C. Damas et al. / Case Reports in Clinical Medicine 2 (2013) 322-325
324
amnesia, the media publicized his story and printed his
picture, also interpol were involved. After two weeks
another man came to the same hospital with same symp-
toms but clinicians referred there were no symptoms of
psychosis elicited and no evidence of cognitive impair-
ment. After three days a teleph one number was found on
his person, this transpired to be his father’s number that
said the patient was waiting for admission to the local
psychiat r ic hospital because of paran oid schizop hrenia.
After two weeks the same patient was admitted to the
orthopaedic ward with multiple fractures having fallen
from scaffolding. He described delusion of persecution
and passivity and a diagnosis of Munchausen Syndrome
was referred [8].
Faida, Smith et al. described a rare case of Lobular
Panniculitis, a 40-year-old female was hospitalized to in-
vestigate numerous painful unilateral ecchymoses found
on her right low er leg. She denied any h istory of trauma.
During hospitalization new ecchymoses were noted and
also a worsening of the patient’s pre existing lesion. Af-
ter more exams and days on charge all the symptoms
resolved spontaneously. A late X-ray of the leg showed
the presence of a sewing needle into her calf. After this,
the patient became aggressive and attempted to jump out
of the hospital window, fortun ately the staff were able to
stop her. The patient refused any further medical assis-
tance or psychiatric follow up so she discharged herself
from hospital, and the psychiatric team referred a severe
Munchausen Syndrome [9].
Goto and Sasajima described a 64-year-old man ad-
mitted to the hospital after head injury. Ct and Mr imag-
ing revealed a mass with edema in the right frontal lobe.
This mass was surgically removed and the authors no-
ticed a small bone defect in the frontal bone above the
brain abscess. The patient presented atypical seizures
several times, and after the discharged of the patient he
was hospitalized again because the wound had reop ened.
After the second surgery he stabbed a nail into his head
where the bone had been removed due to the previous
surgery, and presented intraventricular hemorrhage that
decreased in size with non-surgical treatment. So the
patient was referred to the psychiatry department with a
diagnosis of Munchausen Syndrome [10].
In particular, consider this patient as affected by an at-
tack of acute pancreatitis was clinically reasonable. How-
ever, is commonly known that serum amylase is insuffi-
ciently sensitive in severe pancreatitis, but also needs to
be aware that a normal serum amylase does not exclude
severe forms of acute pancreatitis, which are associated
with a high morbidity and mortality [11-13] this is main-
ly due to the fact that amylase is rapidly cleared from the
kidneys, and this, along with other factors, may lead to a
