B. O. AKINBAMI, O. A. AKADIRI 343
morphogenenic proteins, hydroxyappatite blocks and
Beta TriCalcium phosphates, medpors (polyethelene)
with or without hyaluronic acid are now available as al-
loplasts to minimize donor site mobilities [30]. The
above treatment is also useful for old, malunited and non
united fractures. After refracturing, debriding and fresh-
ening the bony ends, it is necessary to fill gap with can-
cellous chips and apply reconstruction plates. Condyle
implants like the Lorenz or Christensens type are avail-
able for total joint replacements [29,30].
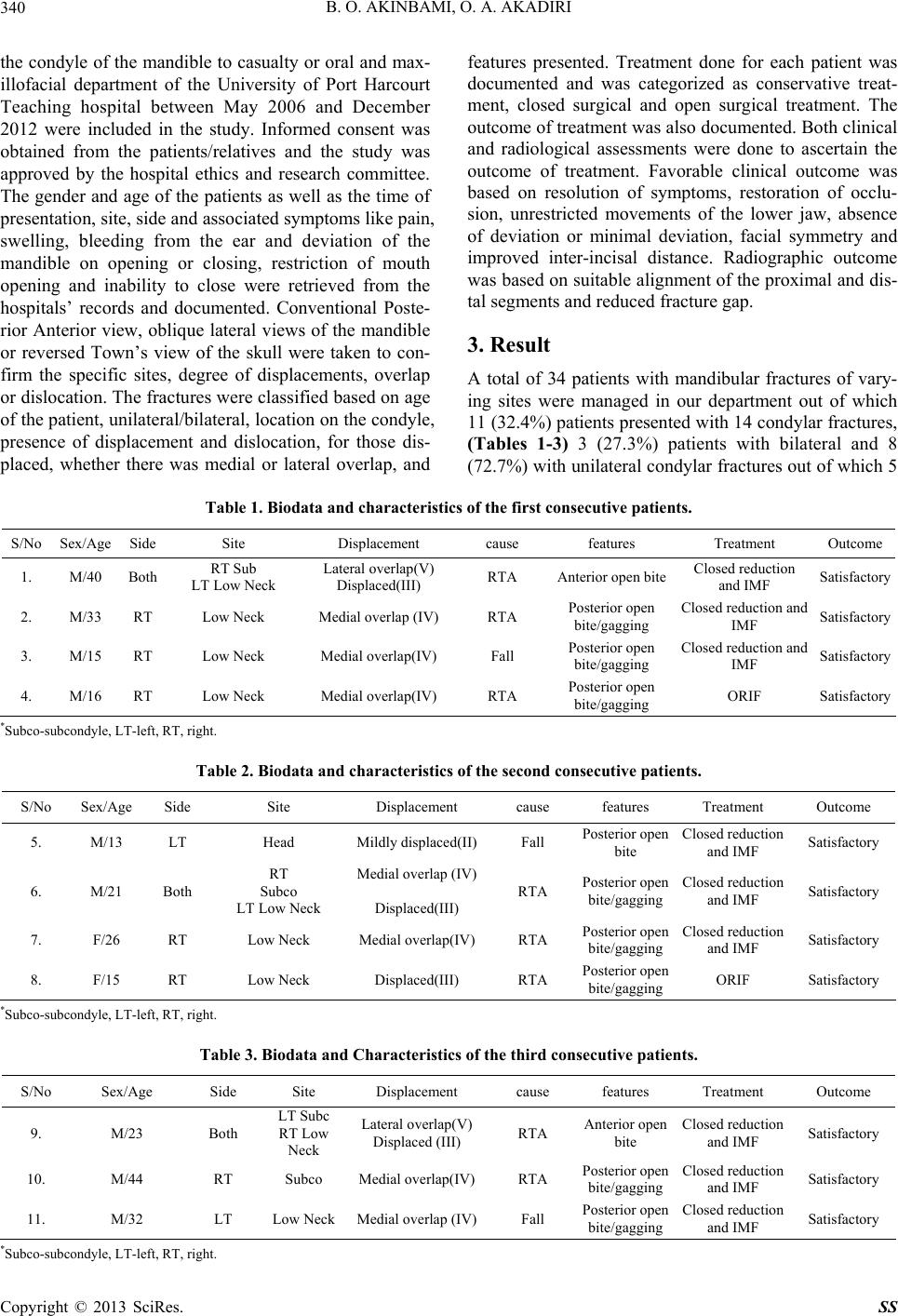
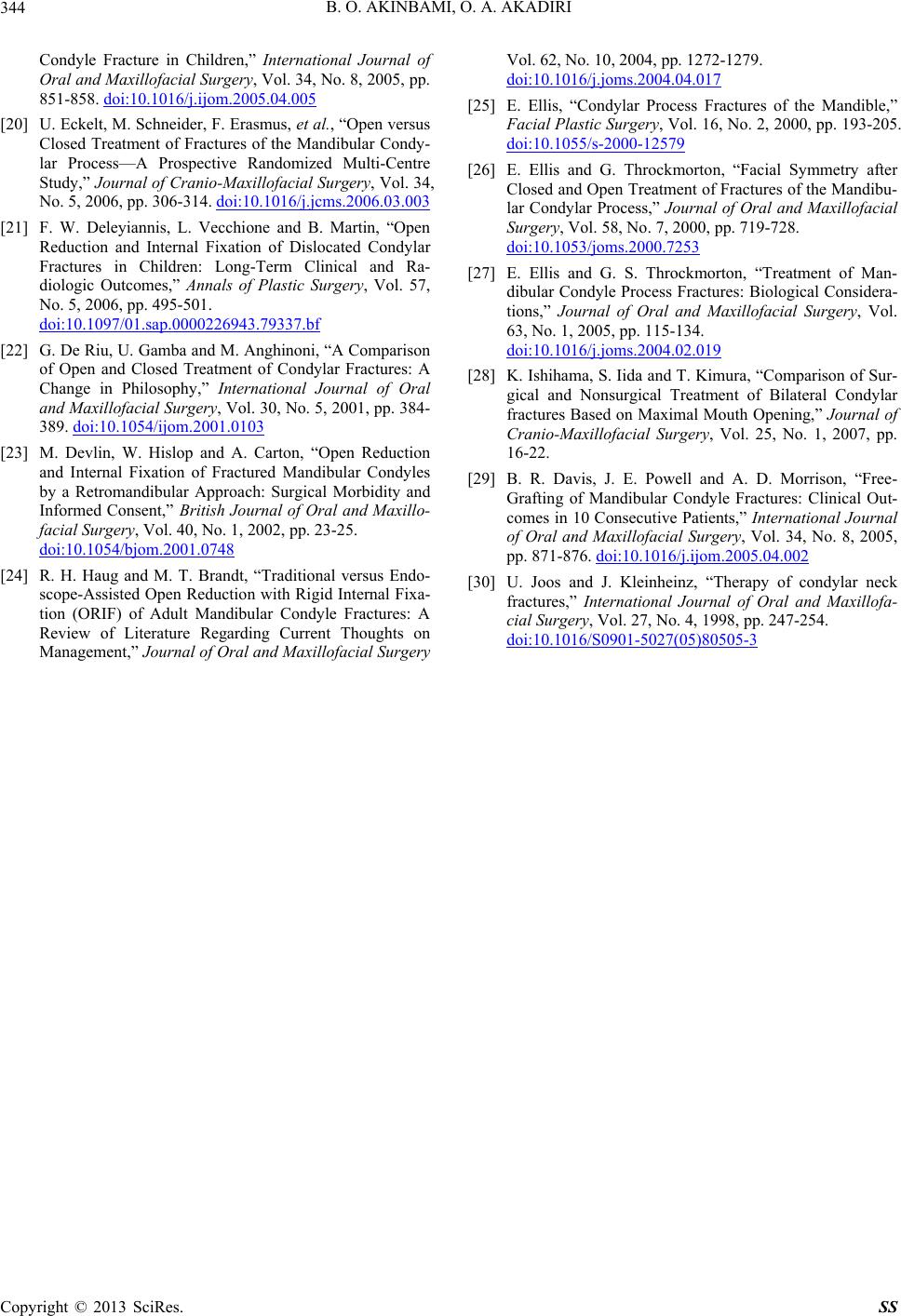
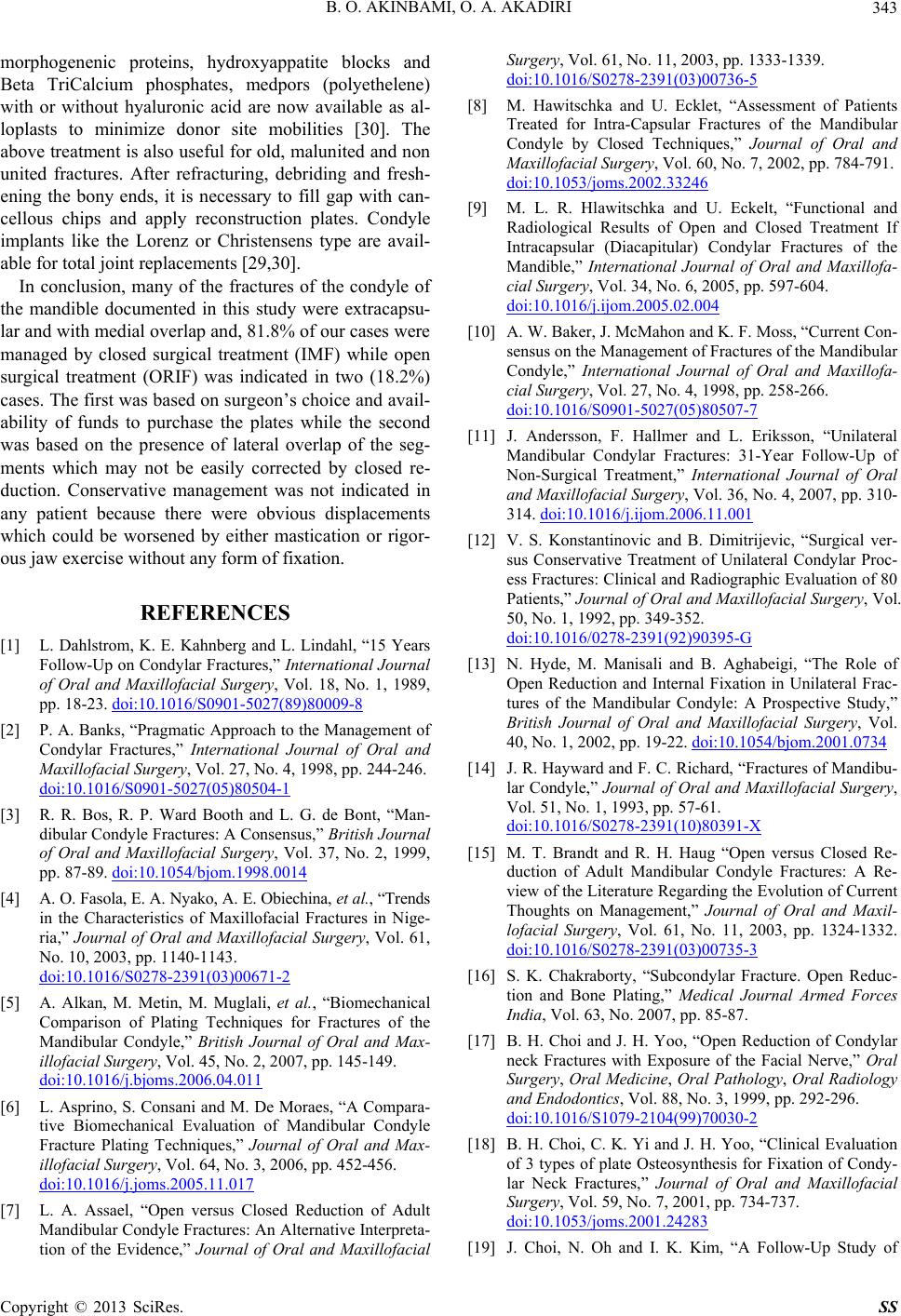
In conclusion, many of the fractures of the condyle of
the mandible documented in this study were extracapsu-
lar and with medial ov erlap and, 81.8 % of our cases were
