Compared Evaluation of Botulinum Toxin A and a Cosmetic Antiperspirant
in the Treatment of Focal Axillary Hyperhidrosis
195
after application. Moreover skin irritation can be a cumu-
lative side effect of long-term treatment.
Another effective treatment modality is the intrader-
mal injection of botulinum toxin A which has been stud-
ied in numerous clinical trials [15,17-20]. It has demon-
strated a sustained relief of symptoms with a good safety
profile in open-label studies of the treatment of axillary
hyperhidrosis. Naumann et al. demonstrated in a double-
blind, placebo-controlled trial a 93.8% response rate after
a single treatment with 50 U total onabotulinumtoxin A
and a safety profile that was comparable to that of pla-
cebo injections [19]. In addition Heckmann et al. showed
an efficacy of onabotulinumtoxin A in a placebo-con-
trolled trial [15].
Therefore we designed an inter-individual comparison
of onabotulinumtoxin A and a cosmetic antiperspirant
containing aluminum chloride in a panel of 22 female
patients suffering from hyperhidrosis as objected by gra-
vimetry.
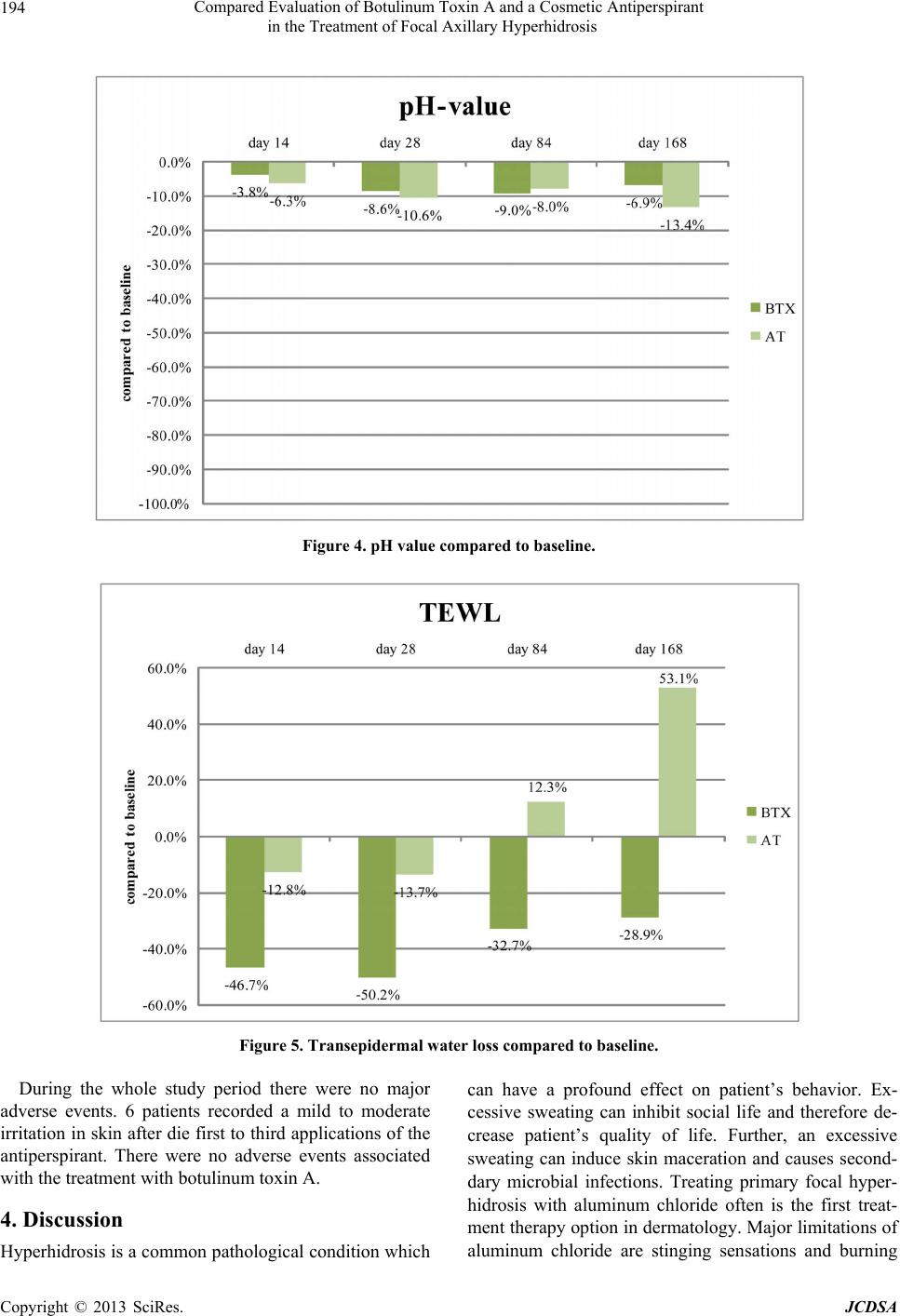
Regarding skin physiology both treatments were well
tolerated. While TEWL decreased during both treatment
modalities (BTX-A: 5.9 to 5.54; AL: 5.97 to 5.17), skin
pH never left the physiological range.
