A Case Report of Fever of Unknown Origin (FUO)
Copyright © 2013 SciRes. JCT
1147
ALCL was first described by Stein et al. in 1985.This
new entity was characterized by large anaplastic cells
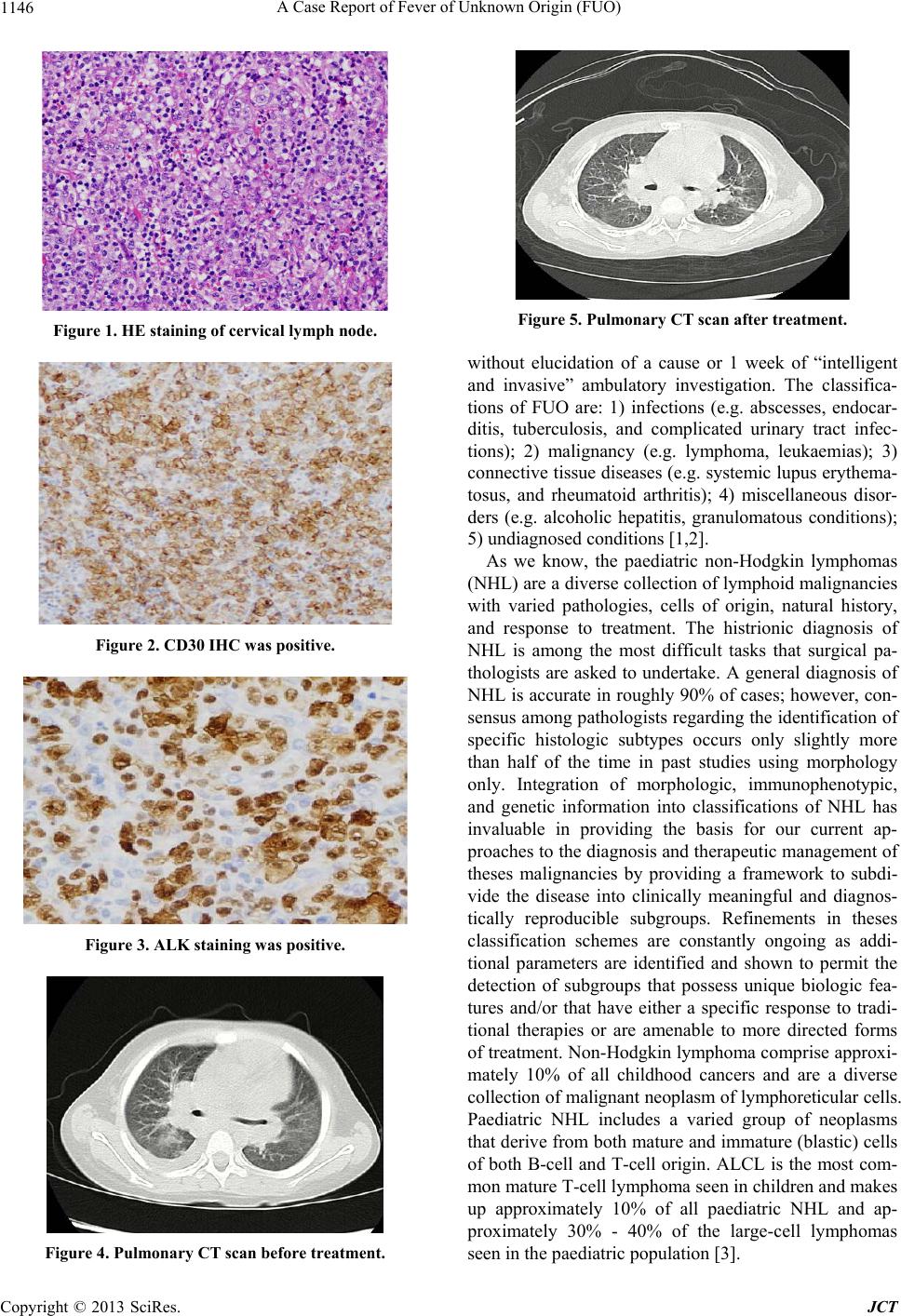
with strong reactivity to the monoclonal antibody, Ki-1
(CD30). Morphologically, primary systemic ALCL can
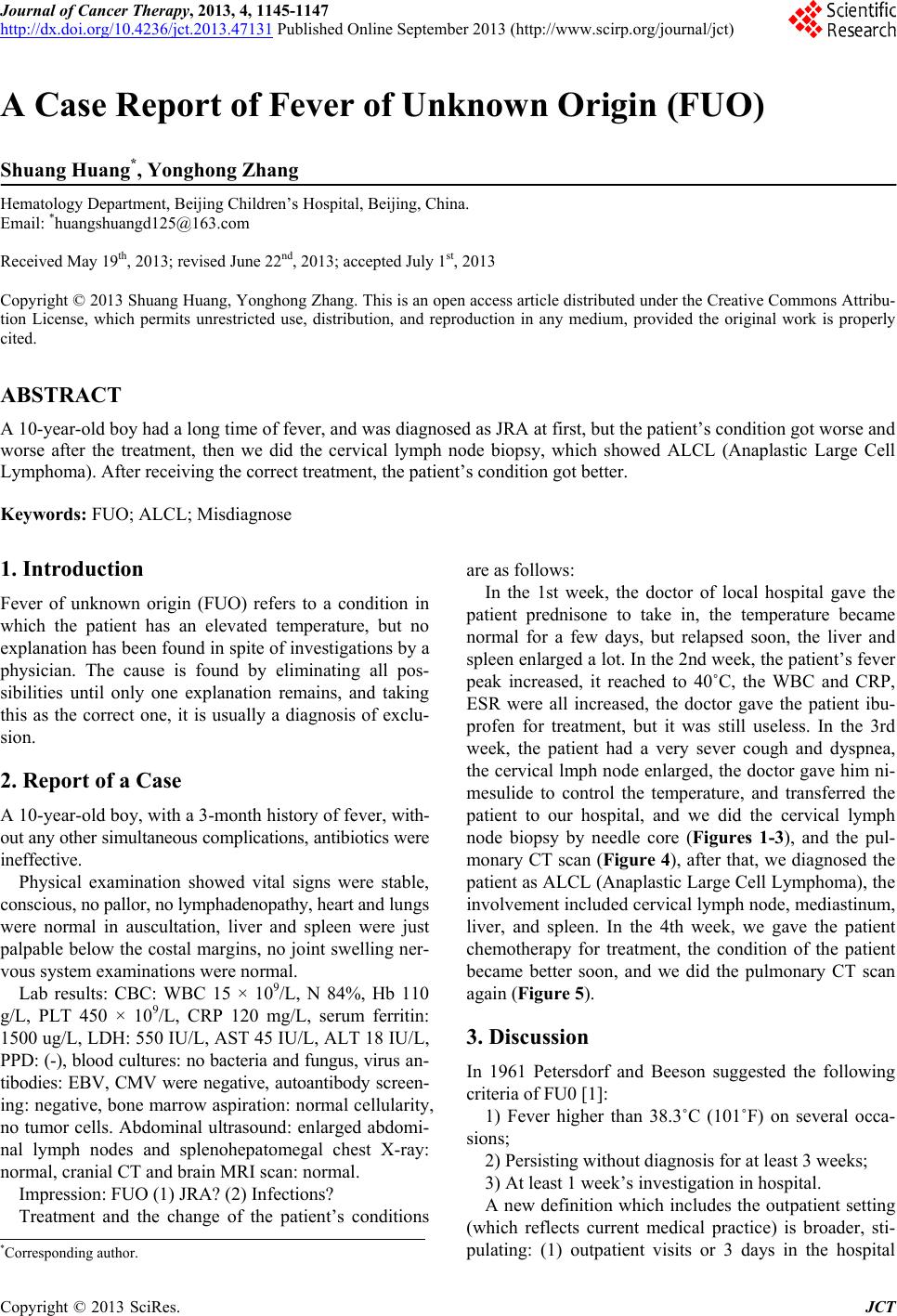
be quite variable. Classic ALCL has a predominance of
