Y. Y. LIANG, K. C. CARRIERE 5
analyzing medical and health data with correlated binary
responses. To illustrate, we made use of alcohol abuse
data from a family study conducted in Edmonton, Can-
ada.
The non-linear mixed effects model assumes that the
error distribution is normal, while allowing for the het-
erogeneity of the data in the form of mixed effects of
some covariates. In this situation, multilevel models can
be viewed as a special case of non-linear mixed effects
models, but they are especially useful when the data have
more than two levels of hierarchies. Unlike these two
approaches, which assume a correlated binomial distri-
bution of the data, the GEE method does not require the
data to follow a particular parametric distribution. How-
ever, if the number of clusters is very large, all three me-
thods are expected to perform similarly.
Using the alcohol abuse data, we found that the non-
linear mixed model resulted in the best overall model
prediction with the additional advantage of requiring
only a moderate amount of computing time. However,
only a limited number of researches have been done to
check the model assumptions [9-11]. Further research is
needed to improve this aspect of the non-linear mixed
model.
The multilevel method allows for a model with several
levels, but for two-level hierarchical data such as was
used in this study, it is essentially the same as the usual
non-linear mixed effects model. A disadvantage of this
approach is that the algorithm may not converge, espe-
cially when the cluster size is small with few clusters.
Furthermore, the computation time to convergence is
relatively long.
In the GEE approach, we choose the exchangeable
structure of the working correlation matrix, assuming all
relatives of the proband have the same correlation. We
note that Liang and Zeger (1986) originally considered
