Causes of Surgical Delay and Demographic Characteristics in Patients with Hip Fracture
Copyright © 2013 SciRes. OJO
197
believe that our study could contribute to future actions
and measurements, in order to further optimize the health
care program for these patients and a prospective study
might be useful in order to better identify the causes of
the surgical delay.
5. Conclusion
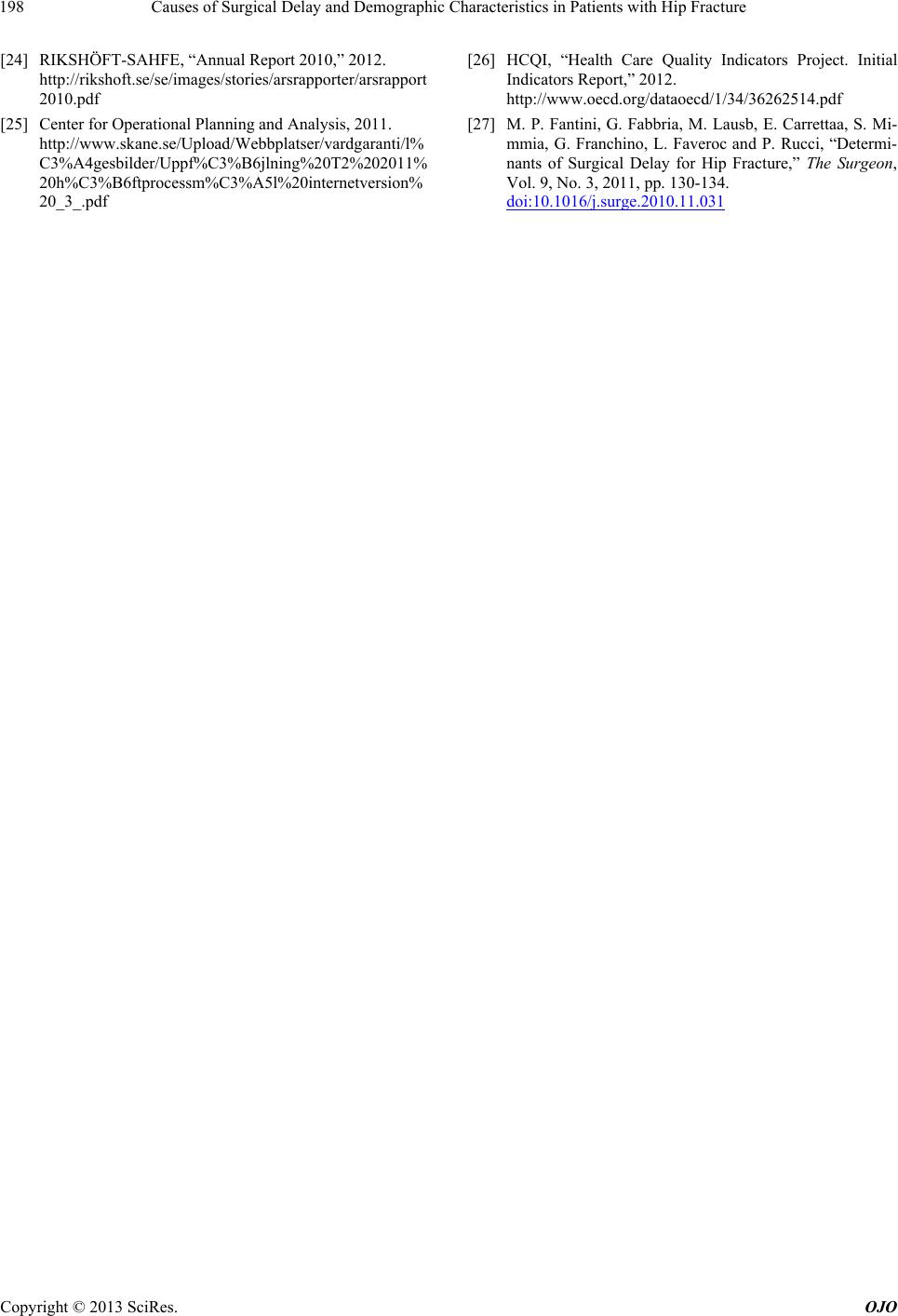
The causes of delay to surgery within 24 hours occurred
in 29.4% of all patients with hip fracture. The main rea-
sons for delays were lack of theatre facilities (54%),
medical unstable patient (16%) and anticoagulant treat-
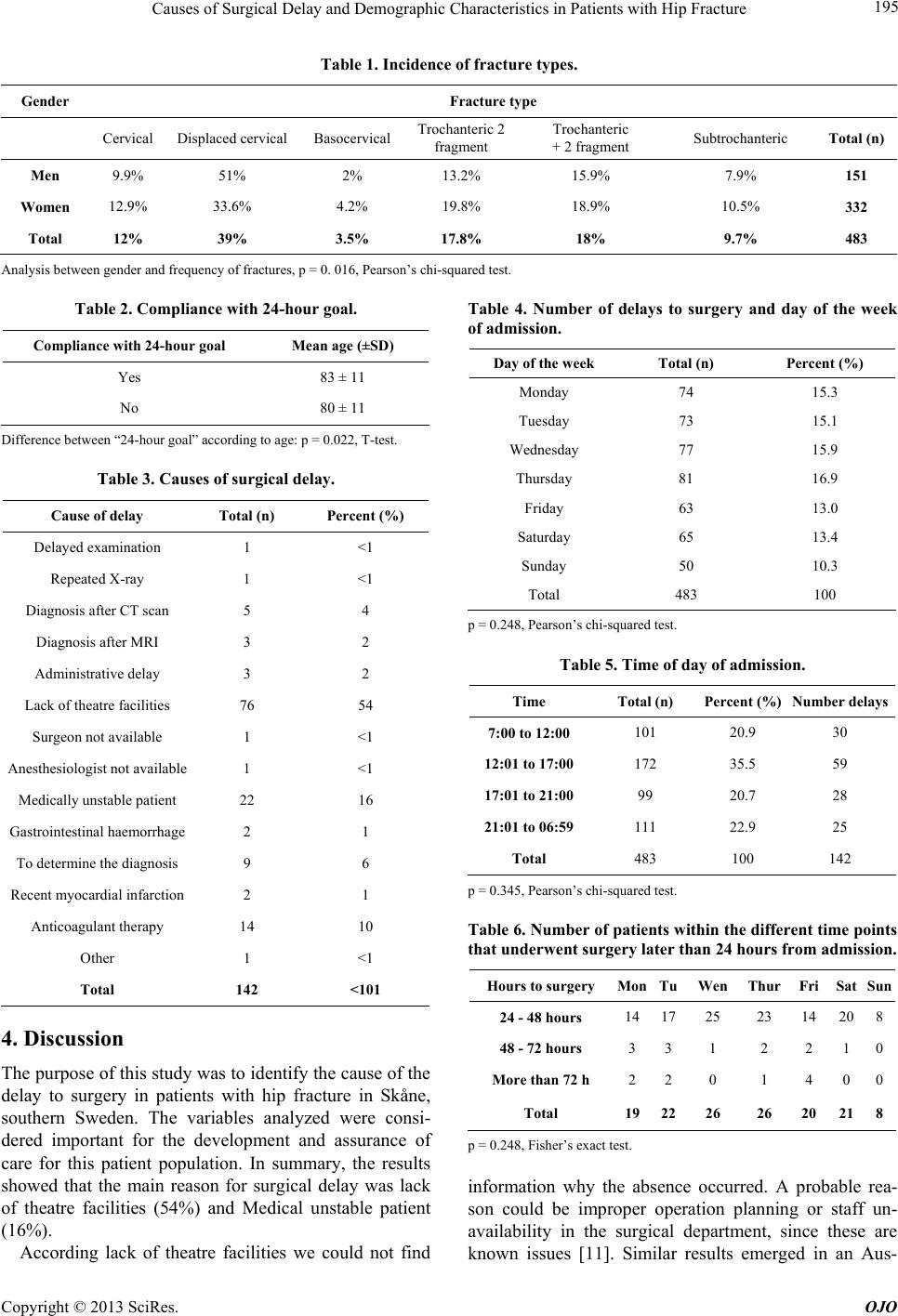
ment (10%). The most common type of hip fracture was
displaced cervical hip fracture (39%) with a majority of
fractures in male patients.
REFERENCES
[1] A. Hommel, “Improved Safety and Quality of Care for
Patients with a Hip Fracture,” Ph.D. Dissertation, Lunds
Universitet, Institutionen för Hälsa, Vård Och Samhälle,
