F. D. DELLAL ET AL. 237
Vitamins are the essential elements which are necessary
for occurrence of metabolic events and maintenance of
health status, while they cannot be synthesized in the body
or synthesized inadequately, and need to be intaken.
Non-enzymatic anti-oxidants, like vitamin E and A,
contribute to decrease the oxidative damage caused by
oxygen radicals by taking their high-energy electrons [4].
Another function of vitamin E is to increase the absorp-
tion of vitamin A from the intestines and its level in the
tissues. Concomitance of hypothyroidism and pernicious
anemia is very frequent, and vitamin B12 deficiency is
observed in pernicious anemia. Due to its antiinflam-
matory and immunomodulatory features and potential
effects on cytokine levels, decreased levels of vitamin D
is associated with the increased risks of many disorders,
particularly autoimmune diseases [5,6]. Folic acid, which
is actually a pro-vitamin, is changed to dihydrofolat by
dehydrofolat reductase enzyme after being absorbed, and
then it is converted to tetrahydrofolate. Using single car-
bon units, the nascent tetrahydrofolate transfers single
carbon to some endogenous substances via various oxi-
dating mechanisms.
In this study, we aimed to determine the levels of serum
trace elements like selenium, zinc, copper and iron, and
vitamins like A, E, B12, 25-OH-D, 1,25(OH)2D, folic acid
in patients with HT and evaluate the association between
thyroid antibodies and these elements and vitamins.
2. Material and Methods
This prospective study included 51 premenopausal wo-
men aged between 18 to 56 years and 27 healthy pre-
menopausal women aged between 19 to 42 years, who
had applied to our clinic. Only female participants are
involved in order to create a homogeneous group. Pa-
tients were newly diagnosed and untreated with L-thy-
roxine. Patients with any known diseases (diabetes mel-
litus, hypertension, hyperlipidemia, coronary artery dis-
ease, chronic liver or kidney diseases, gastrointestinal
absorption problems, collagen tissue disease, bone me-
tabolism disease, thyroid disease or malignancy) or chro-
nic medicine users were excluded. Demographic charac-
teristics, information on current smoking and alcohol
consumption and personal and familial histories were re-
corded, and detailed physical examinations were per-
formed. Informed consent forms were obtained from all
patients. Approval of Local Ethics Committee was taken.
The study was performed in accordance with Helsinki
Declaration and Good Clinical Practice.
HT was diagnosed by elevated anti thyroid peroxidase
(anti-TPO), anti thyroglobulin (anti-TG) levels and thy-
roid ultrasonography evaluation which revealed hetero-
geneity and fibrotic bands in thyroid glands [7]. Subjects
with normal thyroid antibodies were considered to be
healthy.
Weight, waist circumference, hip circumference and
height were measured in fasting status and with daily
clothes by the same person. The waist circumference was
accepted as the narrowest diameter between the arcus
costarum and spina iliaca anterior superior, and the hip
circumference was considered as the largest diameter over
the gluteus maximus posteriorly and symphysis pubis
anteriorly. Body mass index (BMI) was the ratio of the
weight to the square of height (weight/heigh2- kg/m2).
Blood samples were collected following 12 hours of
fasting. In order to study selenium levels (N: 46 - 143
µg/L), the collected blood samples were centrifuged at
5000 rpm/min after coagulation and stored at −80˚C until
testing. The test was performed manually by AAS Hydro
System Management. Blood samples were collected from
antecubital veins to evaluate iron, copper, zinc, albumin,
thyroid stimulating hormone (TSH), Anti-TG, Anti-TPO,
TSH receptor antibody (TRAB), vitamin A, vitamin E,
vitamin B12, 25-OH vitamin D, 1.25-(OH)2 vitamin D
and folic acid. Iron (N: 70 - 180 µg/dL), copper (N: 12.6 -
24 µmol/L) and zinc (N: 10.4 - 22.9 µmol/L) were de-
tected by Olympus AU 2700 equipment using the original
kits. 25-OH vitamin D (N: 10 - 80 ng/mL), 1.25-(OH)2
vitamin D (N: 10 - 60 pg/mL) and TRAB (N: 0 - 14 U/L)
levels were detected by radioimmunaassay (RIA) method
using Dia Source kit. fT3 (N: 2.3 - 4.2 pg/mL), sT4 (N:
0.7 - 1.76 ng/dL), TSH (N: µIU/mL), anti-TPO (N: 0 - 60
U/mL), anti-TG (N: 0 - 60 U/mL), vitamin B12 (N: 190 -
911 pg/mL), folic acid (N: 5.38 - 20 ng/mL) levels were
detected using Advia Centaur System (Siemens) and its
original kits by chemiluscent method. Vitamin A (N: 1.05
- 2.8 µmol/L) and vitamin E (N: 11.6 - 46.4 µmol/L) were
tested by HPLC method using Agilent 1200 equipment
and Chromosystems kits.
