Paper Menu >>
Journal Menu >>
 Journal of Cancer Therapy, 2010, 1, 174-180 doi:10.4236/jct.2010.14027 Published Online December 2010 (http://www.scirp.org/journal/jct) Copyright © 2010 SciRes. JCT Management and Outcomes in Primary Tumors of the Appendix Richard K. Englehardt, Noreen K. Durrani, Vijay K. Mittal Department of Surgery, Providence Hospital and Medical Centers, Southfield, USA. Email: Richard.Englehardt@providence-stjohnhealth.org Received: August 9th, 2010; revised August 15th, 2010; accepted August 23rd, 2010. ABSTRACT Primary tumors of the appendix are rare, comprising 1.1% of all appendectomy specimens. Nevertheless, it often pre- sents in an emergent fashion, creating a need for a well-defined management algorithm that will ensure proper acute management. We performed a retrospective review of medical charts from 1982-2007 on all charts with a diagnosis o f appendiceal neoplasm. A cohort of 41 patients was diagnosed with a primary appendiceal neoplasm from a total of 8560 appendectomies over the 25-year period. Several tumors were identified: adenocarcinomas (n = 16), carcinoid tumors (n = 15), mucinous cystadenocarcinoma (n = 7), and a combination of adenocarcinoma and goblet cell carci- noid of the appendix (n = 3). Twenty-one patients presented with an acute abdomen. Tumors were discovered intraop- eratively in eighteen patients while performing other procedures. At diagnosis, metastatic disease was found in 41.5% of patients (n = 17); average survival ranged from 6 to 21 months based on tumor type. For patients with non-metastatic disease at diagnosis, all survived longer than 2 years and there were no cases of recurrence or post-operative metastasis. We devised an operative strategy dictated by initial presenting characteristics of the tumor. The presence of carcinoma should be suspected and searched for in patients over 40 presenting with acute appendicitis. Intraoperatively any suspicious mass should undergo frozen sectioning as the finding of a malignancy often necessitates a larger or repeat operation. The propensity of these neoplasms for presentation in the guise of acute appendicitis mandates that the surgeon be familiar with the appropriate management algorithm, both in and out of the operating room. Keywords: Appendix Cancer, Gastrointestinal Malignancy, Malignant Neoplasms of the Appendix 1. Introduction Primary tumors of the appendix are rare. However, statis- tics show that one of the most common surgical emergen- cies in the United States today is still appendicitis [1]. Since the pathophysiology of appendicitis was first de- scribed in 1886 by Raymond Fitz, multiple etiologies of appendicitis have been discovered, ranging from obstruc- tion via fecalith to obstruction with tumor [2]. Current management strategies described in the literature advocate aggressive right colonic resections for most tumor types. These recommendations are often based on data extrapo- lated from primary colonic tumors of similar histology. The objective of our study was to review our experience with primary tumors of the appendix, compare our man- agement strategies with the other common management strategies described in the current literature, and use this information to better define an accepted management algorithm for primary appendiceal tumors. 