managed by closed surgical treatment (IMF) while open
surgical treatment (ORIF) was indicated in two (18.2%)
cases. The first was based on surgeon’s choice and avail-
ability of funds to purchase the plates while the second
was based on the presence of lateral overlap of the seg-
ments which may not be easily corrected by closed re-
duction. Conservative management was not indicated in
any patient because there were obvious displacements
which could be worsened by either mastication or rigor-
ous jaw exercise without any form of fixation.
REFERENCES
[1] L. Dahlstrom, K. E. Kahnberg and L. Lindahl, “15 Years
Follow-Up on Condylar Fractures,” International Journal
of Oral and Maxillofacial Surgery, Vol. 18, No. 1, 1989,
pp. 18-23. doi:10.1016/S0901-5027(89)80009-8
[2] P. A. Banks, “Pragmatic Approach to the Management of
Condylar Fractures,” International Journal of Oral and
Maxillofacial Surgery, Vol. 27, No. 4, 1998, pp. 244-246.
doi:10.1016/S0901-5027(05)80504-1
[3] R. R. Bos, R. P. Ward Booth and L. G. de Bont, “Man-
dibular Condyle Fractures: A Consensus,” British Journal
of Oral and Maxillofacial Surgery, Vol. 37, No. 2, 1999,
pp. 87-89. doi:10.1054/bjom.1998.0014
[4] A. O. Fasola, E. A. Nyako, A. E. Obiechina, et al., “Trends
in the Characteristics of Maxillofacial Fractures in Nige-
ria,” Journal of Oral and Maxillofacial Surgery, Vol. 61,
No. 10, 2003, pp. 1140-1143.
doi:10.1016/S0278-2391(03)00671-2
[5] A. Alkan, M. Metin, M. Muglali, et al., “Biomechanical
Comparison of Plating Techniques for Fractures of the
Mandibular Condyle,” British Journal of Oral and Max-
illofacial Surgery, Vol. 45, No. 2, 2007, pp. 145-149.