2007.
[2] WHO, “Sweden: “Nutrition for Older Persons,” 2011.
www.who.int/nutrition/topics/ageing/en/index2.html
[3] V. Novack, A. Jotkowitz, O. Etzion and A. Porath, “Does
Delay in Surgery after Hip Fracture Lead to Worse Out-
comes? A Multicenter Survey,” International Journal for
Quality in Health Care, Vol. 19, No. 3, 2007, pp. 170-176.
doi:10.1093/intqhc/mzm003
[4] J.-E. Gjertsen, L.-B. Engesæter, O. Furnes, L.-I. Havelin,
K. Steindal, T. Vinje and J.-M. Fevang, “The Norwegian
Hip Fracture Register Experiences after the First 2 Years
and 15,576 Reported Operations,” Acta Orthopaedia, Vol.
79, No. 5, 2008, pp. 583-583.
doi:10.1080/17453670810016588
[5] National Board of Health and Welfare, “Sweden: Fall-
skador i Vården,” 2011.
http://www.socialstyrelsen.se/patientsakerhet/riskomrade
n/fallskador
[6] RIKSHÖFT, “Sweden: Höftfrakturer; 2009a,” 2009.
http://www.rikshoft.se/se/index.php?option=com_content
&view=article&id=50&Itemid=37
[7] J. Richmond, G.-B. Aharonoff, J.-D. Zuckerman and K.-J.
