Vol.2, No.5, 281-284 (2013) Case Reports in Clinical Medicine
http://dx.doi.org/10.4236/crcm.2013.25076
Case report of tubercular spondylodiscitis with
paraplegia managed by posterior transpedicular
decompression and pedicle screw fixation*
Paragjyoti Gogoi1#, Anshuman Dutta1, Vikash Agarwala1, Prasant a Sonowal2
1Department of Orthopaedics & Trauma , Silchar Medic al College, Silchar, India; #Corresponding Author: pggogoiparag@gmail.com
2Department of Anaesthesiology, Silchar Medical College, Silchar, India
Received 20 May 2013; revised 21 June 2013; accepted 25 July 2013
Copyright © 2013 Paragjyoti Gogoi et al. This is an open access article distributed under the Creative Commons Attribution License,
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
Pott’s paraplegia is still prevalent in this part of
the world. Early onset paraplegia can be im-
proved by timely surgical intervention under
ATT cover. The disease mostly affects the tho-
raco-lumbar spine. Classically, the diseased area
is addressed by anterior thoracic or thoraco-
lumbar approach and after curettage of the dis-
eased and necrotic material the anterior column
is reconstructed by rib or fibular strut graft or
metallic cage and supplemented by posterior
instrumentation and fusion. Laminectomy, as a
method of decompression, was greatly discour-
aged in spinal tuberculosis with compressive
myelopath y except in posterior element involve-
ment. We present a case of a 35 years old lady
with Pott’s paraplegia treated by hemilaminec-
tomy and transpedicular limited anterior decom-
pression of the cord and pedicle screw fixation
with fusion who improved vastly in terms of
motor power.
Keywords: Spinal TB; Pott’s Paraplegia; Adult;
Hemi-Laminectomy; Pedicle Screw; Fusion
1. INTRODUCTION
Spinal tuberculosis is still a cause of major morbidity.
Millions of people are still affected by this ailment. Be-
cause of the improved chemotherapy the mortality is
now reduced to a great extent. Many cases got improve-
ment by chemotherapy alone. Only some selected cases
require surgical treatment. Spinal tuberculosis is notori-
ous for producing spinal deformities and neurological
involvement like paraplegia. In such cases immediate
surgical intervention becomes necessary to regain normal
or useful motor function [1].
Pott’s paraplegia can occur due to compression of the
spinal cord by soft material like tubercular abscess, cas-
eous mass or granulation tissue or by hard material like
internal gibbus, bony sequestrum or a sequestrated disc.
We report a case of Spinal tubercu losis at D12 and L1
level presenting with paraplegia with bowel and bladder
involvement who regained completely normal motor
function and bowel and bladder control after posterior
decompression and stabilization with pedicle screw rod
system.
2. THE CASE REPORT
A lady of 35 years old presented to us with complete
loss of all motor function of her both lower limbs with
retention of urine and pain over the lower dorsal spine.
She had a history of back pain for one month associated
with fever off and on. She did not sustain any trauma
over the area nor was there any history of cough for
prolonged duration or significant weight loss.
On examination both the lower limbs were flaccid
with grade 0 motor power according to MRC grading.
She did not feel the sensation of bladder fullness. Her
sensation was diminished from L1 dermatome.