tumor cells that are large, pleomorphic, and often multi-
nucleated. Often these cells contain eccentric horseshoe-
shaped nuclei with abundant clear-to-basophilic cyto-
plasm with an area of eosinophilia near the nucleus. A
small-cell variant of ALCL has also been described where
the cells are smaller in size, more monomorphic, and
show minimal cytologic variation. ALCL has tumor cells
which express the CD30 (ki-1) antigen in virtually all
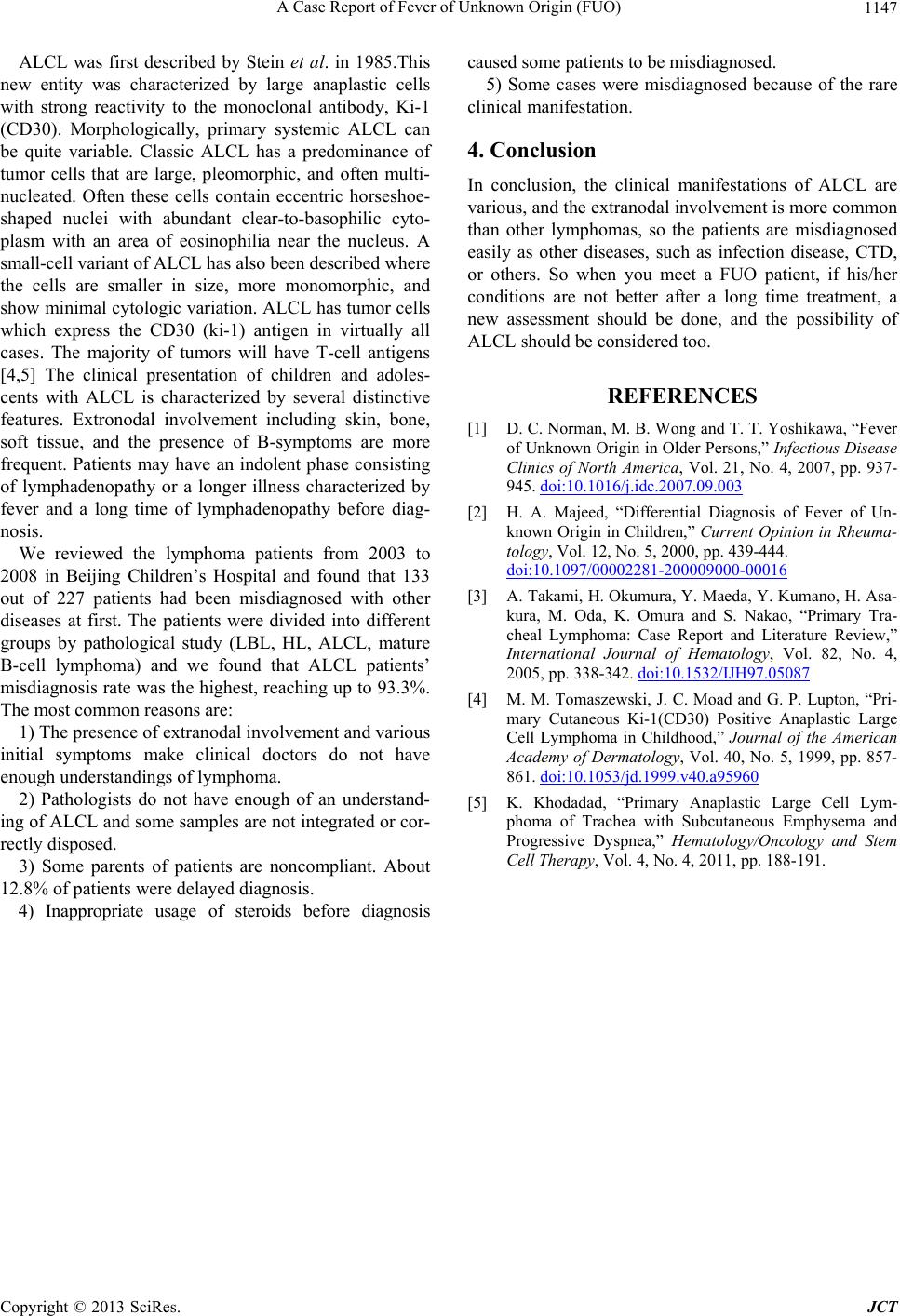
cases. The majority of tumors will have T-cell antigens
[4,5] The clinical presentation of children and adoles-
cents with ALCL is characterized by several distinctive
features. Extronodal involvement including skin, bone,
soft tissue, and the presence of B-symptoms are more
frequent. Patients may have an indolent phase consisting
of lymphadenopathy or a longer illness characterized by
fever and a long time of lymphadenopathy before diag-
nosis.