Our study confirms and extends the results of previous
studies regarding the gravimetry, the rate of sweat pro-
duction and the tolerability [15-17,20-24].
Further to a previous study which compared botulinum
toxin A with a topical 20% aluminum chloride for the
treatment of focal axillary hyperhidrosis our data confirm
that both products provide efficacy treatment option al-
though our data are different concerning the tolerability
of the antiperspirant [25]. According to Flanagan et al.
the aluminum chloride treatment was well tolerated and
effective only in the minority of the patients. This might
be due to the lower dose of 12, 5% aluminum chloride.
However, while Flanagan et al. demonstrated a clean
superiority of onabotulinumtoxin A and a high risk for
skin irritation after treatment with aluminum chloride,
our data did not reveal any significant differences in ef-
ficacy and tolerability between both treatments. This
might be due to the special developed of non-alcoholic
galinic formation and the low aluminum chloride con-
centration of the Sweat-Off® lotion.
5. Conclusion
Treatments of axillary focal hyperhidrosis with BTX-A
or an antiperspirant containing aluminum chloride in the
evaluated galenic formulation and low dose concentra-
tion are effective and safe options. Both treatment mo-
dalities significantly reduced the degree of hyperhidrosis.
Patients rated both options as an effective treatment.
However, patients with sensitive skin treatments with on-
abotulinumtoxin A seem to have a better therapeutic in-
dex while topical treatment with aluminum chloride de-
monstrates a better economic impact.
REFERENCES
[1] F. G. Bechara, Current Treatment of Focal Hyperhidro-
sis,” Surgical Approaches Hautarzt, Vol. 60, No. 7, 2009,
pp. 538-545. doi:10.1007/s00105-009-1717-1
[2] F. G. Bechara, T. Gambichler, A. Bader, M. Sand, P.
Altmeyer and K. Hoffmann, “Assessment of Quality of
Life in Patients with Primary Axillary Hyperhidrosis
Before and After Suction-Curettage,” Journal of the
American Academy of Dermatology, Vol. 57, No. 2, 2007,
pp. 207-212. doi:10.1016/j.jaad.2007.01.035
[3] D. R. Strutton, J. W. Kowalski, D. A. Glaser and P. E.
Stang, “US Prevalence of Hyperhidrosis and Impact on
Individuals with Axillary Hyperhidrosis: Results from a
National Survey,” Journal of the American Academy of
Dermatology, Vol. 51, No. 2, 2004, pp. 241-248.
doi:10.1016/j.jaad.2003.12.040
[4] R. Ramos and J. Moya, “Primary Hyperhidrosis and An-
xiety: A Prospective Preoperative Survey of 158 Pati-
ents,” Archivos de Bronconeumología, Vol. 41, No. 2,
2005, pp. 88-92.
[5] M. Amir, A. Arish and Y. Weinstein, “Impairment in
Quality of Life among Patients Seeking Surgery for
Hyperhidrosis: Preliminary Results,” Israel Journal of
Psychiatry & Related Sciences, Vol. 37, No. 1, 2000, pp.
25-31.
[6] W. B. Shelley and H. J. Hurley Jr., “Studies on Topical
Antiperspirant Control of Axillary Hyperhidrosis,” Acta
Dermato-Venereologica, Vol. 55, No. 4, 1975, pp. 241-
260.
[7] H. Bouman, “The Treatment of Hyperhidrosis of Hands
and Feet with Constant Current,” American Journal of
Physical Medicine & Rehabilitation, Vol. 31, No. 3, 1952,
pp. 158-169.
[8] B. Przybilla, U. Schwab, E. Hölzle and J. Ring, “Contact
Sensitization to an Antiperspirant with the Active Ingre-
dient Propantheline Bromide,” Hautarzt, Vol. 34, No. 9,
1983, pp. 459-462.
[9] M. Hund, R. Sinkgraven and B. Rzany, “Randomized,
Placebo-Controlled, Double Blind Clinical Trial for the
Evaluation of the Efficacy and Safety of Oral Methanthe-
liniumbromide (Vagantin) in the Treatment of Focal
Hyperhidrosis,” Journal der Deutschen Dermatologis-
chen Gesellschaft, Vol. 2, No. 5, 2004, pp. 343-349.
doi:10.1046/j.1439-0353.2004.04765.x
[10] K. T. Moran and M. P. Brady, “Surgical Management of
Primary Hyperhidrosis,” British Journal of Surgery, Vol.
78, No. 3, 1991, pp. 279-283. doi:10.1002/bjs.1800780306
[11] E. Hölzle and O. Braun-Falco, “Structural Alteractions of
Axillary Eccrine Glands in Hyperhidrosis Following Long-
Term Treatment with Aluminium Chloride Hexahydrate,”
British Journal of Dermatology, Vol. 110, No. 4, 1984,
pp. 399-403. doi:10.1111/j.1365-2133.1984.tb04653.x
[12] E. Hölzle, “Topical Pharmacological Treatment,” Current
Copyright © 2013 SciRes. JCDSA