K. Wada et al. / Case Reports in Clinical Medicine 2 (2013) 332-334
334
sible for an increase in cerebral blood flow may play a
pivotal role [2,3]. Blood transfusion may result in a rapid
increase in total blood volume, leading to rapid overload
of cerebral blood flow. Cerebral hyperperfusion, if it is
acutely induced and exceeds the capacity for autoregula-
tion of perfusion pressure in cerebral capillaries, could
result in the huge vasogenic edema responsible for PRES.
In addition, the possibility should not be excluded that
severe anemia per se also might be the predisposing fac-
tor contributing to the induction of PRES, because in-
sufficient oxygen supply due to severe anemia might
exert an unfavorable influence on endothelial cell func-
tions, possibly causing a breakdown of the integrity of
the bloodbrain barrier in capillary circulation.
Another issue is whether a rapid increase in blood
pressure, which is frequently associated with PRES [1-3,
10], simultaneously contributed to inducing PRES in the
present study. In this regard, we think that hypertension
might not have played a prominent role in the mecha-
nism underlying PRES in the present case. During the
course of illness, hypertension was only transiently ob-
served, and an extreme increase in blood pressure (>180
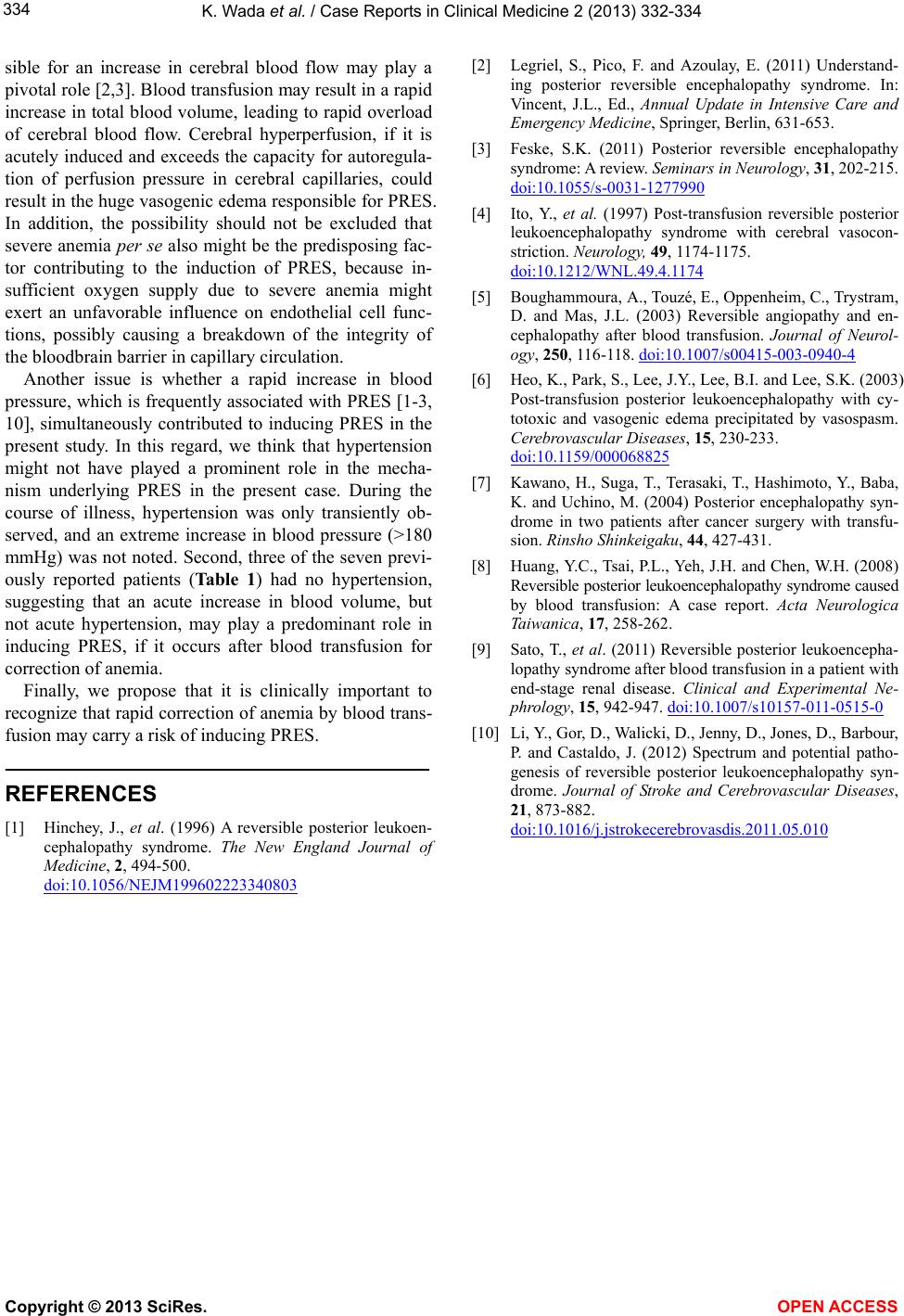
mmHg) was not noted. Second, three of the seven previ-
ously reported patients (Table 1) had no hypertension,
suggesting that an acute increase in blood volume, but
not acute hypertension, may play a predominant role in
inducing PRES, if it occurs after blood transfusion for
correction of anemia.
