M. Cetin et al. / Case Reports in Clinical Medicine 2 (201 3) 315-317
Copyright © 2013 SciRes. OPEN ACCESS
317
[2] Zaoutis, T.E., Heydon, K., Localio, R., Walsh, T.J. and
Feudtner, C. (2007) Outcomes attributable to neonatal can-
didiasis. Clinical Infectious Diseases, 44, 1187-1193.
doi:10.1086/513196
shown to be an effective approach to the treatment o f th is
complication [10]. Use of prolonged anti-fungal treat-
ment alone is reported in few critically ill infants with
fungal endocarditis [11]. In our case, due to high risk of
mortality for cardiopulmoner bypass, only 60 days lipo-
somal amphotericin B therapy was administered. Due to
intracranial hemorrhage risk n o anticoagu lant and throm-
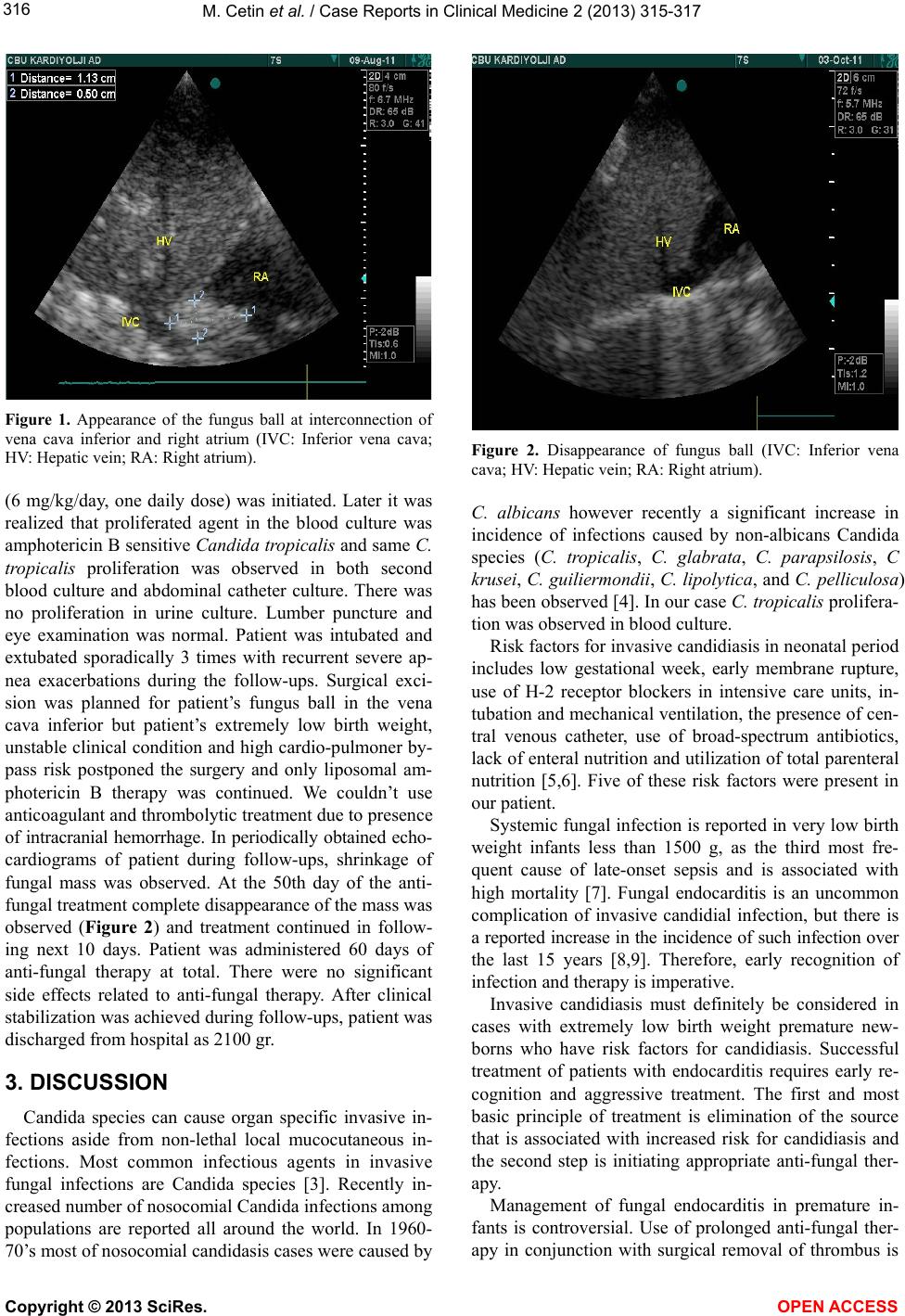
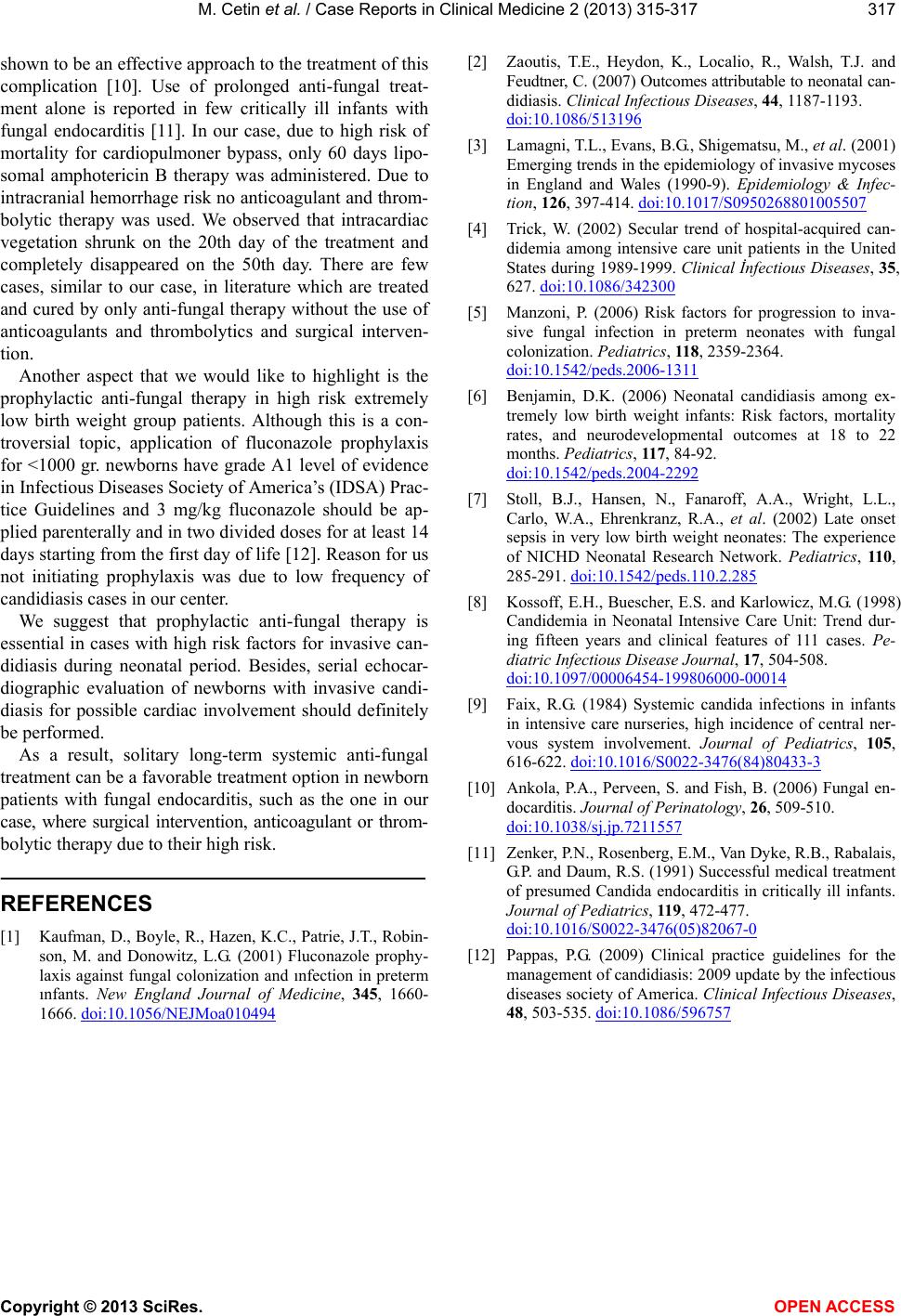
bolytic therapy was used. We observed that intracardiac
vegetation shrunk on the 20th day of the treatment and
completely disappeared on the 50th day. There are few
cases, similar to our case, in literature which are treated
and cured by only anti-fungal therapy without the use of
anticoagulants and thrombolytics and surgical interven-
tion.