normal serum amylase level even in the presence of ne-
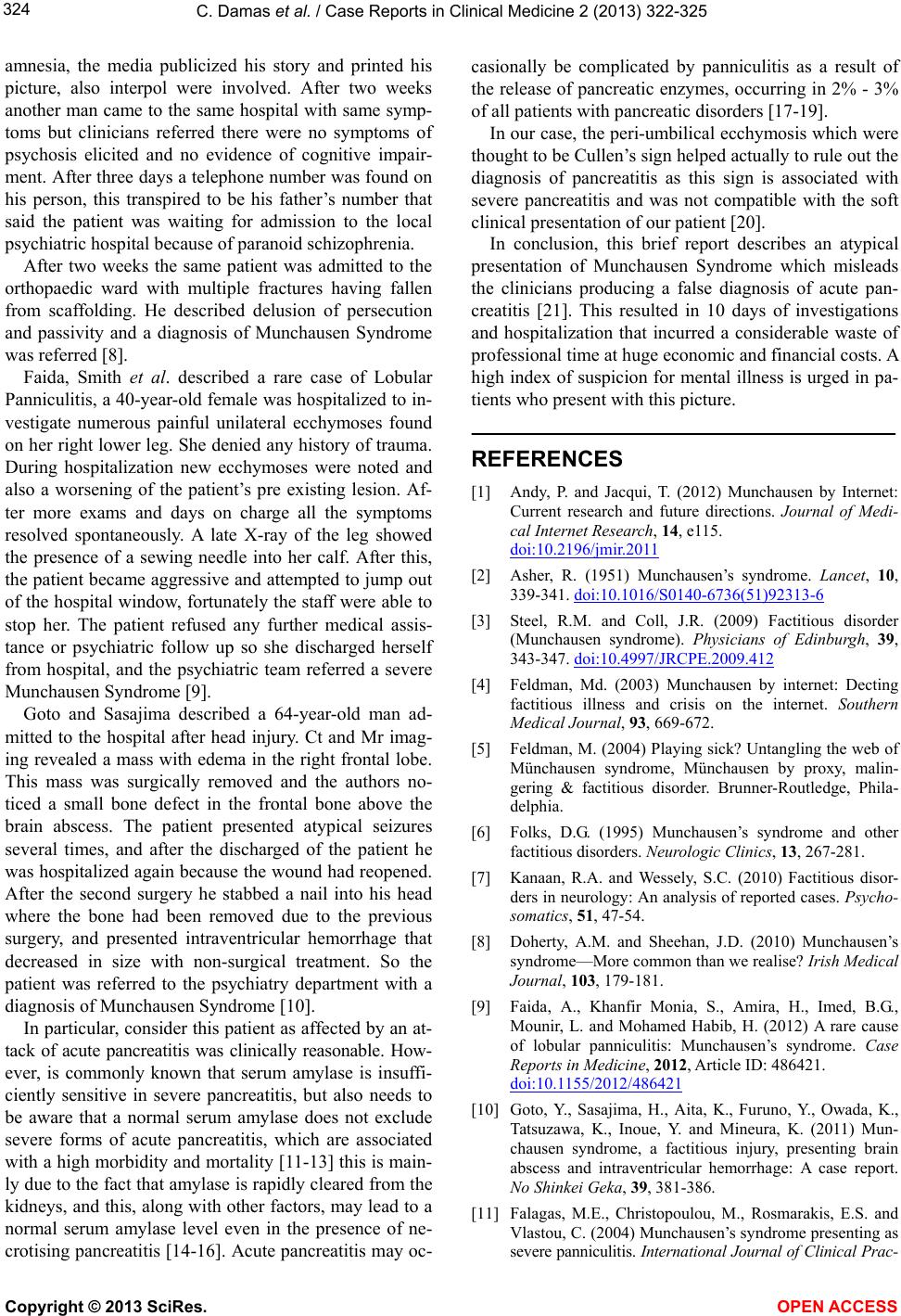
crotising pancreatitis [14-16]. Acute pancreatitis may o c-
casionally be complicated by panniculitis as a result of
the release of pancreatic enzymes, occurring in 2% - 3%
of all patients with pancreatic disorders [17-19].
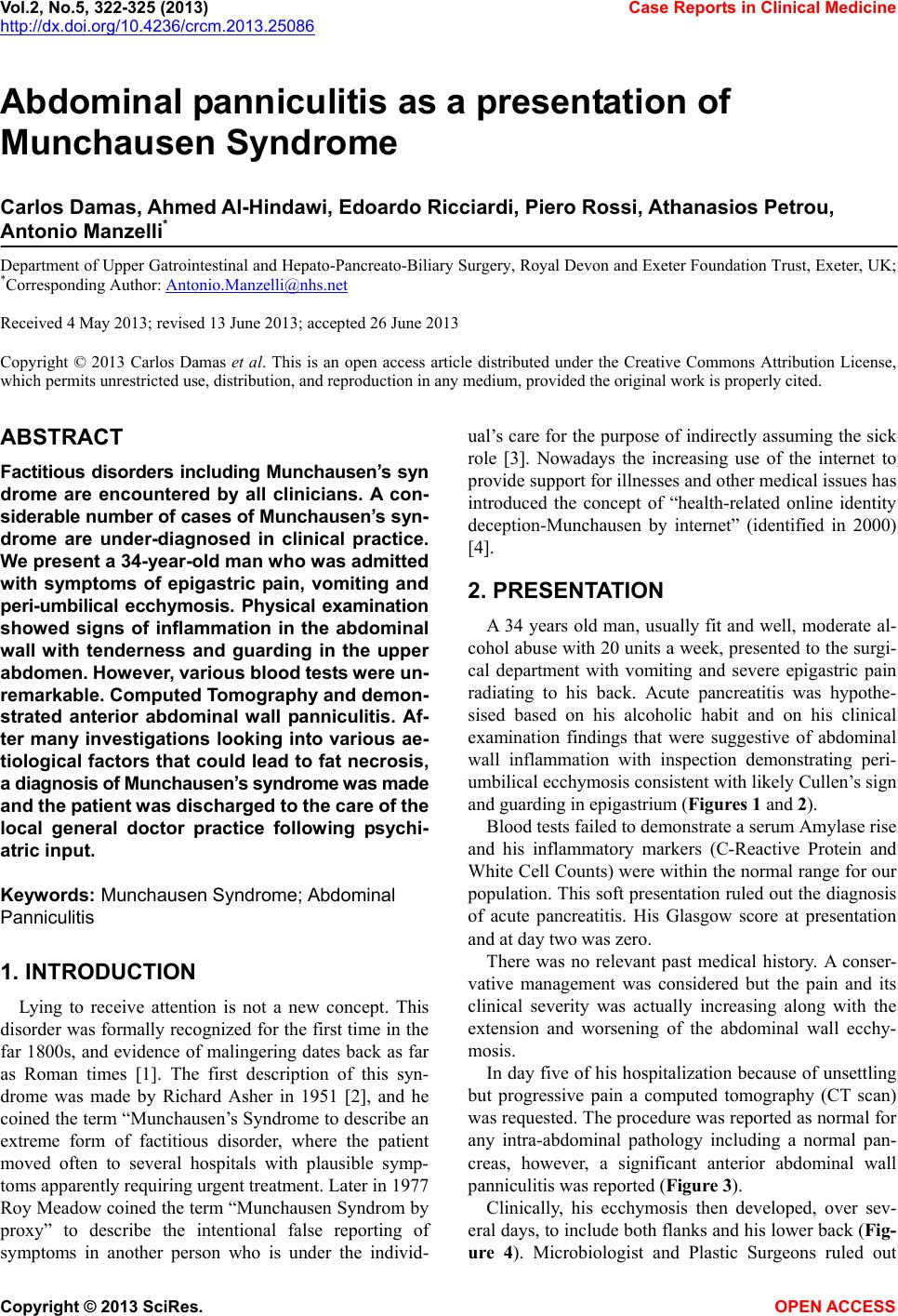
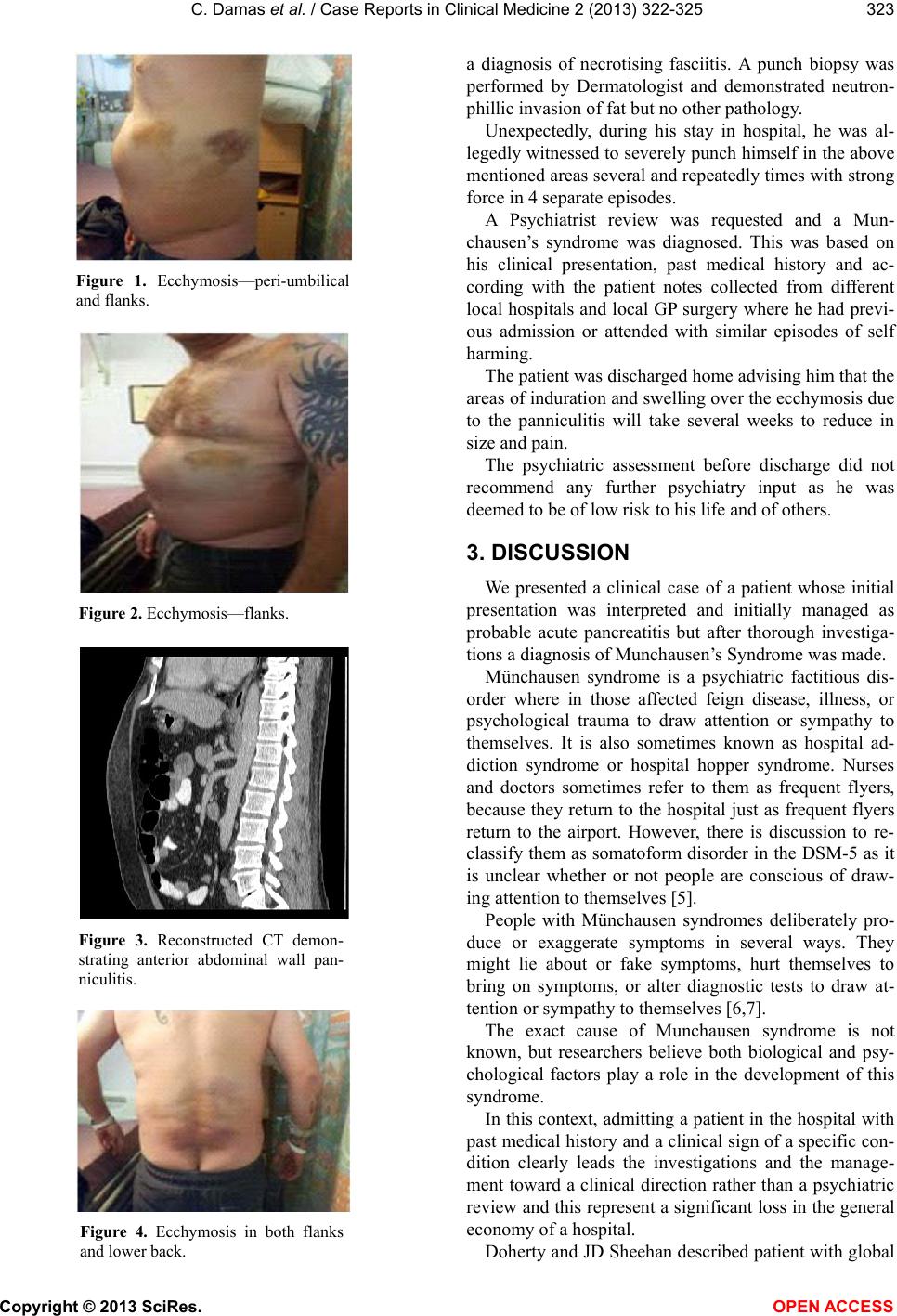
In our case, the peri-umbilical ecchymosis which were
thought to be Cullen’s sign helped actually to rule out the
diagnosis of pancreatitis as this sign is associated with
severe pancreatitis and was not compatible with the soft
clinical presentation of our patient [20].
In conclusion, this brief report describes an atypical
presentation of Munchausen Syndrome which misleads
the clinicians producing a false diagnosis of acute pan-
creatitis [21]. This resulted in 10 days of investigations
and hospitalization that incurred a considerable waste of
professional time at huge economic and financial costs. A
high index of suspicion for mental illness is urged in pa-
tients who present with this picture.
REFERENCES
[1] Andy, P. and Jacqui, T. (2012) Munchausen by Internet:
Current research and future directions. Journal of Medi-
cal Internet Research, 14, e115.
doi:10.2196/jmir.2011
[2] Asher, R. (1951) Munchausen’s syndrome. Lancet, 10,
339-341. doi:10.1016/S0140-6736(51)92313-6
[3] Steel, R.M. and Coll, J.R. (2009) Factitious disorder
