Granular Cell Tumor of the Esophagus: A Patient Treated by Endoscopic Mucosal
Resection with Long Term Follow-Up
356
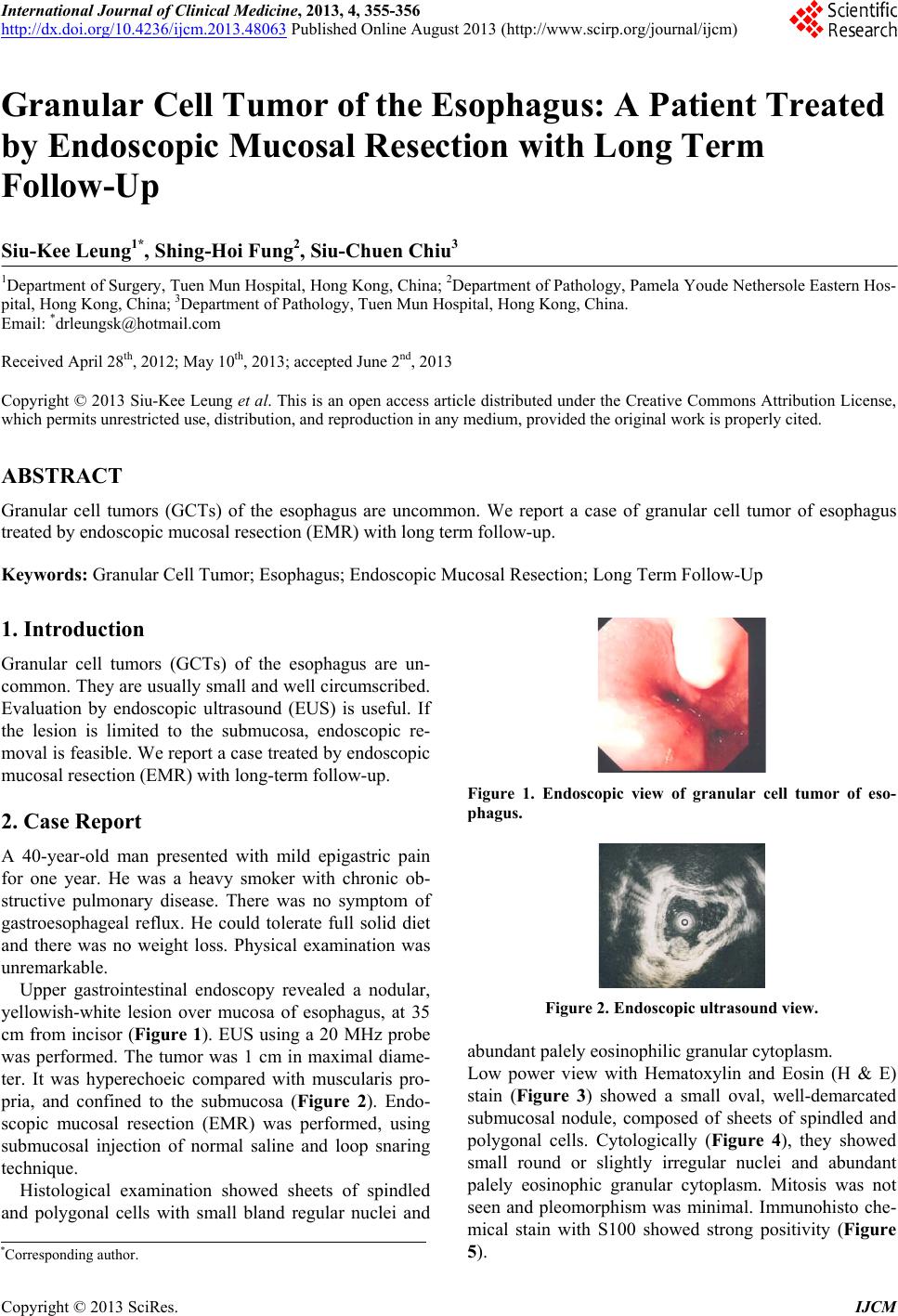
Figure 3. Low power, Hematoxylin and Eosin stain (H & E
stain).