2. Methods All appendectomies performed at Providence Hospital and Medical Centers over a 25-year period from March 1982 to December 2007 were reviewed. Those patients with chart codes positive for appendiceal tumors were reviewed in detail. Only primary neoplasms of the ap- pendix were analyzed. Patients with histology consistent with adenocarcinoma, carcinoid, mucinous cystadeno- carcinoma, and mixed adenocarcinoid tumors were fur- ther evaluated. Patients with benign neoplasms and pa- tients with metastatic disease to the appendix with a sep- arate primary were not included in the study. Factors catalogued in the patients incorporated in the study in- cluded presenting symptoms, method of diagnosis, epi- demiologic data, preoperative imaging, laboratory studies, intraoperative findings, operation performed, pathology results, use of postoperative chemotherapy, and eventual outcomes. 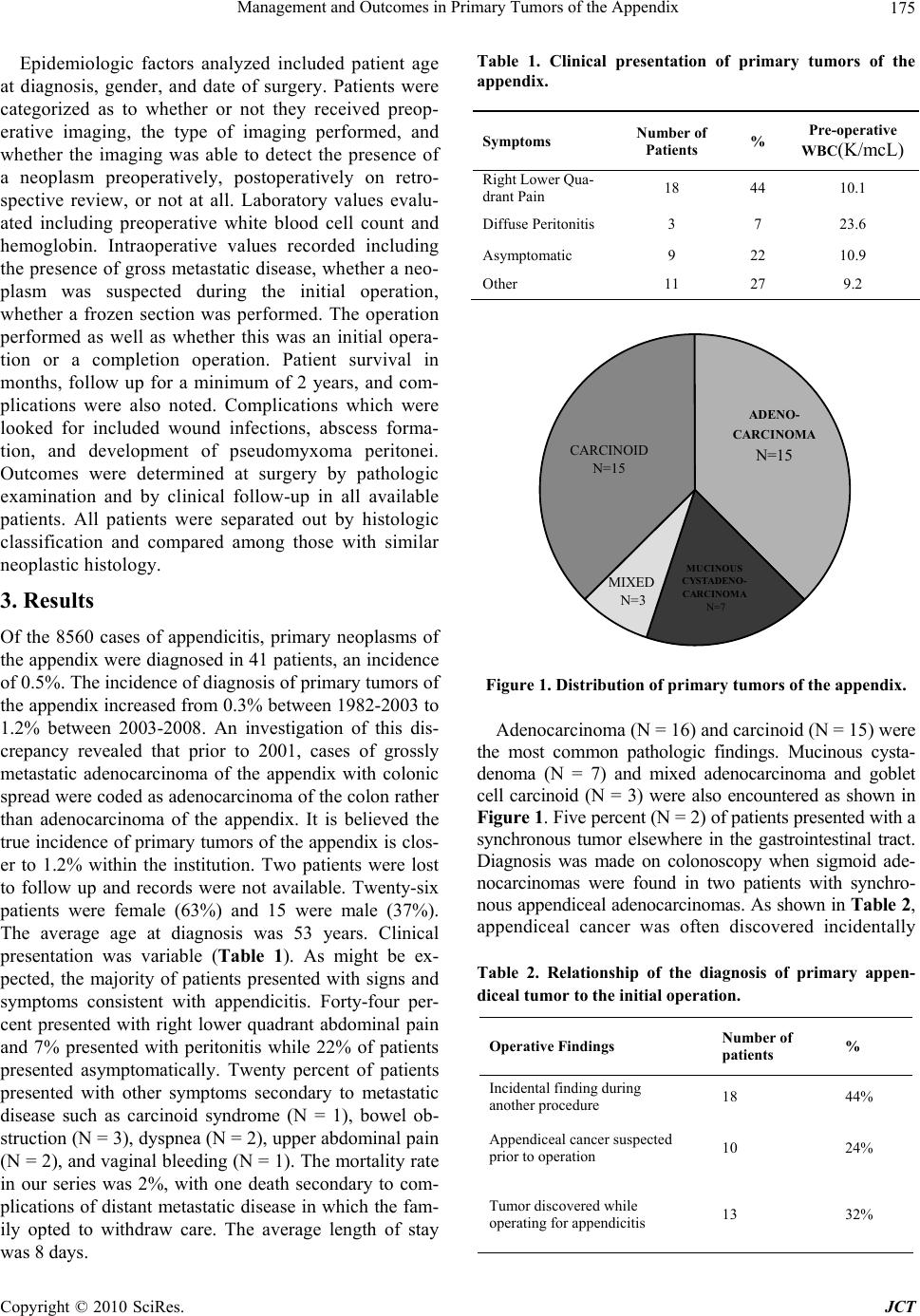 Management and Outcomes in Primary Tumors of the Appendix Copyright © 2010 SciRes. JCT 175 Epidemiologic factors analyzed included patient age at diagnosis, gender, and date of surgery. Patients were categorized as to whether or not they received preop- erative imaging, the type of imaging performed, and whether the imaging was able to detect the presence of a neoplasm preoperatively, postoperatively on retro- spective review, or not at all. Laboratory values evalu- ated including preoperative white blood cell count and hemoglobin. Intraoperative values recorded including the presence of gross metastatic disease, whether a neo- plasm was suspected during the initial operation, whether a frozen section was performed. The operation performed as well as whether this was an initial opera- tion or a completion operation. Patient survival in months, follow up for a minimum of 2 years, and com- plications were also noted. Complications which were looked for included wound infections, abscess forma- tion, and development of pseudomyxoma peritonei. Outcomes were determined at surgery by pathologic examination and by clinical follow-up in all available patients. All patients were separated out by histologic classification and compared among those with similar neoplastic histology. 3. Results Of the 8560 cases of appendicitis, primary neoplasms of the appendix were diagnosed in 41 patients, an incidence of 0.5%. The incidence of diagnosis of primary tumors of the appendix increased from 0.3% between 1982-2003 to 1.2% between 2003-2008. An investigation of this dis- crepancy revealed that prior to 2001, cases of grossly metastatic adenocarcinoma of the appendix with colonic spre ad wer e cod ed as adeno carc inoma of th e co lon r athe r than adenocarcinoma of the appendix. It is believed the true incidence of primary tumors of the appendix is clos- er to 1.2% within the institution. Two patients were lost to follow up and records were not available. Twenty-six patients were female (63%) and 15 were male (37%). The average age at diagnosis was 53 years. Clinical presentation was variable (Table 1). As might be ex- pected, the majority of patients presented with