doi:10.1016/j.bjoms.2006.04.011
[6] L. Asprino, S. Consani and M. De Moraes, “A Compara-
tive Biomechanical Evaluation of Mandibular Condyle
Fracture Plating Techniques,” Journal of Oral and Max-
illofacial Surgery, Vol. 64, No. 3, 2006, pp. 452-456.
doi:10.1016/j.joms.2005.11.017
[7] L. A. Assael, “Open versus Closed Reduction of Adult
Mandibular Condyle Fractures: An Alternative Interpreta-
tion of the Evidence,” Journal of Oral and Maxillofacial
Surgery, Vol. 61, No. 11, 2003, pp. 1333-1339.
doi:10.1016/S0278-2391(03)00736-5
[8] M. Hawitschka and U. Ecklet, “Assessment of Patients
Treated for Intra-Capsular Fractures of the Mandibular
Condyle by Closed Techniques,” Journal of Oral and
Maxillofacial Surgery, Vol. 60, No. 7, 2002, pp. 784-791.
doi:10.1053/joms.2002.33246
[9] M. L. R. Hlawitschka and U. Eckelt, “Functional and
Radiological Results of Open and Closed Treatment If
Intracapsular (Diacapitular) Condylar Fractures of the
Mandible,” International Journal of Oral and Maxillofa-
cial Surgery, Vol. 34, No. 6, 2005, pp. 597-604.
doi:10.1016/j.ijom.2005.02.004
[10] A. W. Baker, J. McMahon and K. F. Moss, “Current Con-
sensus on the Management of Fractures of the Mandibular
Condyle,” International Journal of Oral and Maxillofa-
cial Surgery, Vol. 27, No. 4, 1998, pp. 258-266.
doi:10.1016/S0901-5027(05)80507-7
[11] J. Andersson, F. Hallmer and L. Eriksson, “Unilateral
Mandibular Condylar Fractures: 31-Year Follow-Up of
Non-Surgical Treatment,” International Journal of Oral
and Maxillofacial Surgery, Vol. 36, No. 4, 2007, pp. 310-
314. doi:10.1016/j.ijom.2006.11.001
[12] V. S. Konstantinovic and B. Dimitrijevic, “Surgical ver-
sus Conservative Treatment of Unilateral Condylar Proc-
ess Fractures: Clinical and Radiographic Evaluation of 80
Patients,” Journal of Oral and Maxillofacial Surgery, Vol.
50, No. 1, 1992, pp. 349-352.
doi:10.1016/0278-2391(92)90395-G
[13] N. Hyde, M. Manisali and B. Aghabeigi, “The Role of
Open Reduction and Internal Fixation in Unilateral Frac-
tures of the Mandibular Condyle: A Prospective Study,”
British Journal of Oral and Maxillofacial Surgery, Vol.
40, No. 1, 2002, pp. 19-22. doi:10.1054/bjom.2001.0734
[14] J. R. Hayward and F. C. Richard, “Fractures of Mandibu-
lar Condyle,” Journal of Oral and Maxillofacial Surgery,
Vol. 51, No. 1, 1993, pp. 57-61.
doi:10.1016/S0278-2391(10)80391-X
[15] M. T. Brandt and R. H. Haug “Open versus Closed Re-
duction of Adult Mandibular Condyle Fractures: A Re-
view of the Literature Regarding the Evolution of Current
Thoughts on Management,” Journal of Oral and Maxil-
lofacial Surgery, Vol. 61, No. 11, 2003, pp. 1324-1332.
doi:10.1016/S0278-2391(03)00735-3
[16] S. K. Chakraborty, “Subcondylar Fracture. Open Reduc-
tion and Bone Plating,” Medical Journal Armed Forces
India, Vol. 63, No. 2007, pp. 85-87.
[17] B. H. Choi and J. H. Yoo, “Open Reduction of Condylar
neck Fractures with Exposure of the Facial Nerve,” Oral
Surgery, Oral Medicine, Oral Pathology, Oral Radiology
and Endodontics, Vol. 88, No. 3, 1999, pp. 292-296.
doi:10.1016/S1079-2104(99)70030-2
[18] B. H. Choi, C. K. Yi and J. H. Yoo, “Clinical Evaluation
of 3 types of plate Osteosynthesis for Fixation of Condy-
lar Neck Fractures,” Journal of Oral and Maxillofacial
Surgery, Vol. 59, No. 7, 2001, pp. 734-737.
doi:10.1053/joms.2001.24283
[19] J. Choi, N. Oh and I. K. Kim, “A Follow-Up Study of
Copyright © 2013 SciRes. SS