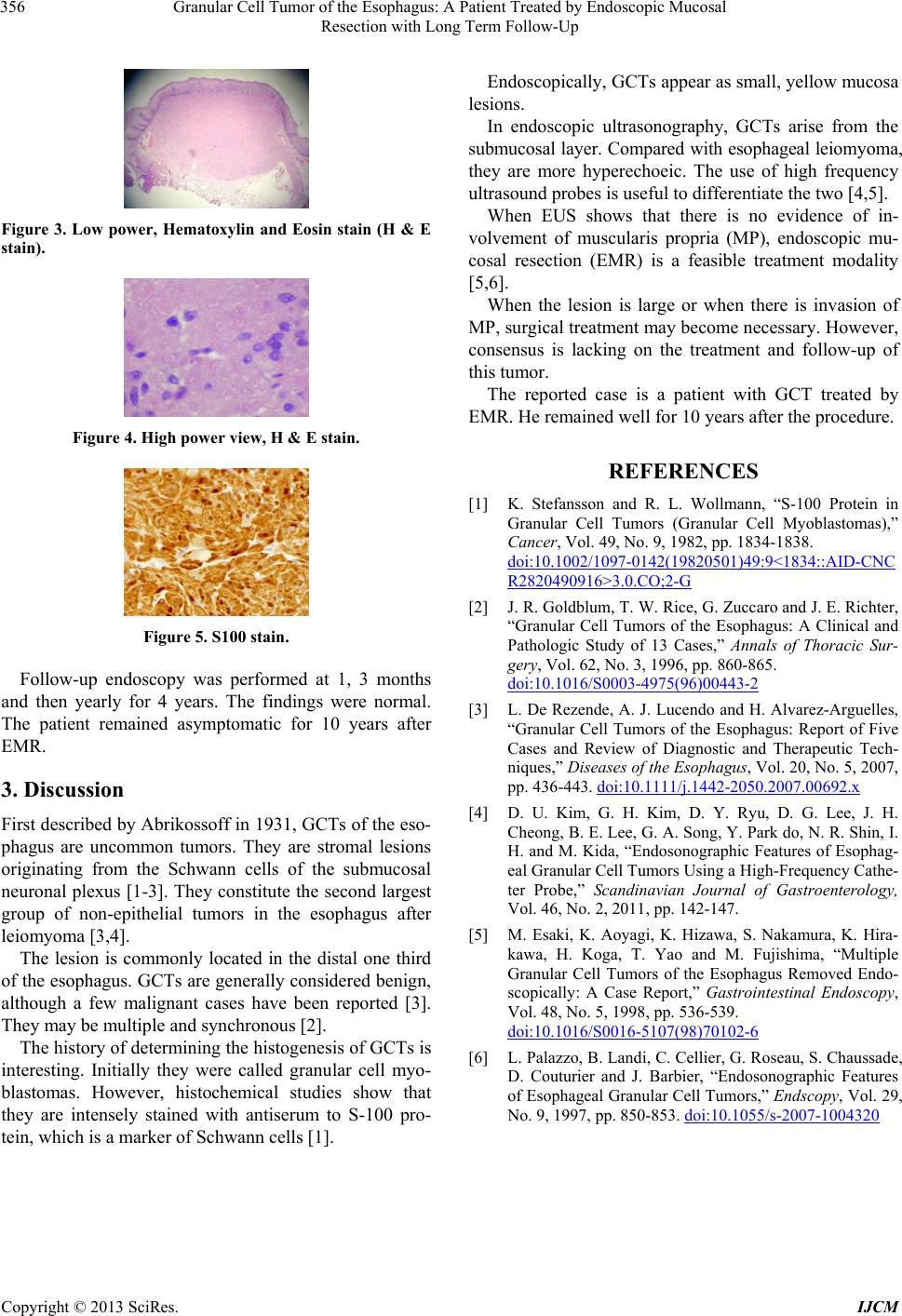
Figure 4. High power view, H & E stain.