signs and symptoms consistent with appendicitis. Forty-four per- cent presented with right lower quadrant abdominal pain and 7% presented with peritonitis while 22% of patients presented asymptomatically. Twenty percent of patients presented with other symptoms secondary to metastatic disease such as carcinoid syndrome (N = 1), bowel ob- struction (N = 3), dyspnea (N = 2), upper abdominal pain (N = 2), and vaginal bleeding (N = 1). The mortality rate in our series was 2%, with one death secondary to com- plications of distant metastatic disease in which the fam- ily opted to withdraw care. The average length of stay was 8 days. Table 1. Clinical presentation of primary tumors of the appendix. Symptoms Number of Patients % Pre-operative WBC(K/mcL) Right Lower Qua- drant Pain 18 44 10.1 Diffuse Peritonitis 3 7 23.6 Asymptomatic 9 22 10.9 Other 11 27 9.2 CARCINOID N=15 ADENO- CARCINOMA N=15 MUCINOUS CYSTADENO- CARCINOMA N=7 MIXED N=3 Figure 1. Distribution of primary tumors of the appendix. Adenocarcinoma (N = 16) and carcinoid (N = 15) we re the most common pathologic findings. Mucinous cysta- denoma (N = 7) and mixed adenocarcinoma and goblet cell carcinoid (N = 3) were also encountered as shown in Figure 1. Five percent (N = 2) of patients presented with a synchronous tumor elsewhere in the gastrointestinal tract. Diagnosis was made on colonoscopy when sigmoid ade- nocarcinomas were found in two patients with synchro- nous appendiceal adenocarcinomas. As shown in Table 2, appendiceal cancer was often discovered incidentally Table 2. Relationship of the diagnosis of primary appen- diceal tumor to the initial operation. Operative Findings Number of patients % Incidental finding during another procedure 18 44% Appendiceal cancer suspected prior to operation 10 24% Tumor discovered while operating for appendicitis 13 32% 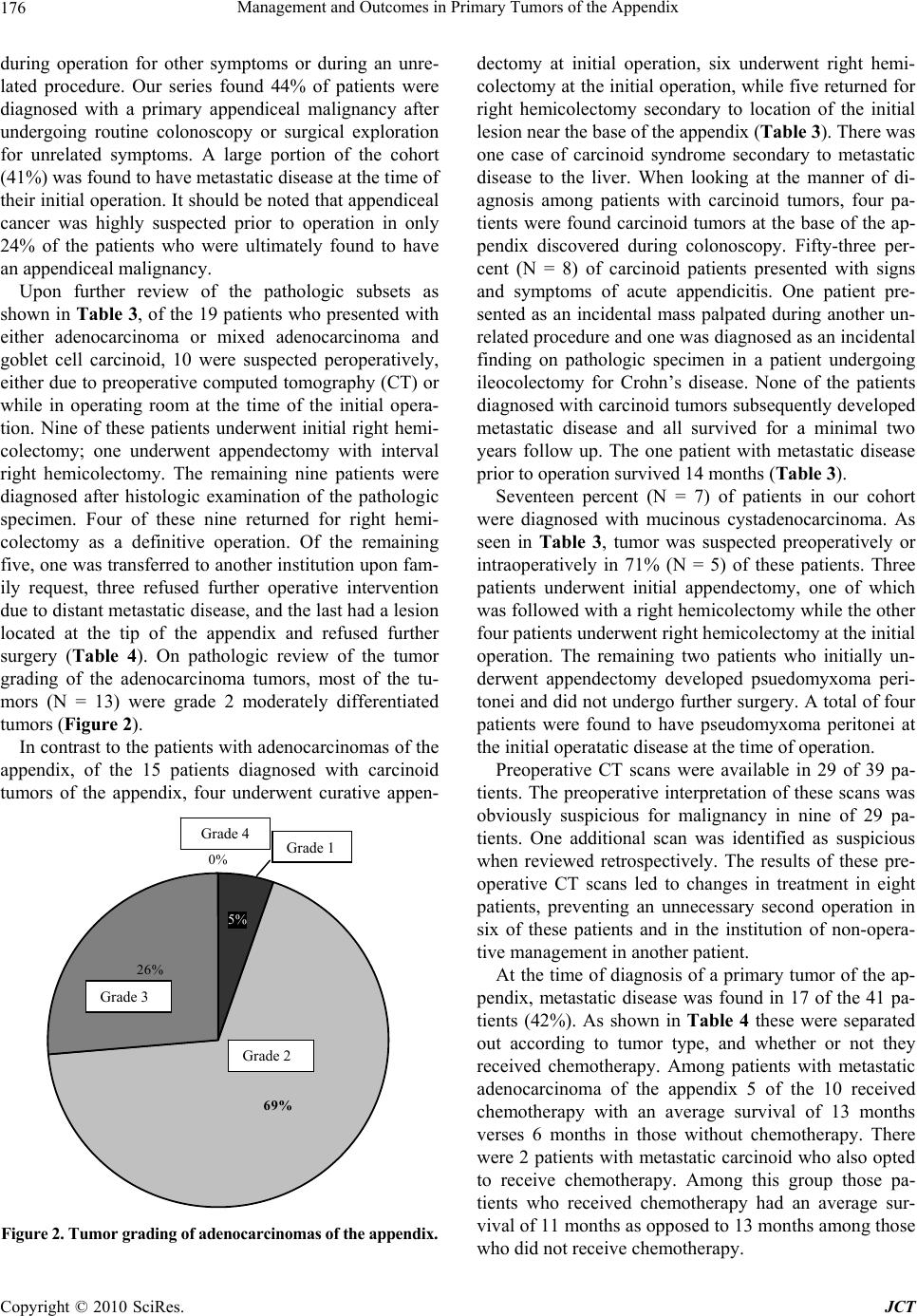 Management and Outcomes in Primary Tumors of the Appendix Copyright © 2010 SciRes. JCT 176 during operation for other symptoms or during an unre- lated procedure. Our series found 44% of patients were diagnosed with a primary appendiceal malignancy after undergoing routine colonoscopy or surgical exploration for unrelated symptoms. A large portion of the cohort (41%) was found to have metastatic disease at the time of their initial operation. It should be noted that appendiceal cancer was highly suspected prior to operation in only 24% of the patients who were ultimately found to have an appendiceal malignancy. Upon further review of the pathologic subsets as shown in Table 3, of the 19 patients who pr esented with either adenocarcinoma or mixed adenocarcinoma and goblet cell carcinoid, 10 were suspected peroperatively, either due to preoperative computed tomography (CT) or while in operating room at the time of the initial opera- tion. Nine of these patients underwent initial right hemi- colectomy; one underwent appendectomy with interval right hemicolectomy. The remaining nine patients were diagnosed after histologic examination of the pathologic specimen. Four of these nine returned for right hemi- colectomy as a definitive operation. Of the remaining five, one was transferred to another in stitution upon