[3] Lamagni, T.L., Evans, B.G., Shigematsu, M., et al. (2001)
Emerging trends in the epidemiology of invasive mycoses
in England and Wales (1990-9). Epidemiology & Infec-
tion, 126, 397-414. doi:10.1017/S0950268801005507
[4] Trick, W. (2002) Secular trend of hospital-acquired can-
didemia among intensive care unit patients in the United
States during 1989-1999. Clinical İnfectious Diseases, 35,
627. doi:10.1086/342300
[5] Manzoni, P. (2006) Risk factors for progression to inva-
sive fungal infection in preterm neonates with fungal
colonization. Pediatrics, 11 8, 2359-2364.
doi:10.1542/peds.2006-1311
Another aspect that we would like to highlight is the
prophylactic anti-fungal therapy in high risk extremely
low birth weight group patients. Although this is a con-
troversial topic, application of fluconazole prophylaxis
for <1000 gr. newborns have grade A1 level of evidence
in Infectious Diseases Society of America’s (IDSA) Prac-
tice Guidelines and 3 mg/kg fluconazole should be ap-
plied parenterally and in two divided doses for at least 14
days starting from the first day of life [12]. Reason for us
not initiating prophylaxis was due to low frequency of
candidiasis cases in our center.
[6] Benjamin, D.K. (2006) Neonatal candidiasis among ex-
tremely low birth weight infants: Risk factors, mortality
rates, and neurodevelopmental outcomes at 18 to 22
months. Pediatrics, 117, 84-92.
doi:10.1542/peds.2004-2292
[7] Stoll, B.J., Hansen, N., Fanaroff, A.A., Wright, L.L.,
Carlo, W.A., Ehrenkranz, R.A., et al. (2002) Late onset
sepsis in very low birth weight neonates: The experience
of NICHD Neonatal Research Network. Pediatrics, 110,
285-291. doi:10.1542/peds.110.2.285
[8] Kossoff, E.H., Buescher, E.S. and Karlowicz, M.G. (1998)
Candidemia in Neonatal Intensive Care Unit: Trend dur-
ing fifteen years and clinical features of 111 cases. Pe-
diatric Infectious Disease Journal, 17, 504-508.
doi:10.1097/00006454-199806000-00014
We suggest that prophylactic anti-fungal therapy is
essential in cases with high risk factors for invasive can-
didiasis during neonatal period. Besides, serial echocar-
diographic evaluation of newborns with invasive candi-
diasis for possible cardiac involvement should definitely
be performed.
[9] Faix, R.G. (1984) Systemic candida infections in infants
in intensive care nurseries, high incidence of central ner-
vous system involvement. Journal of Pediatrics, 105,
616-622. doi:10.1016/S0022-3476(84)80433-3
As a result, solitary long-term systemic anti-fungal
treatment can be a favorable treatment option in newborn
patients with fungal endocarditis, such as the one in our
case, where surgical intervention, anticoagulant or throm-
bolytic therapy due to their high risk.
[10] Ankola, P.A., Perveen, S. and Fish, B. (2006) Fungal en-
docarditis. Journal of Perinatology, 26, 509-510.
doi:10.1038/sj.jp.7211557
[11] Zenker, P.N., Rosenberg, E.M., Van Dyke, R.B., Rabalais,
G.P. and Daum, R.S. (1991) Successful medical treatment
of presumed Candida endocarditis in critically ill infants.
Journal of Pediatrics, 11 9, 472-477.
doi:10.1016/S0022-3476(05)82067-0
REFERENCES
[1] Kaufman, D., Boy le, R., Hazen, K.C., Patrie, J. T., Robin-
son, M. and Donowitz, L.G. (2001) Fluconazole prophy-
laxis against fungal colonization and ınfection in preterm
ınfants. New England Journal of Medicine, 345, 1660-
1666. doi:10.1056/NEJMoa010494
[12] Pappas, P.G. (2009) Clinical practice guidelines for the
management of candidiasis: 2009 update by the infectious
diseases society of America. Clinical Infectious Diseases,
48, 503-535. doi:10.1086/596757