Figure 5. S100 stain.
Follow-up endoscopy was performed at 1, 3 months
and then yearly for 4 years. The findings were normal.
The patient remained asymptomatic for 10 years after
EMR.
3. Discussion
First described by Abriko ssoff in 1931, GCTs of the eso-
phagus are uncommon tumors. They are stromal lesions
originating from the Schwann cells of the submucosal
neuronal plexus [1-3]. They constitute the second largest
group of non-epithelial tumors in the esophagus after
leiomyoma [3,4].
The lesion is commonly located in the distal one third
of the esophagus. GCTs are generally considered benign,
although a few malignant cases have been reported [3].
They may be multiple and synchronous [2].
The history of determining the histogenesis of GCTs is
interesting. Initially they were called granular cell myo-
blastomas. However, histochemical studies show that
they are intensely stained with antiserum to S-100 pro-
tein, which is a marker of Schwann cells [1].
Endoscopically, GCTs appear as small, yellow mucosa
lesions.
In endoscopic ultrasonography, GCTs arise from the
submucosal layer. Compared with esophageal leiomyoma,
they are more hyperechoeic. The use of high frequency
ultrasound probes is usef ul to differentiate the two [4,5].
When EUS shows that there is no evidence of in-
volvement of muscularis propria (MP), endoscopic mu-
cosal resection (EMR) is a feasible treatment modality
[5,6].
When the lesion is large or when there is invasion of
MP, surgical treatment may become necessary. However,
consensus is lacking on the treatment and follow-up of
this tumor.
The reported case is a patient with GCT treated by
EMR. He remained well for 10 years after the procedure.
REFERENCES
[1] K. Stefansson and R. L. Wollmann, “S-100 Protein in
Granular Cell Tumors (Granular Cell Myoblastomas),”
Cancer, Vol. 49, No. 9, 1982, pp. 1834-1838.
doi:10.1002/1097-0142(19820501)49:9<1834::AID-CNC
R2820490916>3.0.CO;2-G
[2] J. R. Goldblum, T. W. Rice, G. Zuccaro and J. E. Richter,
“Granular Cell Tumors of the Esophagus: A Clinical and
Pathologic Study of 13 Cases,” Annals of Thoracic Sur-
gery, Vol. 62, No. 3, 1996, pp. 860-865.
doi:10.1016/S0003-4975(96)00443-2
[3] L. De Rezende, A. J. Lucendo and H. Alvarez-Arguelles,
“Granular Cell Tumors of the Esophagus: Report of Five
Cases and Review of Diagnostic and Therapeutic Tech-
niques,” Diseases of the Esophagus, Vol. 20, No. 5, 2007,
pp. 436-443. doi:10.1111/j.1442-2050.2007.00692.x
[4] D. U. Kim, G. H. Kim, D. Y. Ryu, D. G. Lee, J. H.
Cheong, B. E. Lee, G. A. Song, Y. Park do, N. R. Shin, I.
H. and M. Kida, “Endosonographic Features of Esophag-
eal Granular Cell Tumors Using a High-Frequency Cathe-
ter Probe,” Scandinavian Journal of Gastroenterology,
Vol. 46, No. 2, 2011, pp. 142-147.
[5] M. Esaki, K. Aoyagi, K. Hizawa, S. Nakamura, K. Hira-
kawa, H. Koga, T. Yao and M. Fujishima, “Multiple
Granular Cell Tumors of the Esophagus Removed Endo-
scopically: A Case Report,” Gastrointestinal Endoscopy,
Vol. 48, No. 5, 1998, pp. 536-539.
doi:10.1016/S0016-5107(98)70102-6
[6] L. Palazzo, B. Landi, C. Cellier, G. Roseau, S. Chaussade,
D. Couturier and J. Barbier, “Endosonographic Features
of Esophageal Granular Cell Tumors,” Endscopy, Vol. 29,
No. 9, 1997, pp. 850-853. doi:10.1055/s-2007-1004320
Copyright © 2013 SciRes. IJCM