the diagnosis [5]. Wang et al.
reported that Btk gene mutation was not identified from
4 of the 16 patients with XLA [8]. The history of recur-
rent pneumonias requiring hospitalization and recurrent
otitis media, hypogammaglobulinemia with the defi-
ciency of CD19 B cells, absence of palpable lymph no des
and hypoplasic tonsils suggested the diagnosis of XLA in
our patient.
In conclusion, pneumonia is one of the most common
reasons for referral to pediatric physicians. Our case em-
phasises that patients with recurrent pneumonia should be
evaluated carefully for immunodeficiency diseases, be-
cause delay in diagnosis and treatment can result in se-
vere illness or death.
REFERENCES
[1] Lee, K.H., Shyur, S.D., Chu, S.H., Huang, L.H., Kao,
Y.H., Lei ,W.T., et al. (2011) Clinical manifestations and
BTK gene defect in 4 unrelated Taiwanese families with
Bruton’s disease. Asian Pacific Journal of Allergy and
Immunology, 29, 260-265.
[2] Váncsa, A., Tóth, B. and Szekanecz, Z. (2011) BTK gene
mutation in two non-identical twins with X-linked agam-
maglobulinemia associated with polyarticular juvenile
idiopathic arthritis. Israel Medical Association Journal,
13, 579-580.
[3] Lodha, R., Puranik, M., Natchu, U.C., and Kabra, S.K.
(2002) Recurrent pneumonia in children: Clinical profile
and underlying causes. Acta Paediatrica, 91, 1170-1173.
d oi:1 0 .1111/ j.16 5 1-2227.2002.tb00123.x
[4] Owayed, A.F., Camphell, D.M., and Wang, E.E.L. (2000)
Underlying causes of recurrent pneumonia in children.
Archives of Pediatrics & Adolescent Medicine, 154 , 190-
Copyright © 2013 SciRes. Openly accessible at http://www.sc irp.or g/journal/crcm/