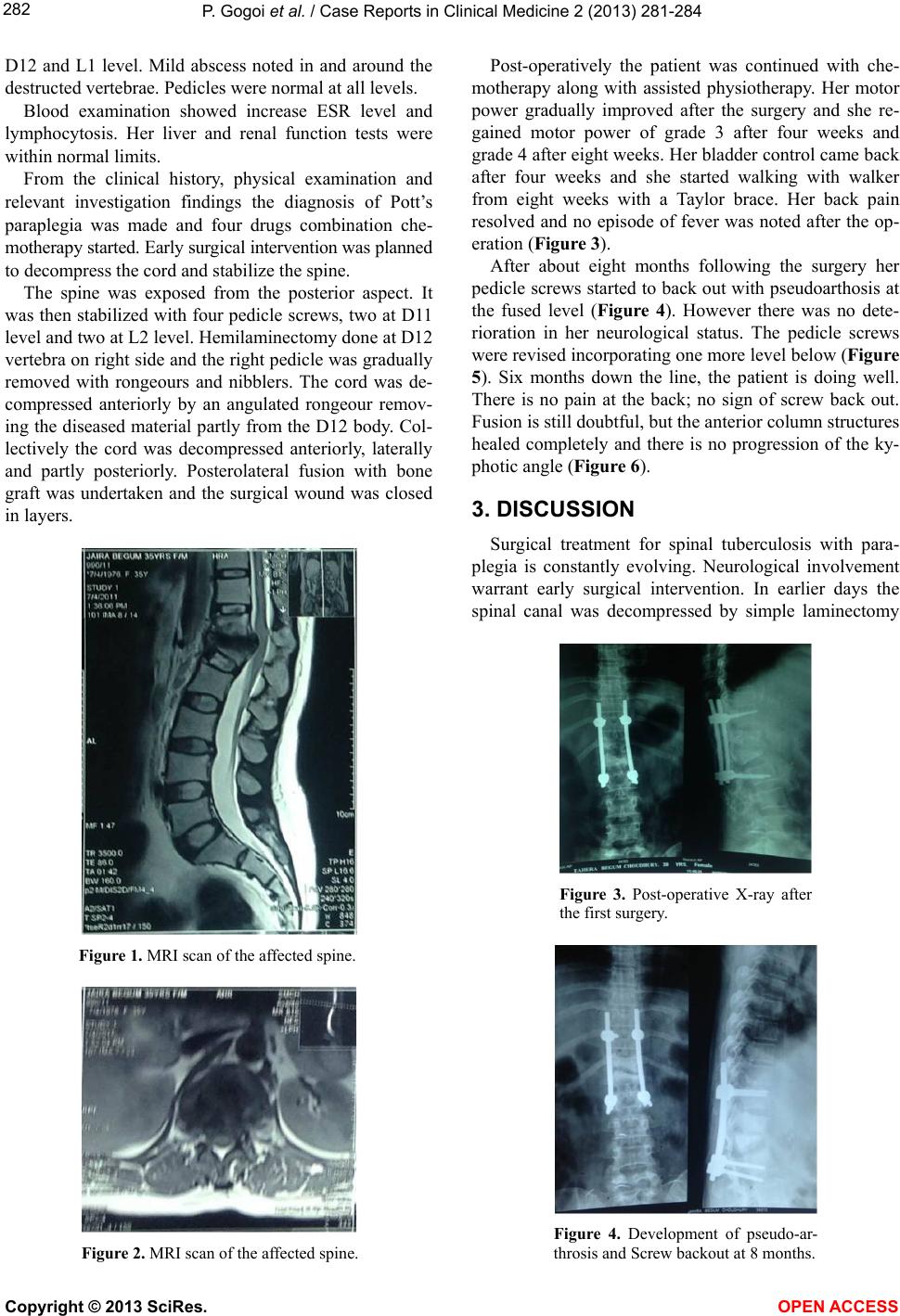
The spine examination revealed a kyphus deformity at
D12 and L1 level with mild tenderness. Wasting of para-
spinal muscles were also noted. Plain X-ray showed obli-
teration of D12, L1 disc space along with destruction of
inferior part of body of D12 and superior part of body of
L1 as well as wedging at that level. No obvious para-
spinal soft tissue shadow was noted.