the correlation among clustered observations as a nui-
sance, while the regression parameters are the primary
interest [2]. With the GEE approach, regression parame-
ters can be estimated consistently but not necessarily
with complete efficiency, whether the working correla-
tion structure is correct or not. This consistency is based
on the assumption that the regression parameters and the
association parameters are orthogonal to one another,
even when they are not [12]. However, the GEE method
may still be preferable in some cases, when a population
averaged level analysis is suitable for the research ques-
tions and objectives. Further, the computational algo-
rithm is relatively fast and it makes weaker assumptions
about the structure of the variance-covariance matrix of
the response vector.
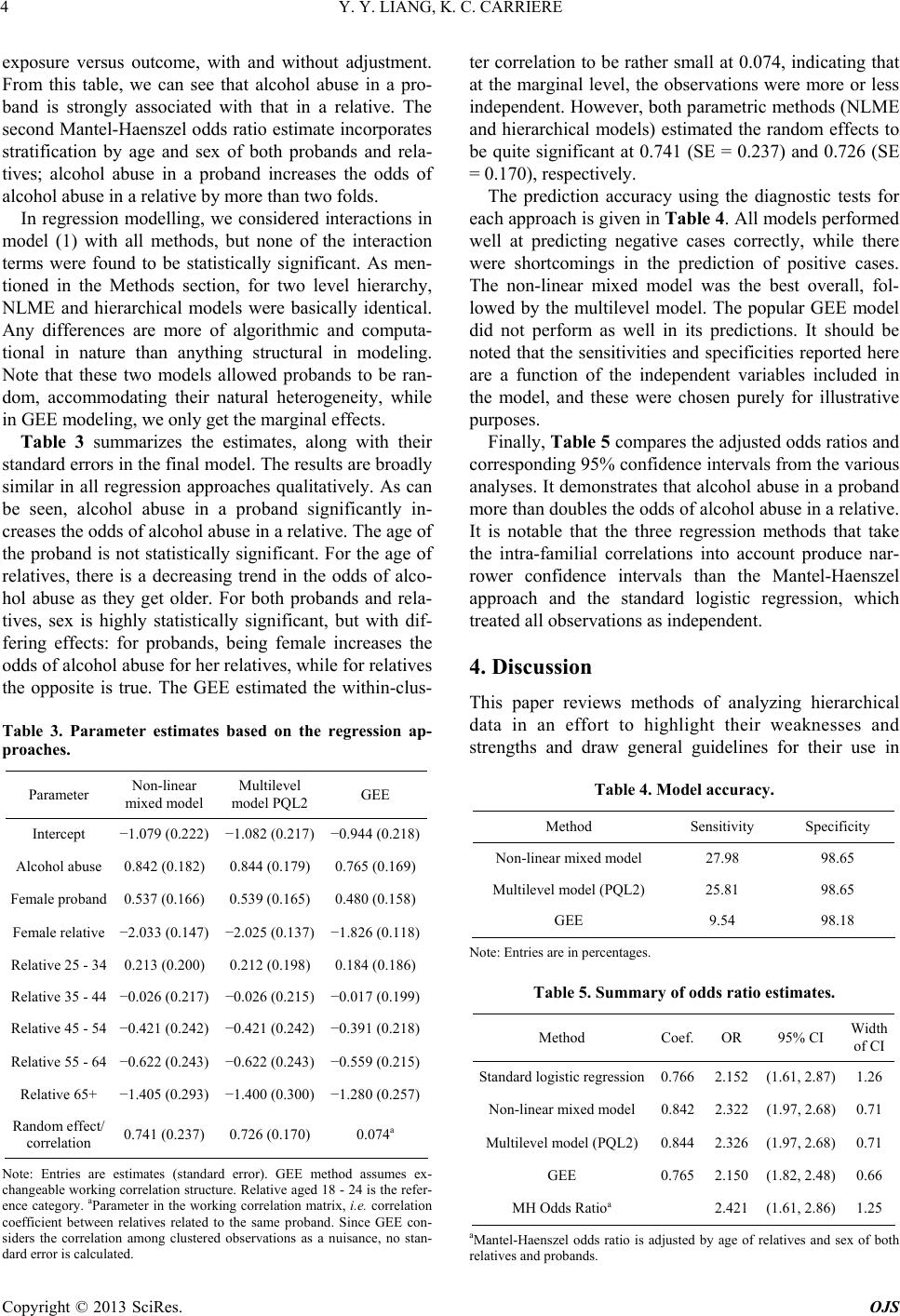
Regarding the model’s prediction accuracy, in general,
the model’s specificity is quite high, but rather low in
sensitivity. In other words, the model has much more
difficulty predicting cases that have an alcohol abuse
problem, which is a common situation when there are no
strong risk factors for modelling. In the absence of ran-
dom effects, all models have an essentially equal ability
to predict the outcome. However, when there are signifi-
cant random effects, the prediction level improves by
properly accounting for the random effects in the model.
5. Conclusion
Overall, the non-linear mixed effects approach to analy-
sis of these data seems quite competitive with the multi-
level method in terms of convergence properties. The
random family effects were significant, reflecting het-
erogeneity among families, and both the non-linear
mixed effects model and the multilevel model captured
them effectively. The popular marginal modeling via the
GEE method may still be preferable because of its com-
putational ease and relaxed distribution assumptions.
