T. Abe et al. / Open Journal of Gastroenterology 3 (2013) 223-226 225
by sphincter division, removal can certainly be a primary
focus, which eliminates the risk of missing secondary
tracts and allows healing by secondary intention of
healthier tissue. Moreover, divided sphincters are fixed
to prevent reduction in anal resting tone. We have also
used this technique successfully to manage complex fis-
tulas, but the present study was limited to a more com-
mon group, simple fistulas.
Both fistulotomy and fistulectomy have long been ac-
cepted as the gold standard for simple fistulas. Although
fistulotomy has been associated with success rates of
92% - 97%, the procedure will result in some form of
incontinence even for simple fistulas in approximately
12% - 39% of patients [3,5,6].
Both fistulotomy and fistulectomy leaves the unepi-
thelialized wound opened, which may cause undesired
pain and complications, such as bleeding and suppura-
tion. Marsupializatio n of the unepithelialized wound was
introduced to provide the benefit of shortened healing
times and improved continence by minimizing anal de-
formity [10]. The addition of marsupialization also has
been associated with less postoperative pain and bleeding
[11]. However, this procedure leaves the sphincters di-
vided, and Pescatori et al. [11] did not observe any supe-
riority of marsupialization with respect to incontinence
rates.
Fistulectomy and immediate sphincter repair for low
fistulas, described by Parkash et al. [12], aim to eradicate
infection and to anatomically reconstruct the muscular
defect. However, very few studies have been published
on this technique. Dehiscence of sphincteroplasty is the
most fearful complication of this technique and is re-
sponsible for its infrequent use [13]. Roig et al. [14]
treated 75 patients in whom most of the fistulas were
complex (69%) by fistulectomy and end-to-end recon-
struction of the disrupted EAS. Five recurrences in total
have been described (6.7%), and the postoperative in-
continence rate was 21%. Perez et al. [13] included 16
patients with recurrent complex fistulas in whom fistu-
lotomy was performed with overlapping repair of the
disrupted EAS. Two (25%) of 8 fully continent patients
developed incontinence for watery stools and flatus,
which gave a recurrence rate of 6.3% (1 patient). By
overlapping the muscle, the area in contact is increased
and rupture of the sutures may be more unlikely. How-
ever, when the width of overlap is too long, the anal ca-
nal may narrow and drainage worsen.
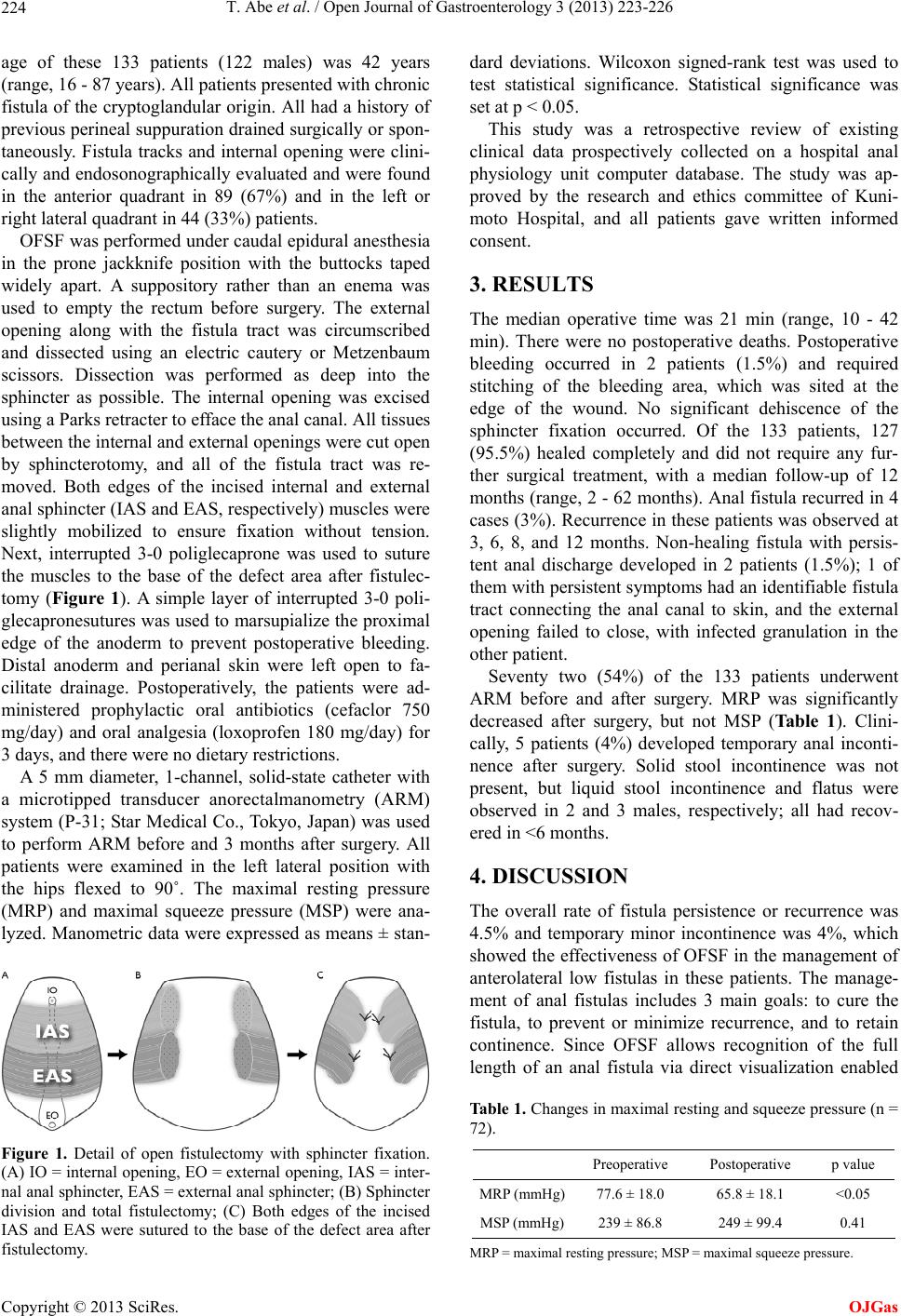
The strengths of sphincter fixation, our original me-
thod, are as follows: 1) since both edges of the sphincters
are sutured separately, the tension on the sutures can be
reduced by half relative to that on end-to-end sutures; 2)