fam- ily request, three refused further operative intervention due to distant metastatic disease, and the last had a lesion located at the tip of the appendix and refused further surgery (Table 4). On pathologic review of the tumor grading of the adenocarcinoma tumors, most of the tu- mors (N = 13) were grade 2 moderately differentiated tumors (Figure 2). In contrast to the patients with adenocarcinomas of the appendix, of the 15 patients diagnosed with carcinoid tumors of the appendix, four underwent curative appen- 0% 5% 26% 69% Figure 2. Tumor grad ing of ad eno carcinomas of t he appendix . dectomy at initial operation, six underwent right hemi- colectomy at the initial o peration, while five returned for right hemicolectomy secondary to location of the initial lesion near the base of the appendix (Table 3). There was one case of carcinoid syndrome secondary to metastatic disease to the liver. When looking at the manner of di- agnosis among patients with carcinoid tumors, four pa- tients were found carcinoid tumors at the base of the ap- pendix discovered during colonoscopy. Fifty-three per- cent (N = 8) of carcinoid patients presented with signs and symptoms of acute appendicitis. One patient pre- sented as an incidental mass palpated during another un- related procedure and one was diagnosed as an incidental finding on pathologic specimen in a patient undergoing ileocolectomy for Crohn’s disease. None of the patients diagnosed with carcinoid tumors subsequently developed metastatic disease and all survived for a minimal two years follow up. The one patient with metastatic disease prior to operation survived 14 months (Table 3). Seventeen percent (N = 7) of patients in our cohort were diagnosed with mucinous cystadenocarcinoma. As seen in Table 3, tumor was suspected preoperatively or intraoperatively in 71% (N = 5) of these patients. Three patients underwent initial appendectomy, one of which was followed with a right hemicolecto my while the other four patients underwent right hemicolectomy at the initial operation. The remaining two patients who initially un- derwent appendectomy developed psuedomyxoma peri- tonei and did not undergo further surgery. A total of four patients were found to have pseudomyxoma peritonei at the initial operatatic disease at the time of operation. Preoperative CT scans were available in 29 of 39 pa- tients. The preoperative interpretation of these scans was obviously suspicious for malignancy in nine of 29 pa- tients. One additional scan was identified as suspicious when reviewed retrospectively. The results of these pre- operative CT scans led to changes in treatment in eight patients, preventing an unnecessary second operation in six of these patients and in the institution of non-opera- tive management in another patient. At the time of diagnosis of a primary tumor of the ap- pendix, metastatic disease was found in 17 of the 41 pa- tients (42%). As shown in Table 4 these were separated out according to tumor type, and whether or not they received chemotherapy. Among patients with metastatic adenocarcinoma of the appendix 5 of the 10 received chemotherapy with an average survival of 13 months verses 6 months in those without