World Journal of Cardiovascular Diseases, 2013, 3, 377-379 WJCD
http://dx.doi.org/10.4236/wjcd.2013.35058 Published Online August 2013 (http://www.scirp.org/journal/wjcd/)
Unusual treatment of postoperative bleeding
after cardiac surgery
José Rubio-Alvarez1*, Juan Sierra-Quiroga1, Belén Adrio-Nazar1, Laura Reija López1,
Ángela Granda Bauza1, Carola Rubio Taboada2, Jose Manuel Martinez-Cereijo1
1Department of Cardiac Surgery, Universitary Hospital Santiago de Compostela, Santiago, Spain
2Department of Vascular Surgery, Universitary Hospital of Elche, Alicante, Spain
Email: *framan1@hotmail.com
Received 15 June 2013; revised 20 July 2013; accepted 1 August 2013
Copyright © 2013 José Rubio-Alvarez et al. This is an open access article distributed under the Creative Commons Attribution Li-
cense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
A young patient was presented to the emergency de-
partment with chest pain and palpitations. A tran-
sthoracic echocardiogram showed a right atrial mass.
Coronary angiography showed a right coronary ar-
tery with collateral circulation to a large mass. The
tumor could only be partially resected and the patient
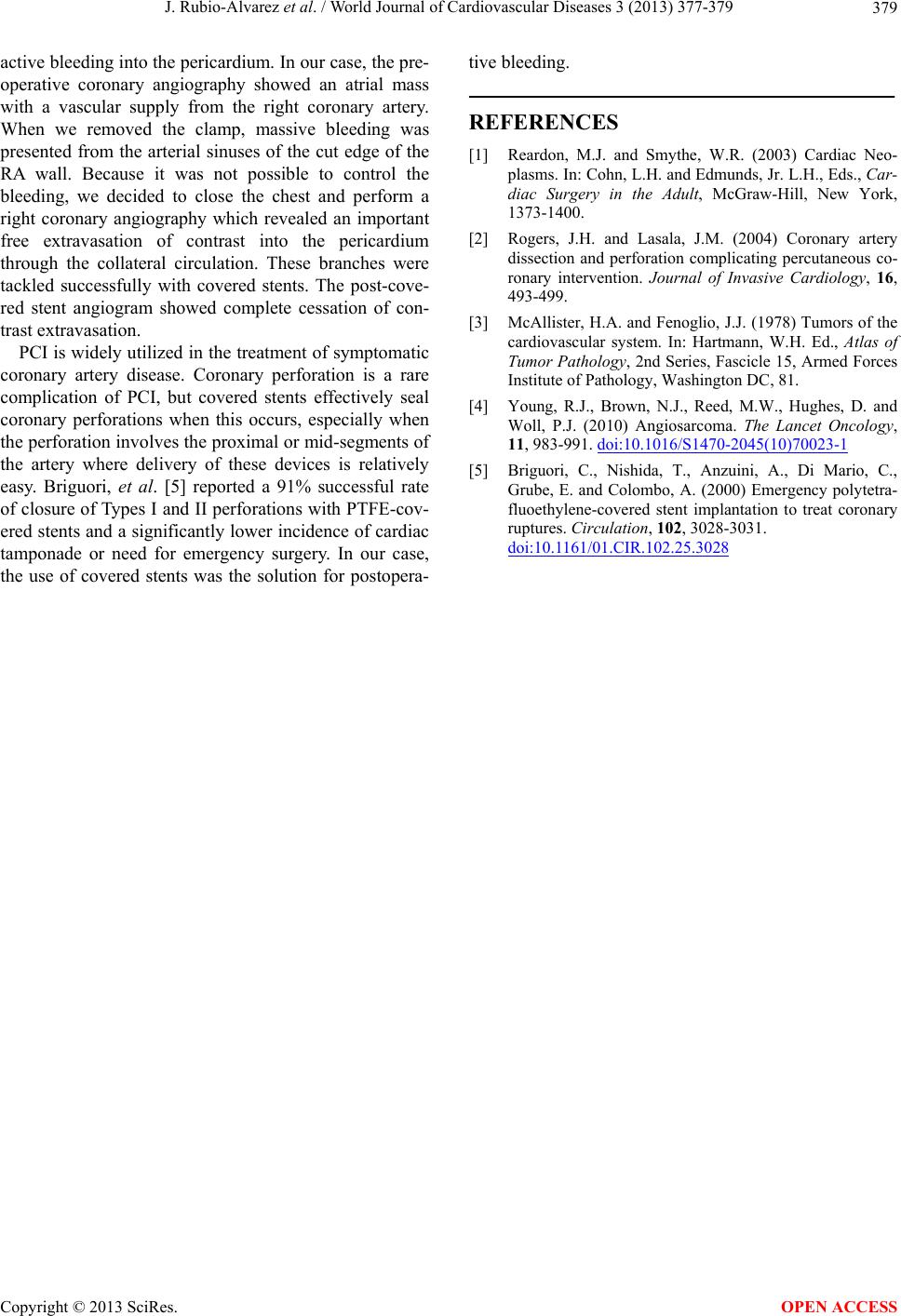
experienced persistent postoperative bleeding. We
performed a new right coronary artery angiography
which showed an important free extravasation of
contrast into the pericardium through the collateral
circulation. Using covered stents, the bleeding was