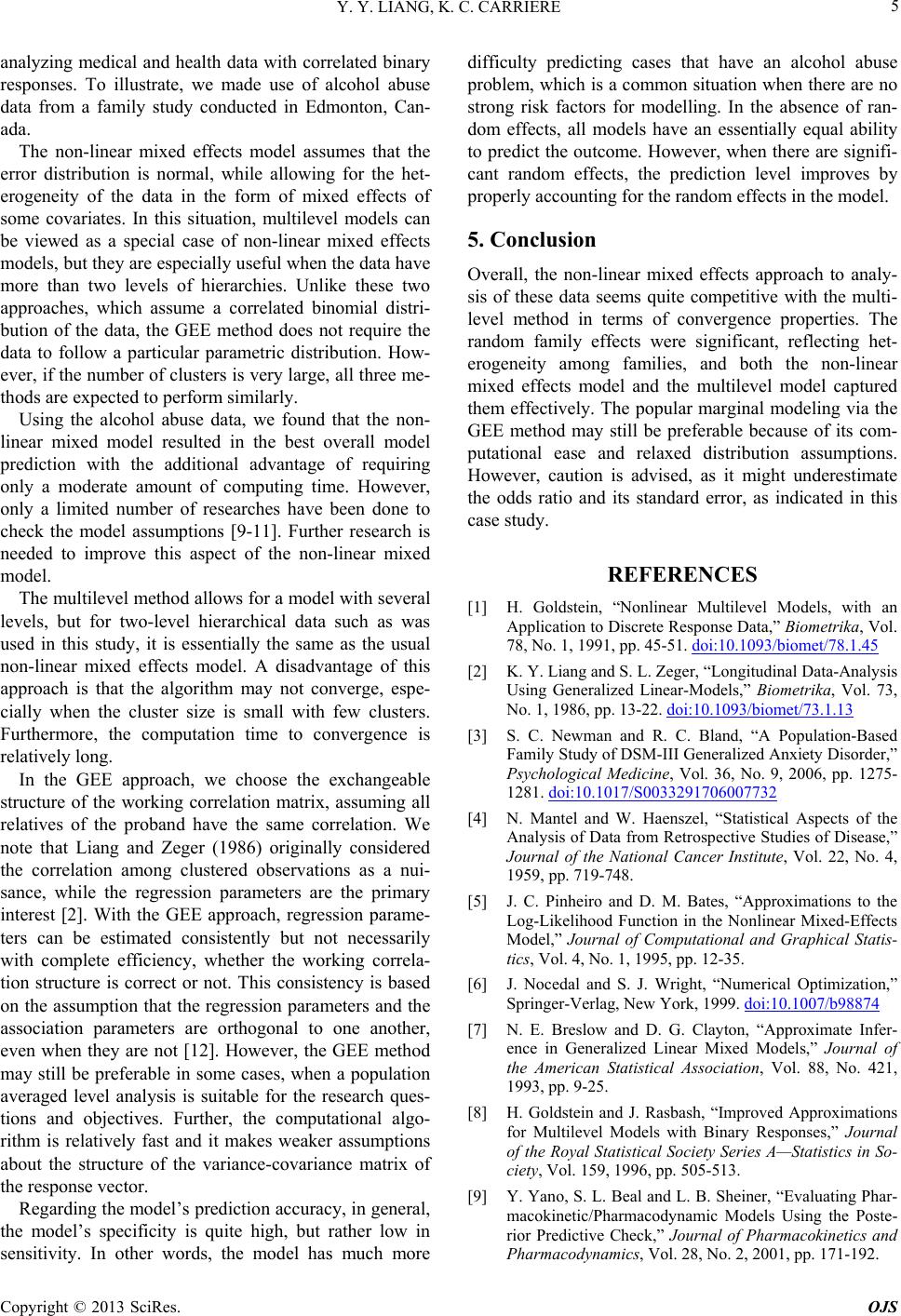
However, caution is advised, as it might underestimate
the odds ratio and its standard error, as indicated in this
case study.
REFERENCES
[1] H. Goldstein, “Nonlinear Multilevel Models, with an
Application to Discrete Response Data,” Biometrika, Vol.
78, No. 1, 1991, pp. 45-51. doi:10.1093/biomet/78.1.45
[2] K. Y. Liang and S. L. Zeger, “Longitudinal Data-Analysis
Using Generalized Linear-Models,” Biometrika, Vol. 73,
No. 1, 1986, pp. 13-22. doi:10.1093/biomet/73.1.13
[3] S. C. Newman and R. C. Bland, “A Population-Based
Family Study of DSM-III Generalized Anxiety Disorder,”
Psychological Medicine, Vol. 36, No. 9, 2006, pp. 1275-
1281. doi:10.1017/S0033291706007732
[4] N. Mantel and W. Haenszel, “Statistical Aspects of the
Analysis of Data from Retrospective Studies of Disease,”
Journal of the National Cancer Institute, Vol. 22, No. 4,
1959, pp. 719-748.
[5] J. C. Pinheiro and D. M. Bates, “Approximations to the
Log-Likelihood Function in the Nonlinear Mixed-Effects
Model,” Journal of Computational and Graphical Statis-
tics, Vol. 4, No. 1, 1995, pp. 12-35.
[6] J. Nocedal and S. J. Wright, “Numerical Optimization,”
Springer-Verlag, New York, 1999. doi:10.1007/b98874
[7] N. E. Breslow and D. G. Clayton, “Approximate Infer-
ence in Generalized Linear Mixed Models,” Journal of
the American Statistical Association, Vol. 88, No. 421,
1993, pp. 9-25.
[8] H. Goldstein and J. Rasbash, “Improved Approximations
for Multilevel Models with Binary Responses,” Journal
of the Royal Statistical Society Series A—Statistics in So-
ciety, Vol. 159, 1996, pp. 505-513.
[9] Y. Yano, S. L. Beal and L. B. Sheiner, “Evaluating Phar-
macokinetic/Pharmacodynamic Models Using the Poste-
rior Predictive Check,” Journal of Pharmacokinetics and
Pharmacodynamics, Vol. 28, No. 2, 2001, pp. 171-192.
Copyright © 2013 SciRes. OJS