(Munchausen syndrome). Physicians of Edinburgh, 39,
343-347. doi:10.4997/JRCPE.2009.412
[4] Feldman, Md. (2003) Munchausen by internet: Decting
factitious illness and crisis on the internet. Southern
Medical Journal, 93, 669-672.
[5] Feldman, M. (2004) Playing sick? Untangling the web of
Münchausen syndrome, Münchausen by proxy, malin-
gering & factitious disorder. Brunner-Routledge, Phila-
delphia.
[6] Folks, D.G. (1995) Munchausen’s syndrome and other
factitious disorders. Neurologic Clinics, 13, 267-281.
[7] Kanaan, R.A. and Wessely, S.C. (2010) Factitious disor-
ders in neurology: An analysis of reported cases. Psycho-
somatics, 51, 47-54.
[8] Doherty, A.M. and Sheehan, J.D. (2010) Munchausen’s
syndrome—More common than we realise? Irish Medical
Journal, 103, 179-181.
[9] Faida, A., Khanfir Monia, S., Amira, H., Imed, B.G.,
Mounir, L. and Mohamed Habib, H. (2012) A rare cause
of lobular panniculitis: Munchausen’s syndrome. Case
Reports in Medicine, 2012, Article ID: 486421.
doi:10.1155/2012/486421
[10] Goto, Y., Sasajima, H., Aita, K., Furuno, Y., Owada, K.,
Tatsuzawa, K., Inoue, Y. and Mineura, K. (2011) Mun-
chausen syndrome, a factitious injury, presenting brain
abscess and intraventricular hemorrhage: A case report.
No Shinkei Geka, 39, 381-386.
[11] Falagas, M.E., Christopoulou, M., Rosmarakis, E.S. and
Vlastou, C. (2004) Munchausen’s syndrome presenting as
severe panniculitis. International Journal of Clinical Prac-
Copyright © 2013 SciRes. OPEN ACCESS