We reviewed the lymphoma patients from 2003 to
2008 in Beijing Children’s Hospital and found that 133
out of 227 patients had been misdiagnosed with other
diseases at first. The patients were divided into different
groups by pathological study (LBL, HL, ALCL, mature
B-cell lymphoma) and we found that ALCL patients’
misdiagnosis rate was the highest, reaching up to 93.3%.
The most common reasons are:
1) The presence of extranodal involvement and various
initial symptoms make clinical doctors do not have
enough understandings of lymphoma.
2) Pathologists do not have enough of an understand-
ing of ALCL and some sample s are not integrated or cor -
rectly disposed.
3) Some parents of patients are noncompliant. About
12.8% of pa t ients were delayed diagnosis.
4) Inappropriate usage of steroids before diagnosis
caused some patients to be misdiagnosed.
5) Some cases were misdiagnosed because of the rare
clinical manifestation.
4. Conclusion
In conclusion, the clinical manifestations of ALCL are
various, and the extranodal involvement is more common
than other lymphomas, so the patients are misdiagnosed
easily as other diseases, such as infection disease, CTD,
or others. So when you meet a FUO patient, if his/her
conditions are not better after a long time treatment, a
new assessment should be done, and the possibility of
ALCL should be considered too.
REFERENCES
[1] D. C. Norman, M. B. Wong and T. T. Yoshikawa, “Fever
of Unknown Origin in Older Persons,” Infectious Disease
Clinics of North America, Vol. 21, No. 4, 2007, pp. 937-
945. doi:10.1016/j.idc.2007.09.003
[2] H. A. Majeed, “Differential Diagnosis of Fever of Un-
known Origin in Children,” Current Opinion in Rheuma-
tology, Vol. 12, No. 5, 2000, pp. 439-444.
doi:10.1097/00002281-200009000-00016
[3] A. Takami, H. Okumura, Y. Maeda, Y. Kumano, H. Asa-
kura, M. Oda, K. Omura and S. Nakao, “Primary Tra-
cheal Lymphoma: Case Report and Literature Review,”
International Journal of Hematology, Vol. 82, No. 4,
2005, pp. 338-342. doi:10.1532/IJH97.05087
[4] M. M. Tomaszewski, J. C. Moad and G. P. Lupton, “Pri-
mary Cutaneous Ki-1(CD30) Positive Anaplastic Large
Cell Lymphoma in Childhood,” Journal of the American
Academy of Dermatology, Vol. 40, No. 5, 1999, pp. 857-
861. doi:10.1053/jd.1999.v40.a95960
[5] K. Khodadad, “Primary Anaplastic Large Cell Lym-
phoma of Trachea with Subcutaneous Emphysema and
Progressive Dyspnea,” Hematology/Oncology and Stem
Cell Therapy, Vol. 4, No. 4, 2011, pp. 188-191.