chemotherapy. There were 2 patients with metastatic carcinoid who also opted to receive chemotherapy. Among this group those pa- tients who received chemotherapy had an average sur- vival of 11 months as opposed to 13 months among those who did n ot receiv e ch e mothera py. Grade 2 Grade 3 Grade 4 Grade 1 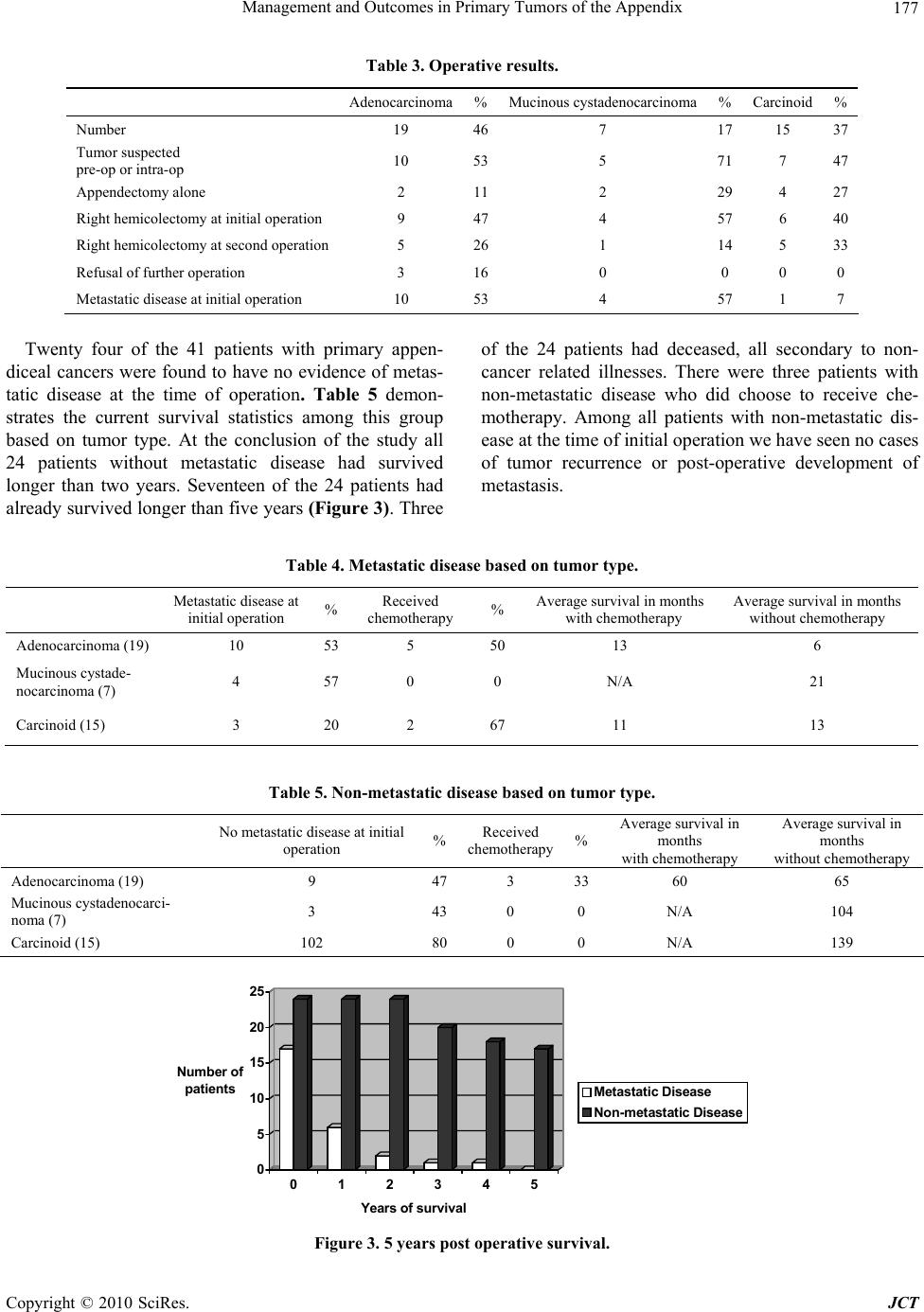 Management and Outcomes in Primary Tumors of the Appendix Copyright © 2010 SciRes. JCT 177 Table 3. Operative results. Adenocarcinoma%Mucinous cystadenocarcinoma % Carcinoid % Number 19 467 17 15 37 Tumor suspected pre-op or intra-op 10 535 71 7 47 Appendectomy alone 2 112 29 4 27 Right hemicolectomy at initial operation 9 474 57 6 40 Right hemicolectomy at second operation 5 261 14 5 33 Refusal of further operation 3 160 0 0 0 Metastatic disease at initial operation 10 534 57 1 7 Twenty four of the 41 patients with primary appen- diceal cancers were found to have no evidence of metas- tatic disease at the time of operation. Table 5 demon- strates the current survival statistics among this group based on tumor type. At the conclusion of the study all 24 patients without metastatic disease had survived longer than two years. Seventeen of the 24 patients had already survived longer than fi ve years (Figure 3). Thr ee of the 24 patients had deceased, all secondary to non- cancer related illnesses. There were three patients with non-metastatic disease who did choose to receive che- motherapy. Among all patients with non-metastatic dis- ease at the time of initial operation we have seen no cases of tumor recurrence or post-operative development of metastasis. Table 4. Metastatic disease based on tumor type . Metastatic disease at initial operation % Received chemotherapy % Average survival in months with chemotherapy Average survival in months without chemotherapy Adenocarcinoma (19) 10 53 5 50 13 6 Mucinous cystade- nocarcinoma (7) 4 57 0 0 N/A 21 Carcinoid (15) 3 20 2 67 11 13 Table 5. Non-metastatic disease based on tumor type. No metastatic disease at initial operation %Received chemotherapy %Average survival in months with chemotherapy Average survival in months without chemotherapy Adenocarcinoma (19) 9 473 3360 65 Mucinous cystadenocarci- noma (7) 3 430 0N/A 104 Carcinoid (15) 102 800 0N/A 139 0 5 10 15 20 25 Number of patients 012345 Years of survival Metastatic Disease Non-metastatic Di s e ase Figure 3. 5 years post operative survival.  Management and Outcomes in Primary Tumors of the Appendix Copyright © 2010 SciRes. JCT 178 4. Discussion Primary malignant tumors of the appendix are rare, oc- curring in 0.5% of all appendectomies [3]. The four main types of appendiceal malignancies are carcinoid tumors, mucinous cystadenocarcinomas, adenocarcinomas and adenocarcinoid tumors [4]. Common benign tumors in- clude villous adenomas and mucinous cystadenomas. Once encountered, the management of appendiceal tu- mors changes patient management from that of tradi- tional causes of appendicitis. As the study has shown, the majority of cases of appendiceal neoplasm are not diag- nosed pre-operatively, but rather intra-operatively, or on pathologic review of the specimen post-operatively. The diversity in treatment strategies for appendicitis