controlled. The pathological examination performed
later revealed a primary cardiac angiosarcoma. After
asympto m-free survival of 14 month s the patien t pre-
sented bone metastases.
Keywords: Angiosarcoma; Coronary Stenting;
Postoperative Bleeding
1. INTRODUCTION
Primary cardiac malignant tumors are very uncommon
and about 75% are sarcomas [1]. Although rare, angio-
sarcomas are the most common primary malignant neo-
plasms of the heart and are very aggressive and locally
invasive. These tumors are highly vascularized and are
often are actively bleeding into the pericardium.
Since the introduction of percutaneous coronary inter-
vention (PCI) in 197 7, it is increasingly used not only in
simple coronary lesions, but also in complex coronary
anatomies. Coronary perforation is a rare but serious
complication of PCI with the occurrence of important
bleeding into the pericardium. However, this complica-
tion can be tackled successfully with covered stents [2].
We describe the case of a 50-year-old man with non-
metastatic primary right atrial (RA) angiosarcoma, who
underwent surgical excision of the tumor and recon-
struction of the RA with a bovine pericardial patch. The
tumour could only be partially resected and the patient
experienced persistent postoperative bleeding through
the collateral circulation from the right coronary artery,
which was controlled using covered stents. After a sym-
ptom-free survival of 12 months, the patient presented
bone metastases.
2. CASE REPORT
