M. A. S. ALI
Copyright © 2013 SciRes. ENG
66
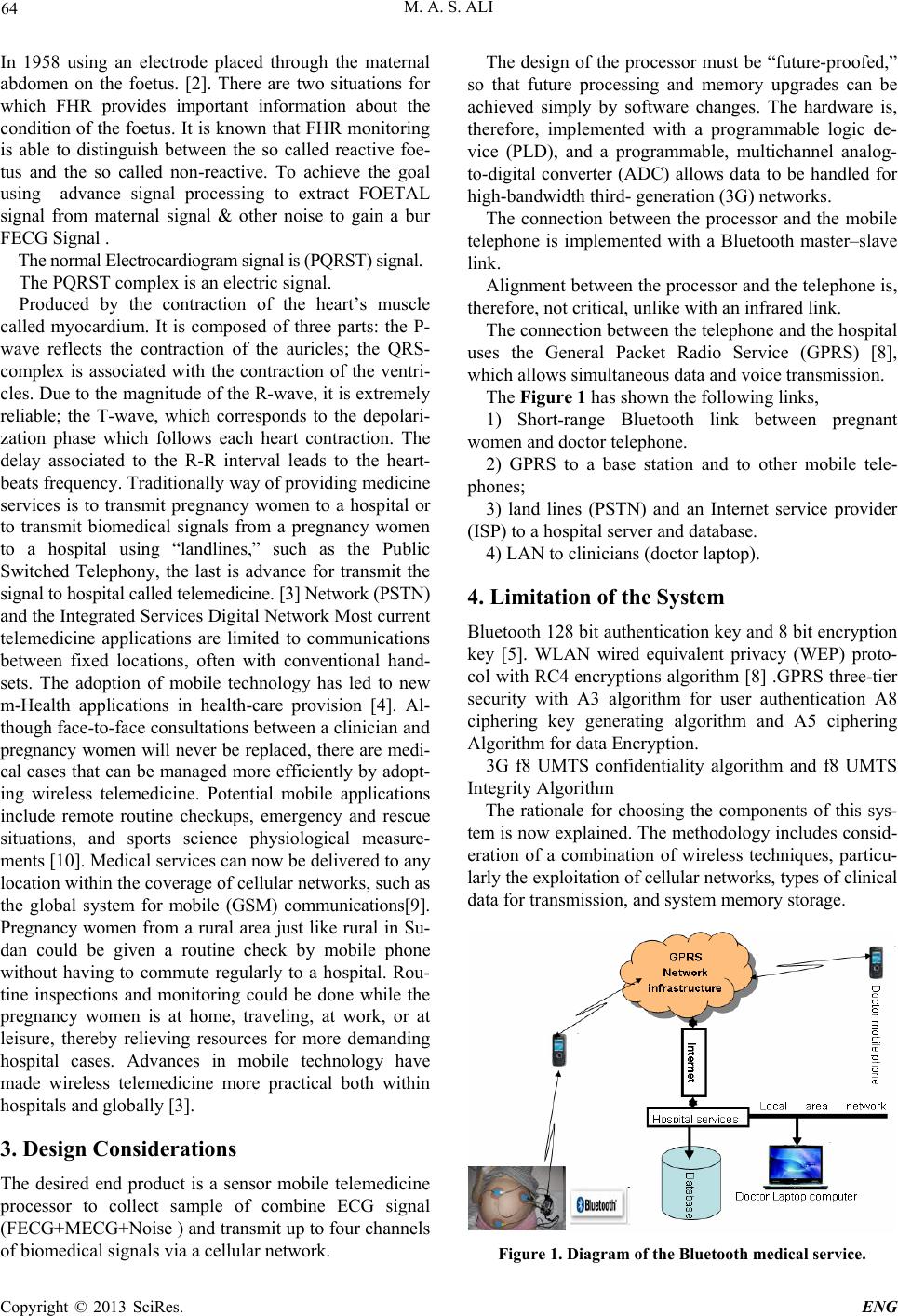
Figure 3. Shows the abdominal records and pure foetal sig-
nals.
Already the records of the maternal Thoracic Electro-
cardiogram (TECG) signals are known and the record s of
the Abdominal Electrocardiogram (AECG) which contains
foetal ECG + maternal ECG represent the complex part.