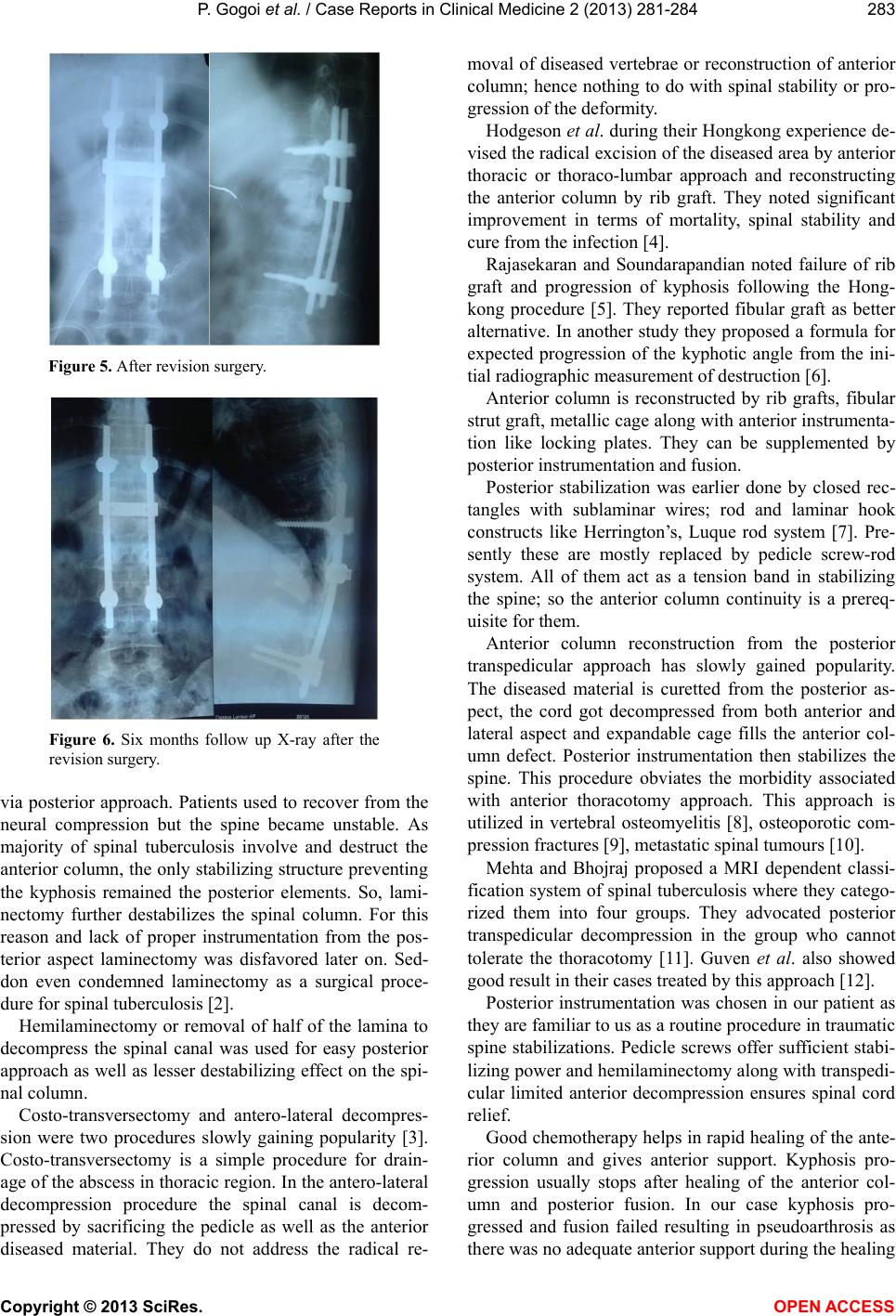
MRI scan of the Dorso-lumbar Spine confirmed the
X-ray findings (Figures 1 and 2). There was destruction
of the vertebrae with compression of the spinal cord at
*Consent: Informed consent obtained from the patient regarding pre-
sentation and publication of t h i s c a s e .
Copyright © 2013 SciRes. OPEN ACCESS