extensive dissection of sphincter muscles is not needed
to achieve overlap; 3) the anal canal does not become
narrow as can occur with overlap. The edges of the di-
vided sphincter muscles will separate rapidly when they
are not at all repaired. Even if they are fixed in the origi-
nal position, continence will be fully maintainable. In
fact, it was found that sphincter fixation was better pre-
served for MSP 3 months after surgery. Although MRP
was significantly reduced, the extent was only 15%. Cli-
nically, 5 patients (4%) developed temporary inconti-
nence for liquids and gas, and all of them had recovered
in <6 months.
5. CONCLUSION
The true advantages of the OFSF procedure may not be
clear until larger prosp ective rando mized studies are co n-
ducted. However, considering the current reported data,
we believe that OFSF can achieve complete removal of
fistulas safely and easily with minimal risk of post-
operative incontinence and low recurrence rates.
REFERENCES
[1] Parks, A.G. (1961) Pathogenesis and treatment of fis-
tula-in-ano. British Medical Journal, 1, 463-469.
doi:10.1136/bmj.1.5224.463
[2] Parks, A.G., Gordon, P.H. and Hardcastle, J.D. (1976) A
classification of fistula-in ano. British Journal of Surgery,
63, 1-12. doi:10.1002/bjs.1800630102
[3] Garcia-Aguilar, J., Belmonte, C., Wong, W.D., et al.
(1996) Anal fistula surgery. Factors associated with re-
currence and incontinence. Disease of the Colon and
Rectum, 39, 723-729. doi:10.1007/BF02054434
[4] Parks, A.G. and Stitz, R.W. (1976) The treatment of high
fistula-in-ano. Disease of the Colon and Rectum, 19, 487-
499. doi:10.1007/BF02590941
[5] Davies, M., Harris, D. and Lohana, P. (2008) The sur-
gical management of fistula-in-ano in a specialist colo-
rectal unit. International Journal of Colorectal Disease,
23, 833-838. doi:10.1007/s00384-008-0444-x
[6] Roig, J.V., Jordan, J., Garcia-Armengol, J., et al. (2009)
Change in anorectal morphologic and functional parame-
ters after fistula-in-ano surgery. Disease of the Colon and
Rectum, 52, 1462-1469.
doi:10.1007/DCR.0b013e3181a80e24
[7] Atkin, G.K., Martins, J., Tozer, P., et al. (2011) For many
high anal fistulas, lay open is still a good option. Tech-
niques in Coloproctology, 15, 143-150.
doi:10.1007/s10151-011-0676-6
[8] Steele, S.R., Kumar, R., Feingold, D.L., et al. (2011)
Practice parameters for the management of perianal ab-
scess and fistula-in-ano. Disease of the Colon and Rectum,
54, 1465-1474. doi:10.1097/DCR.0b013e31823122b3
[9] Iwadare, J. (2000) Sphincter-preserving techniques for
anal fistulas in Japan. Disease of the Colon and Rectum,
43, S69-S77. doi:10.1007/BF02237229
[10] Ho, Y.H., Tan, M., Leong, A.F.P.K., et al. (1998) Marsu-
pialization of fistulotomy wounds improves healing: A
randomized controlled trial. British Journal of Surgery,
Copyright © 2013 SciRes. OJGas