creates the need for a well-defined treatment algorithm for ap- pendiceal malignancies that will ensure proper treatment in both the acute setting and retrospectively, when diag- nosis is made based on the pathologic specimen. First, gross inspection by the surgeon may reveal atypical findings. A frozen section should be done whenever the appendiceal findings are atypical. A diag- nosis of malignancy can be made during surgery and appropriate surgery can be done primarily [4]. Treatment then varies depending on tumor type and location. The treatment of each type of appendiceal neoplasm is well described in the literature. All patients with appendiceal neoplasms should be followed because a second malig- nancy will develop in 15% to 20% of cases [4]. Consistent with our findings, carcinoid tumors are the second most frequently encountered malignancy of the appendix after adenocarcinoma [5]. Appendiceal carci- noid tumors are typically found in 0.3-0.9 percent of pa- tients undergoing appendectomy [6]. They tend to pre- sent with the clinical signs and symptoms of an acute abdomen and frequently coexist with other intestinal neoplasms[5]. The size of the tumor is correlated with prognosis [7]. Diagnosis of a carcinoid tumor less than one centimeter, or according to some sources between one and two centimeters is appropriately treated with appen- dectomy alone [6]. The same tumor, measuring greater than two centimeters, or associated with mesen- teric/lymphatic invasion, should prompt right hemicolec- tomy [8]. Examination of the histological specimen re- vealing location at the base of the appendix, rather than at the tip also necessitates right hemi colectomy [6]. Review of the literature reveals that mucinous cystic neoplasms of the appendix continue to engender con- siderable debate in their diagnosis and management. Abdominal pain is the most common presenting symptom. The recommended treatment of mucinous cystadenocarcinoma is a right hemicolectomy with debulking of any pseudomyxoma peritonei [4]. In the reported literature, an approximately equal number of patients have been subjected to appendectomy alone versus right hemicolectomy [9]. Primary appendiceal adenocarcinoma is a rare neo- plasm that constitutes less than 0.5% of all gastrointesti- nal neoplasms, yet it is the most common appendiceal neoplasm. Most patients present with either local inva- sion or metastatic disease often involving the peritoneu m or ovaries [10]. In one study, a high frequency of ovarian metastases in women suggested a role for bilateral oo- phorectomy [11]. One important prognostic factor of primary appendiceal adenocarcinoma appears to be his- tology, with Park et al. [12] reporting improved survival in those patients with mucinous variants. Adenocarci- noma is best treated with right hemicolectomy regardless of size [4]. Survival rate has been shown to be superior after right hemicolectomy versus appendectomy alone [13]. In addition, right hemicolectomy performed as a secondary procedure resulted in the upstaging of 38% of the patients' tumors [13]. Adenocarcinoid tumors have a dual cell origin, sharing the histological features of both carcinoids and adenocar- cinomas, and