Cerebral Infarction after Spine Surgery: Report of Two Cases
Copyright © 2013 SciRes. OJO
205
Multiple regression, multiple logistic regression and
discriminant analyses were performed. The multiple lo-
gistic regression analysis was performed with binary
variables established using a cut-off value (Table 2).
Analyses were conducted using EXCEL Statistics (Social
Survey Research Information Co., Ltd., Tokyo, Japan)
for multiple logistic and multiple regression analyses and
SPSS (IBM SPSS Statistics version 19, IBM Japan Ltd.,
Tokyo, Japan) for discriminant analysis.
3. Case Report
Case 1: The patient was a 83-year old man with cervical
spondylotic myelopathy and lumbar spinal stenosis who
underwent simultaneous cervical and lumbar laminoplasty.
The surgical time was 290 min and the bleeding volume
was 295 g. He had a history of prostatic hyperplasia and
gastric ulcer. Blood pressure on rising on the operative
day was 134/74 mmHg and that on extubation was 184/
104 mmHg, giving a systolic blood pressure ratio (pre-
operative/extubation) of 0.73. Dysarthria occurred on
extubation and arousal from anesthesia. Brain MRI was
performed immediately and showed brainstem infarction,
for which neuroprotective drugs were administered. Re-
habilitation for swallowing was also started because dys-
phagia occurred. The symptoms gradually improved and
the patient had no disturbance of activities of daily living
(ADL) at about 6 months after surgery.
Case 2: The patient was a 76-year old man with cer-
vical spondylotic amyotrophy who underwent forami-
notomy. The surgical time was 132 min and the bleeding
volume was 130 g. He had a history of diabetes and ce-
rebrovascular disorder, but had not taken drugs for cere-
brovascular disorder. Blood pressure on rising on the
operative day was 132/62 mmHg and that on extubation
was 177/100 mmHg. The systolic blood pressure ratio
(preoperative/extubation) was 0.75. Marked dysarthria
was found in arousal from anesthesia. Brain MRI was
performed immediately and minor infarction was found
in the midbrain, for which neuroprotective drugs were
administered. The symptoms gradually improved and the
patient had no disturbance of ADL at about 6 months
after surgery.
Table 2. Binary variables.
Age (0: <79 years old; 1≧
: 79 years old)
BMI (0: <25; 1: ≧25)
Systolic blood pressure ratio (on rising/on extubation)
(0: blood pressure ratio < ≧
0.8; 1: blood pressure ratio 0.8)
Diastolic blood pressure ratio (on rising/on extubation)
(0: blood pressure ratio < 0.8; 1≧
: blood pressure ratio 0.8)
Surgical time (0≧
: <150 min; 1: 150 min)
Bleeding volume (0: <300 mL; 1≧
: 300 mL)
4. Results
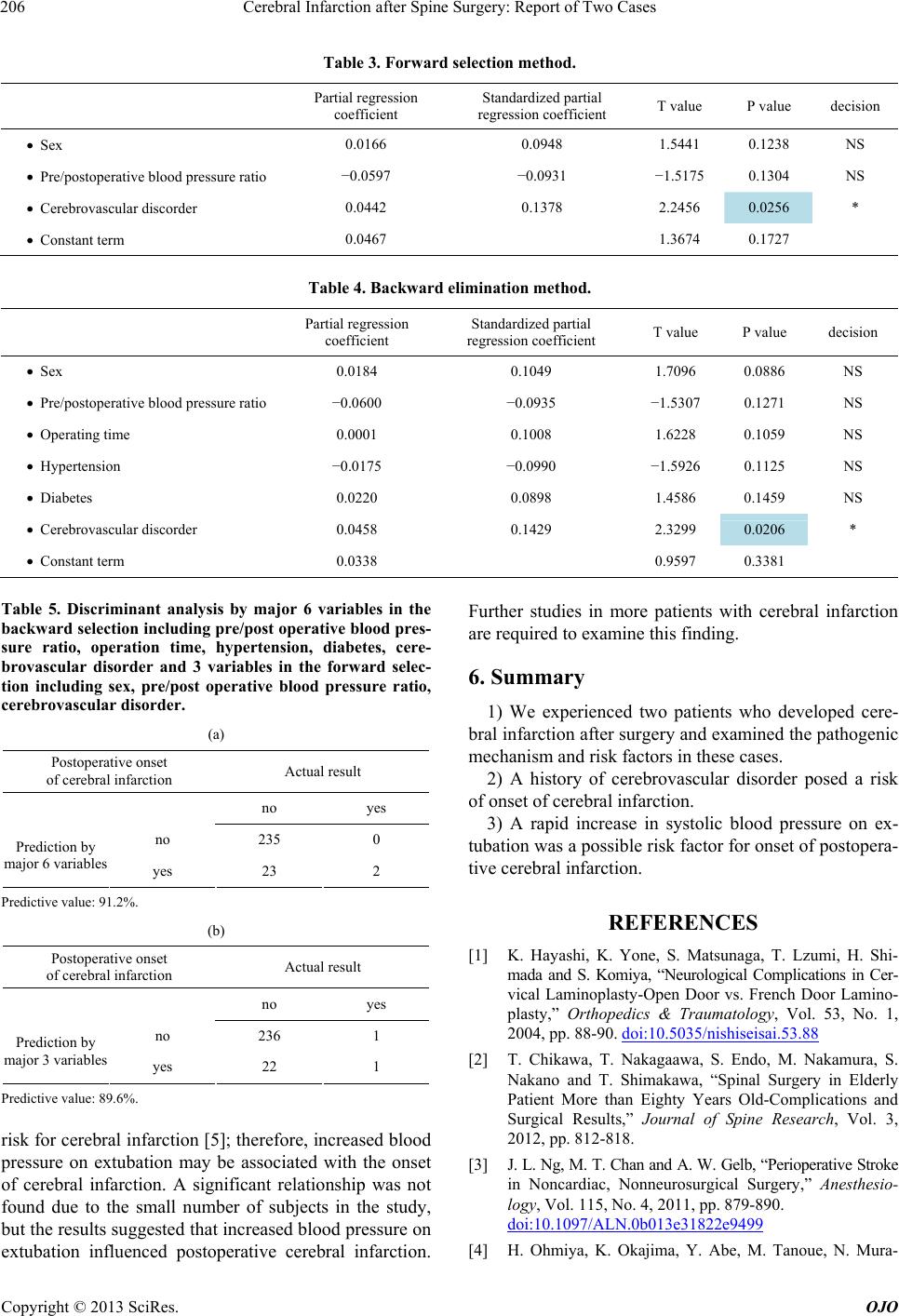
Multiple regression analysis was conducted using the