Finally, we propose that it is clinically important to
recognize that rapid correction of anemia by blood trans-
fusion may carry a risk of inducing PRES.
REFERENCES
[1] Hinchey, J., et al. (1996) A reversible posterior leukoen-
cephalopathy syndrome. The New England Journal of
Medicine, 2, 494-500.
doi:10.1056/NEJM199602223340803
[2] Legriel, S., Pico, F. and Azoulay, E. (2011) Understand-
ing posterior reversible encephalopathy syndrome. In:
Vincent, J.L., Ed., Annual Update in Intensive Care and
Emergency Medicine, Springer, Berlin, 631-653.
[3] Feske, S.K. (2011) Posterior reversible encephalopathy
syndrome: A review. Seminars in Neurology, 31, 202-215.
doi:10.1055/s-0031-1277990
[4] Ito, Y., et al. (1997) Post-transfusion reversible posterior
leukoencephalopathy syndrome with cerebral vasocon-
striction. Neurology, 49, 1174-1175.
doi:10.1212/WNL.49.4.1174
[5] Boughammoura, A., Touzé, E., Oppenheim, C., Trystram,
D. and Mas, J.L. (2003) Reversible angiopathy and en-
cephalopathy after blood transfusion. Journal of Neurol-
ogy, 250, 116-118. doi:10.1007/s00415-003-0940-4
[6] Heo, K., Park, S., Lee, J.Y., Lee, B.I. and Lee, S.K. (2003)
Post-transfusion posterior leukoencephalopathy with cy-
totoxic and vasogenic edema precipitated by vasospasm.
Cerebrovascular Diseases, 15, 230-233.
doi:10.1159/000068825
[7] Kawano, H., Suga, T., Terasaki, T., Hashimoto, Y., Baba,
K. and Uchino, M. (2004) Posterior encephalopathy syn-
drome in two patients after cancer surgery with transfu-
sion. Rinsho Shinkeigaku, 44, 427-431.
[8] Huang, Y.C., Tsai, P.L., Yeh, J.H. and Chen, W.H. (2008)
Reversible posterior leukoencephalopathy syndrome caused
by blood transfusion: A case report. Acta Neurologica
Taiwanica, 17, 258-262.
[9] Sato, T., et al. (2011) Reversible posterior leukoencepha-
lopathy syndrome after blood transfusion in a patient with
end-stage renal disease. Clinical and Experimental Ne-
phrology, 15, 942-947. doi:10.1007/s10157-011-0515-0
[10] Li, Y., Gor, D., Walicki, D., Jenny, D., Jones, D., Barbour,
P. and Castaldo, J. (2012) Spectrum and potential patho-
genesis of reversible posterior leukoencephalopathy syn-
drome. Journal of Stroke and Cerebrovascular Diseases,
21, 873-882.
doi:10.1016/j.jstrokecerebrovasdis.2011.05.010
Copyright © 2013 SciRes. OPEN ACCESS