a predilection for developing ovarian me- tastases. Size and location of the primary tumor is often cited as an indication for hemicolectomy rather than ap- pendectomy. However, other than size greater than two centimeters and base localization, current studies suggest that the presence of mucin producing cells, atypical foci, high mitotic count, or spread beyond the appendix is a further indication for secondar y r ight hemicolecto my [14, 15]. Adenocarcinoid tumor is appropriately treated by right hemicolectomy and ooph orectomy in females [4]. Although uncommon, primary appendiceal neo- plasms often result in clinical symptoms of appendicitis that may lead to radiographic analysis. As our study and other studies have shown, acute appendicitis is the most common manifestation for most tumor types. Other manifestations include intussusception, a palpa- ble mass, gastrointestinal bleeding, increasing ab- dominal girth (from pseudomyxoma peritoneii), and secondary genitourinary complications [16]. CT can help rule out or confirm an appendiceal tumor and may suggest a more specific diagnosis [16]. 5. Conclusions Operative strategy should be dictated by initial presenting characteristics of the tumor. Tumors should be first differen- tiated based on pathology. All adenocarcinomas, mixed adenocarcinoids, and mucinous cystadenocarcinomas should undergo right hemicolectomy regardless of size or locatio n on th e append ix. With regards to carcin oid tu mors, if discovered a t initial surger y as a mass larger than two cm, 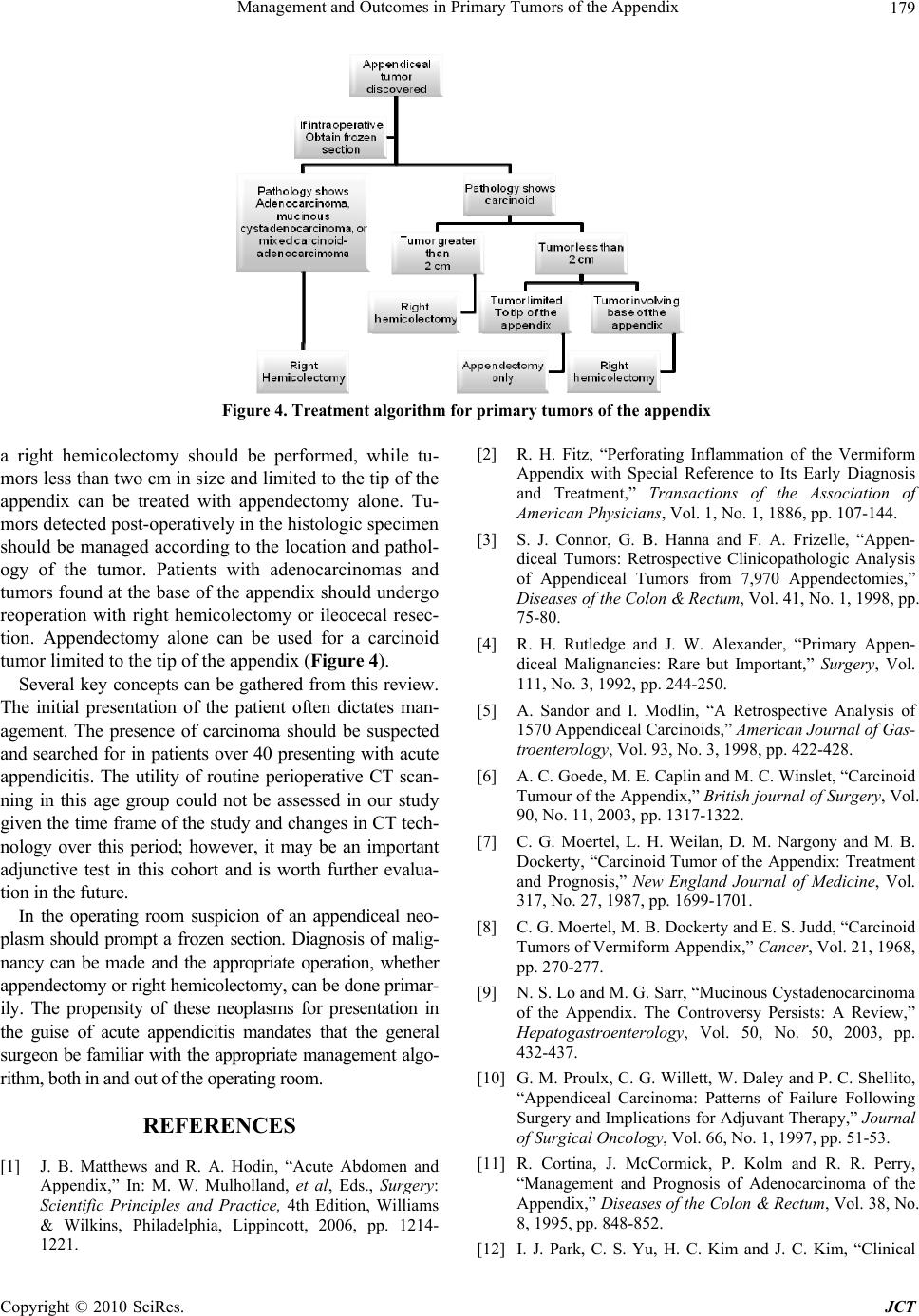 Management and Outcomes in Primary Tumors of the Appendix Copyright © 2010 SciRes. JCT 179 Figure 4. Treatment algorithm for primary tumors of the appendix a right hemicolectomy should be performed, while tu- mors less than two cm in size and limited to the tip of the appendix can be treated with appendectomy alone. Tu- mors detected post-operatively in the histologic specimen should be managed according to the location and pathol- ogy of the tumor. Patients with adenocarcinomas and tumors found at the base of the appendix should undergo reoperation with right hemicolectomy or ileocecal resec- tion. Appendectomy alone can be used for a carcinoid tumor limited to the tip of th e appendix (Figure 4). Several key concepts can be gathered from this review. The initial presentation of the patient often dictates man- agement. The presence of carcinoma should be suspected and searched for in patients over 40 presenting with acute appendicitis. The utility of routine perioperative CT scan- ning in this age group could not be assessed in our study given the time frame of the study and changes in CT tech- nology over this period; however, it may be an important adjunctive test in this cohort and is worth further evalua- tion in the future. In the operating room suspicion of an appendiceal neo- plasm should prompt a frozen section. Diagnosis of malig- nancy can be made and the appropriate operation, whether appendectomy or right hemicolectomy, can be done primar- ily. The propensity of these neoplasms for presentation in the guise of acute appendicitis mandates that the general surgeon be familiar with the appropriate management