stepwise selection method. Forward selection identified
sex, low systolic blood pressure ratio (preoperative/ex-
tubation), and a history of cerebrovascular disorder as
potentially important variables, but only a history of ce-
rebrovascular disorder was significant (p = 0.025) (Table
3). Backward elimination identified these variables and
surgical time, bleeding volume and history of hyperten-
sion, but similarly the only significant variable was a
history of cerebrovascular disorder (p = 0.021) (Table
4).
In multiple logistic regression analysis, the only sig-
nificant risk factor was a history of cerebrovascular dis-
order alone. In discriminant analysis, the 3 and 6 vari-
ables extracted in the respective multiple regression ana-
lyses were used for prognosis prediction. The predictive
value, sensitivity and specificity of the 3 variables were
lower than those of the 6 variables, indicating that the
latter were effective for prediction of prognosis (Table 5).
The findings were not significant because data were
available for only 2 subjects with postoperative cerebral
infarction, but these results support the findings from
multiple regression analysis.
5. Discussion
The incidence of cerebral infarction after spinal surgery
ranges from 0.3% to 1% [1,2]. In our department, 2 of
1833 patients (approx. 0.1%) developed cerebral infarc-
tion and the outcomes were better than those in previous
case reports. The results of the study indicate that a his-
tory of cerebral infarction posed a risk for perioperative
cerebral infarction, as also found in other case reports. A
history of transient ischemic attack (TIA) is also a risk
for perioperative cerebral infarction, and surgery 1 to 3
months after cerebral infarction should be avoided [3].
Continuous administration of anticoagulant and anti-
platelet drugs causes no serious hemorrhagic complica-
tion and decreases the risk for perioperative cerebral in-
farction [4]. However, in our department, drug admini-
stration is usually discontinued 1 to 2 weeks before sur-
gery and postoperative administration is resumed after
extubation. The two patients with cerebral infarction were
not given anticoagulant or antiplatelet drugs before sur-
gery. Therefore, this issue was not examined in this study,
but should be investigated in the future.
The onset of cerebral infarction was thought to have
occurred during surgery in both cases. In our hospital,
systolic blood pressure is controlled at ≤100 mmHg dur-
ing surgery when possible to prevent intraoperative
bleeding; however, a rapid increase in systolic blood
pressure on extubation occurs in all patients. Reduction
in perioperative variation of blood pressure decreases the