Koval, “Mortality Risk after Hip Fracture,” Journal of
Orthopaedic Trauma, Vol. 17, No. 1, 2003, pp. 53-56.
doi:10.1097/00005131-200301000-00008
[8] P. Vestergaard, L. Rejnmark and L. Mosekilde, “Increased
Mortality in Patients with a Hip Fracture-Effect of Pre-
Morbid Conditions and Post-Fracture Complications,”
Osteoporosi International, Vol. 18, No. 12, 2007, pp.
1583-1593. doi:10.1007/s00198-007-0403-3
[9] A. Hommel, K. Ulander, K. B. Björkelund, P.-O. Norman,
H. Wingstrand and K.-G. Thorngren, “Influence of Opti-
mised Treatment of People with Hipfracture on Time to
Operation, Length of Hospital Stay, Reoperations and
Mortality within 1 Year,” International Journal of the
Care of the Injured, Vol. 39, No. 10, 2008, pp. 1164-1174.
doi:10.1016/j.injury.2008.01.048
[10] S.-K. Khan, S. Kalra, M. M. Thiruvengada and M. J.
Parker, “Timing to Surgery for Hip Fractures: A System-
atic Rewiew of 52 Published Studies Involving 291,413
Patients,” International Journal of the Care of the Injured,
Vol. 40, No. 7, 2009, pp. 692-697.
doi:10.1016/j.injury.2009.01.010
[11] N. Simunovic, P. J. Devereaux and M. Bhandari, “Sur-
gery for Hip Fractures: Does Surgical Delay Affect Out-
comes?” Indian Journal Orthopaedia, Vol. 45, No. 1,
2011, pp. 27-32. doi:10.4103/0019-5413.73660
[12] K. B. Björkelund, “Acute Confusional State in Elderly Pa-
tients with Hip Fracture. Identification of Risk factors and
Intervention Using a Prehospital and Perioperative Man-
agement Program,” Ph.D. Dissertation, Lunds Universitet,
Institutionen för Hälsa, Vård Och Samhälle, 2008.
[13] RIKSHÖFT, “Sweden: Om Rikshöft; 2009b,” 2011.
http://www.rikshoft.se/se/index.php?option=com_content
&view=article&id=46&Itemid=27
[14] A. Bottle and P. Aylin, “Mortality Associates with Delay
in Operation after Hip Fracture: Observational Study,”
British Medical Journal, Vol. 332, No. 7547, 2006, pp.
947-951. doi:10.1136/bmj.38790.468519.55
[15] J. Librero, S. Peiró, E. Leutscher, J. Merlo, E. Bernal-
Delgado, M. Ridao, N. Martínez-Lizaga and G. Sanfélix-
Gimeno, “Timing of Surgery for Hip Fracture and In-Hos-
pital Mortality: A Retrospective Population-Based Cohort
Study in the Spanish National Health System,” BMC
Health Services Research, Vol. 12, No. 15, 2012.
doi:10.1186/1472-6963-12-15
[16] C. R. Hamish, I. A. Harris, L. Mcevoy and T. Todovora,
“Delay to Surgery and Mortality after Hip Fracture,” The
Australian and New Zealand Journal of Surgery, Vol. 77,
No. 10, 2007, pp. 889-891.
doi:10.1111/j.1445-2197.2007.04267.x
[17] RIKSHÖFT-SAHFE, “Annual Report 2009,” 2012.
http://rikshoft.se/se/images/stories/arsrapporter/arsrapport
2009.pdf
[18] K. B. Björkelund, A. Hommel, K.-G. Thorgren, L. Gus-
tafson, S. Larsson and D. Lundberg, “Reducing Delirium
in Elderly Patients with Hip Fracture: A Multi-Factorial
Intervention Study,” Acta Anaesthesiologica Scandinavia,
Vol. 54, No. 6, 2010, pp. 678-688.
doi:10.1111/j.1399-6576.2010.02232.x
[19] National Board of Health and Welfare, “Guidelines for
Care and Treatment in Patients with Hip Fracture,” So-
cialstyrelsen, Stockholm, 2003.
[20] RIKSHÖFT-SAHFE, “Annual Report 2005,” 2011.
http://rikshoft.se/se/images/stories/arsrapporter/Arsrappor
t2005.pdf
[21] RIKSHÖFT-SAHFE, “Annual Report 2006,” 2011.
http://rikshoft.se/se/images/stories/arsrapporter/Arsrappor
t2006.pdf
[22] RIKSHÖFT-SAHFE, “Annual Report 2007,” 2011.
http://rikshoft.se/se/images/stories/arsrapporter/Arsrappor
t2007.pdf
[23] RIKSHÖFT-SAHFE, “Annual Report 2008,” 2011.
http://www.rikshoft.se/se/images/stories/arsrapporter/Arsr
apport2008.pdf