algo- rithm, both in and out of the operating room. REFERENCES [1] J. B. Matthews and R. A. Hodin, “Acute Abdomen and Appendix,” In: M. W. Mulholland, et al, Eds., Surgery: Scientific Principles and Practice, 4th Edition, Williams & Wilkins, Philadelphia, Lippincott, 2006, pp. 1214- 1221. [2] R. H. Fitz, “Perforating Inflammation of the Vermiform Appendix with Special Reference to Its Early Diagnosis and Treatment,” Transactions of the Association of American Physicians, Vol. 1, No. 1, 1886, pp. 107-144. [3] S. J. Connor, G. B. Hanna and F. A. Frizelle, “Appen- diceal Tumors: Retrospective Clinicopathologic Analysis of Appendiceal Tumors from 7,970 Appendectomies,” Diseases of the Colon & Rectum, Vol. 41, No. 1, 1998, pp. 75-80. [4] R. H. Rutledge and J. W. Alexander, “Primary Appen- diceal Malignancies: Rare but Important,” Surgery, Vol. 111, No. 3, 1992, pp. 244-250. [5] A. Sandor and I. Modlin, “A Retrospective Analysis of 1570 Appendiceal Carcinoids,” American Journal of Gas- troenterology, Vol. 93, No. 3, 1998, pp. 422-428. [6] A. C. Goede, M. E. Caplin and M. C. Winslet, “Carcinoid Tumour of the Appendix,” British journal of Surgery, Vol. 90, No. 11, 2003, pp. 1317-1322. [7] C. G. Moertel, L. H. Weilan, D. M. Nargony and M. B. Dockerty, “Carcinoid Tumor of the Appendix: Treatment and Prognosis,” New England Journal of Medicine, Vol. 317, No. 27, 1987, pp. 1699-1701. [8] C. G. Moertel, M. B. Dockerty and E. S. Judd, “Carcinoid Tumors of Vermiform Appendix,” Cancer, Vol. 21, 1968, pp. 270-277. [9] N. S. Lo and M. G. Sarr, “Mucinous Cystadenocarcinoma of the Appendix. The Controversy Persists: A Review,” Hepatogastroenterology, Vol. 50, No. 50, 2003, pp. 432-437. [10] G. M. Proulx, C. G. Willett, W. Daley and P. C. Shellito, “Appendiceal Carcinoma: Patterns of Failure Following Surgery and Implications for Adjuvant Therapy,” Journal of Surgical Oncology, Vol. 66, No. 1, 1997, pp. 51-53. [11] R. Cortina, J. McCormick, P. Kolm and R. R. Perry, “Management and Prognosis of Adenocarcinoma of the Appendix,” Diseases of the Colon & Rectum, Vol. 38, No. 8, 1995, pp. 848-852. [12] I. J. Park, C. S. Yu, H. C. Kim and J. C. Kim, “Clinical  Management and Outcomes in Primary Tumors of the Appendix Copyright © 2010 SciRes. JCT 180 Features and Prognostic Factors in Primary Adenocarci- noma of the Appendix,” Korean Journal of Gastroen- terology, Vol. 43, No. 1, 2004, pp. 29-34. [13] S. S. Nitecki, B. G. Wolff, R. Schlinkert and M. G. Sarr, “The Natural History of Surgically Treated Primary Adenocarcinoma of the Appendix,” Annals of Surgery, Vol. 219, No. 1, 1994, pp. 51-57. [14] R. L. Warkel, P. H. Cooper and E. B. Helwig, “Adeno- carcinoid, a Mucin-producing Carcinoid Tumor of the Appendix: a Study of 39 Cases,” Cancer, Vol. 42, No. 6, 1978, pp. 2781-2793. [15] J. L. Gouzi, P. Laigneau, J. P. Delalande, et al., “Indica- tions for Right Hemicolectomy in Carcinoid Tumors of the Appendix,” Surgery, Gynecology & Obstetrics, Vol. 176, No. 6, 1993, pp. 543-547. [16] P. J. Pickhardt, A. D. Le vy, C. A. Rohrmann Jr. and A. I. Kende, “Primary Neoplasms of the Appendix: Radiologic Spectrum of Disease with Pathologic Correlation,” Ra- diographics, Vol. 23, No. 3, 2003, pp. 645-662. |