A 50-year-old previously healthy male visited emergency
service because of palpitations and left chest pain. A
chest X-ray showed enlargement of the RA border an d an
electrocardiogram showed normal sinus rhythm with a
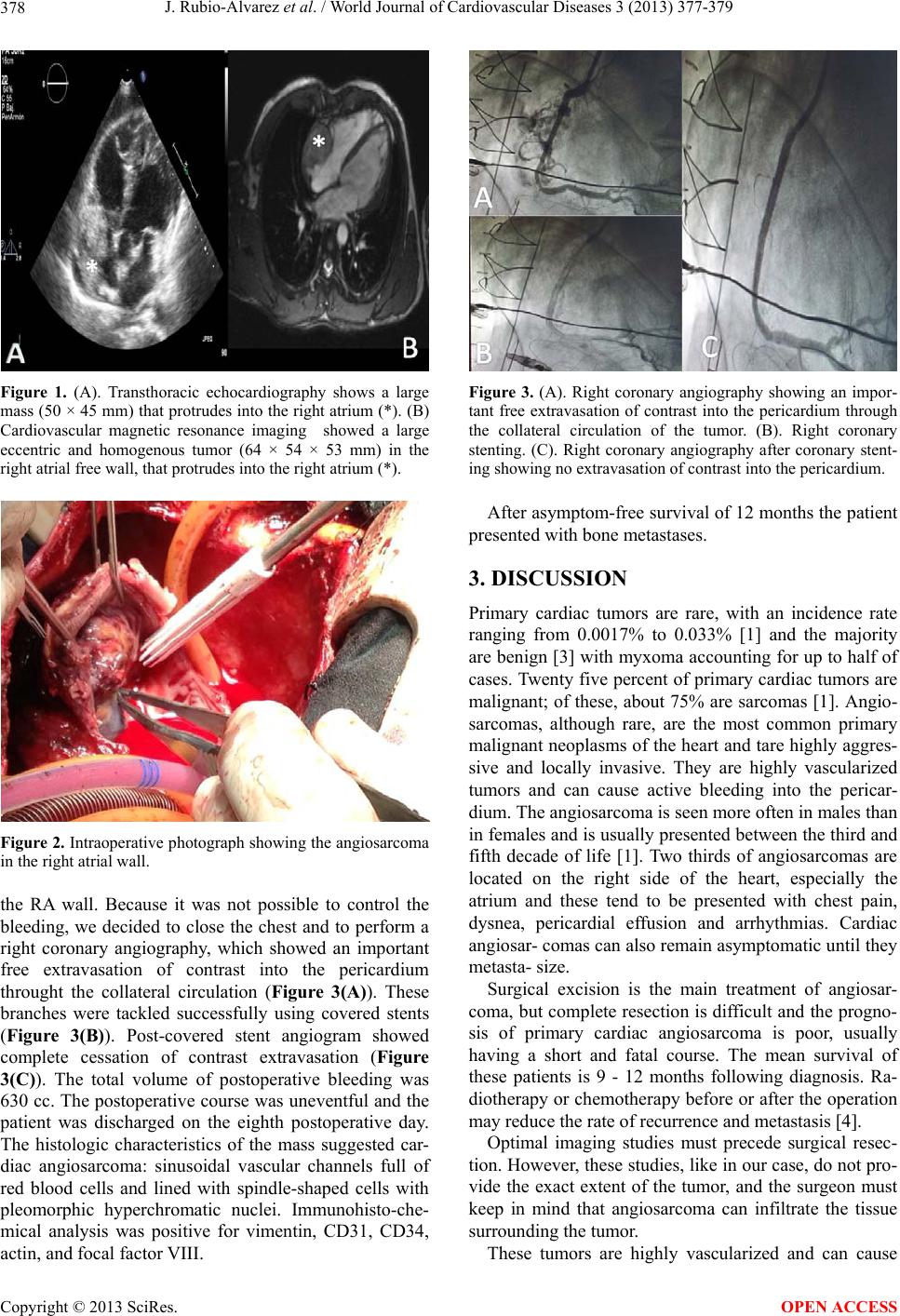
heart rate of 87 beats per minute. A transthoracic echo-
cardiogram was performed and detected a RA mass (50 ×
45 mm) that had infiltrated the free wall of and protruded
into the RA (Figure 1(A)). Left ventricular function was
normal and there were no valvular abnormalities. For
further evaluation of the RA mass magnetic resonance
imaging was performed (Figure 1(B)). This exploration
also showed a large eccentric tumor (64 × 54 × 53 mm)
in the RA free wall, protruding into the right atrium. The
tumor extended into the right atrioventricular groove, but
did not involve the right ventricle, or the annulus of the
tricuspid valve. Coronary angiography showed a right
coronary artery with collateral circulation to a large mass.
Surgery was performed under standard extracorporeal
circulation with selective cannulation of both cava veins
and the ascending aorta. The RA was excised (Figure 2),
but the tumor could only be partially resected because it
extended into the free wall of the right ventricle and tri-
cuspid valve annulus. The RA was reconstructed using
bovine pericardium. After declamping massive bleeding
was present from the arterial sinuses of the cut edge of
*Corresponding a uthor.
OPEN ACCESS