6. Results
The maternal ECG signal interference was canceled from
the foetal heart ECG signal .ECG signals are given as an
input and is simulated using MATLAB. The results of
programs are shown in the Figure 3. These results rep-
resent the raw data of PQRST and U complex signal re-
corded from maternal abdominal and pure PQRST com-
plex signal for Fetus after extraction , this results should
be appeared at doctor laptop computer or mobile phone
7. Discussion
Figure 3 in results above contains two graphs. The upper
graph shows AECG and FECG recombined after being
extracted. In comparing these two signals we can see the
region of FECG in AECG signal. The lower graph shows
pure FECG. The amplitude of QRS of FECG is about 30
microvolt while that of MECG is about 150 microvolt.
These values may agree to the value of QRS amplitude.
The obtained result shows the effectiveness of the pro-
posed algorithm.
8. Conclusions
It can be assumed from this study that the goal of Sensor
mobile telemedicine is to record real accurate electrocar-
diogram data and encapsulate then transmit to the target
safety without any interference. It is important to under-
stand the actual though process over several wireless
systems of individual technique which have different
attachment styles. It is easy to transfer this idea to sense
and monitoring one of very important issue that is foetal
electrocardiogram (FECG), but the weakness of FECG
signal need more security technique to avoid interference
of the noises.
The algorithm used in this study is v ery simple an d not
complex. The performance and validity of the proposed
algorithm have been confirmed by computer simulations
and experiment on real-world ECG data. The data used
here is public databases widely used by the signal proc-
ssing community known as SISTA/DAISY dataset. The
result which was obtained appears to agree with the
standard Foetal ECG signals. The Researcher recom-
mends following this method to gain more useful results.
9. Acknowledgements
This work was supported in part by university of Nyala
Republic of the Sudan. Many thanks to the University of
Nyala for offering me the fund for this conference.
REFERENCES
[1] R. Sameni, “Extraction of Foetal Cardiac Signals from an
Array of Maternal Abdominal Recordings,” Sharif Uni-
versity of Technology, Tehran, Iran,Doctor of Philoso-
phy thesis , July 2008
[2] A. M. J. Lenssen. “From Cardiac Electrical Activity to
the ECG: A finite Element Model,” Master thesis, Eind-
hoven University of Technology, May 2008.
[3] N. M. Fisk, S. Bower and W. Sepulveda, “Foetal Tele-
medicine: Interactive Transfer of Real Time Ultrasound
and Video Via ISDN for Remote Consultation,” Journal
of Telemedicine and Telecare, Vol. 1, No. 1, 1995, pp.
38-44.
[4] M. F. A. Rasid and B. Woodward, “Bluetooth Telemedi-
cine Processor for Multichannel Biomedical Signal
Transmission Via Mobile Cellular Networks,” IEEE, Vol.
9, No. 1, March 2005.
[5] Noureddine BELGACEM, Fethi BEREKSI-REGUIG, “A
Design of DSPIC Based ECG Signal Monitoring and
Processing System,” BP 230 Tlemcen, 2003
[6] O. Krejcar, D. Janckulik, L. Motalova and K. Musil,
“Real Time Processing of ECG Signal on Mobile Em-
bedded Monitoring Stations,” Second International Con-
ference on Computer Engineering and Applications,
2010.
[7] S. Da˘ gtas, G. Pekhteryev, Z. Sahino ˘ glu, H. C am and
N. Challa, “Real-Time and Secure Wireless Health Moni-
toring,” Hindawi Publishing Corporation International
Journal of Telemedicine and Applications, Article ID,
2008, 135808.
[8] J. P. Tello, O. Manjarres, M. Quijano, A. Blanco, F. Va-
rona and M. Manrique,’’ Remote Monitoring System of
ECG and Body Temperature Signals,” IEEE LATIN
AMERICA Transactions, Vol. 11, No. 1, Feb 2013.
[9] Zuckerwar, R. Pretlow, J. Stoughton and D. Baker, “De-
velopment of a Piezopolymer Pressure Sensor for a Port-
able Foetal Heart Rate Monitor,” IEEE Trans. Biomed.
Eng., Vol. 40, No. 9, 1993, pp. 963-969.
doi:10.1109/10.245618
[10] M. Scanziani and M. Häusser, “Electrophysiology in the
Age of Light,” Nature, 2009, Vol. 461, 15 Octo-
ber.doi:10.1038/nature08540
[11] E. M. Symonds, “Foetal Electrocardiographic Monitoring:
Past, Present and Future--a Historical Perspective,” J
Perinat Med., Vol. 14, No. 6, 1986, pp. 385-90.
e