Statistical analyzes were performed by SPSS 16 pro-
gram. The values were presented as mean ± standard de-
viation. Mann Whitney U test was used to compare the
means between the two groups. P < 0.05 was accepted to
be significant.
3. Results
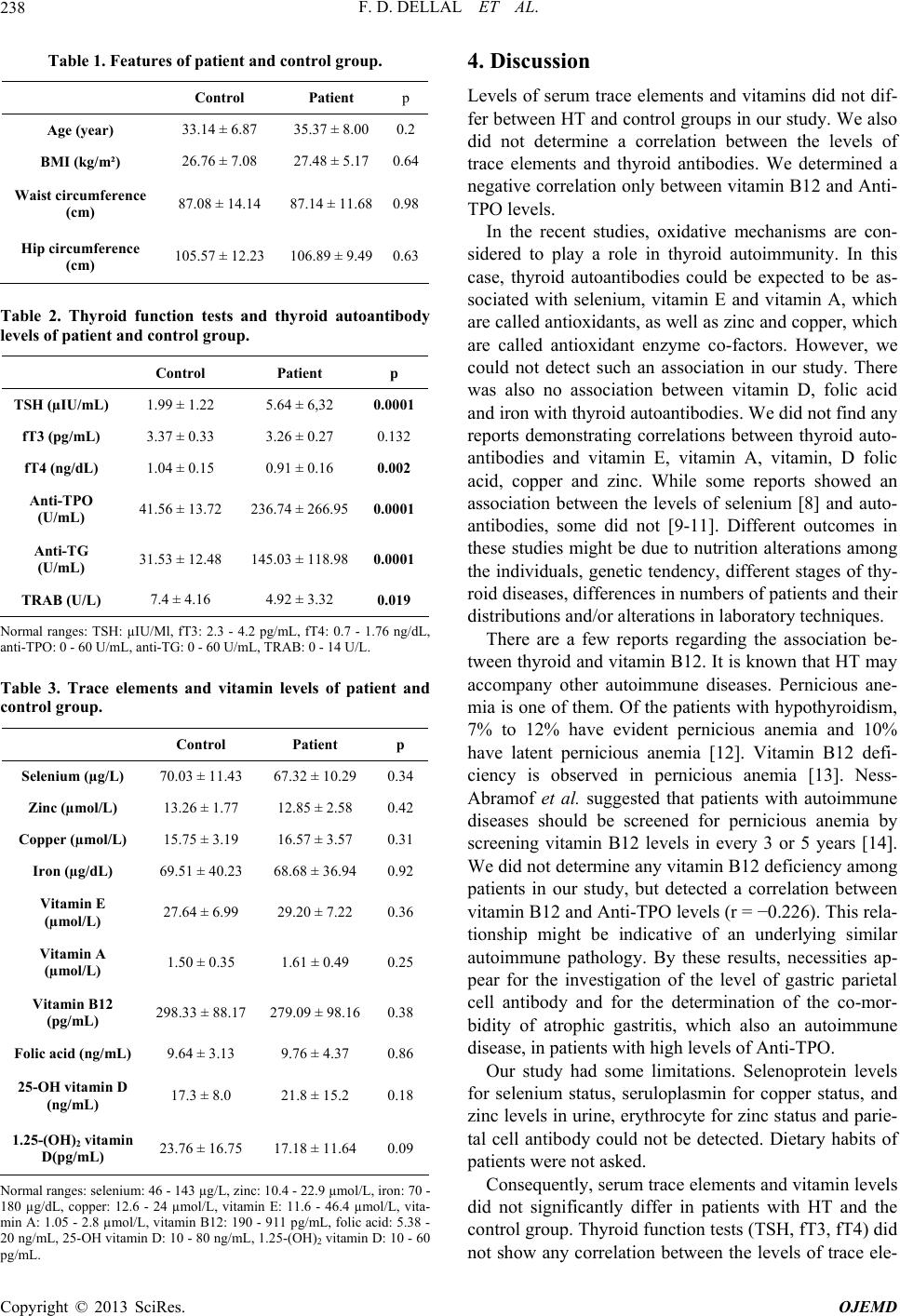
Features of Hashimoto and control groups are presented
on Table 1.
While there was a significant difference between Has-
himoto and control groups regarding TSH, fT4, Anti-
TPO, Anti-TG and TRAB, there was no significant dif-
ference in terms of FT3 (Table 2).
The levels of serum selenium, zinc, copper, iron, vita-
min E, vitamin A, vitamin B12, folic acid, 25-OH vita-
min D and 1.25-(OH)2 vitamin D did not differ between
Hashimoto and the control groups (Table 3).
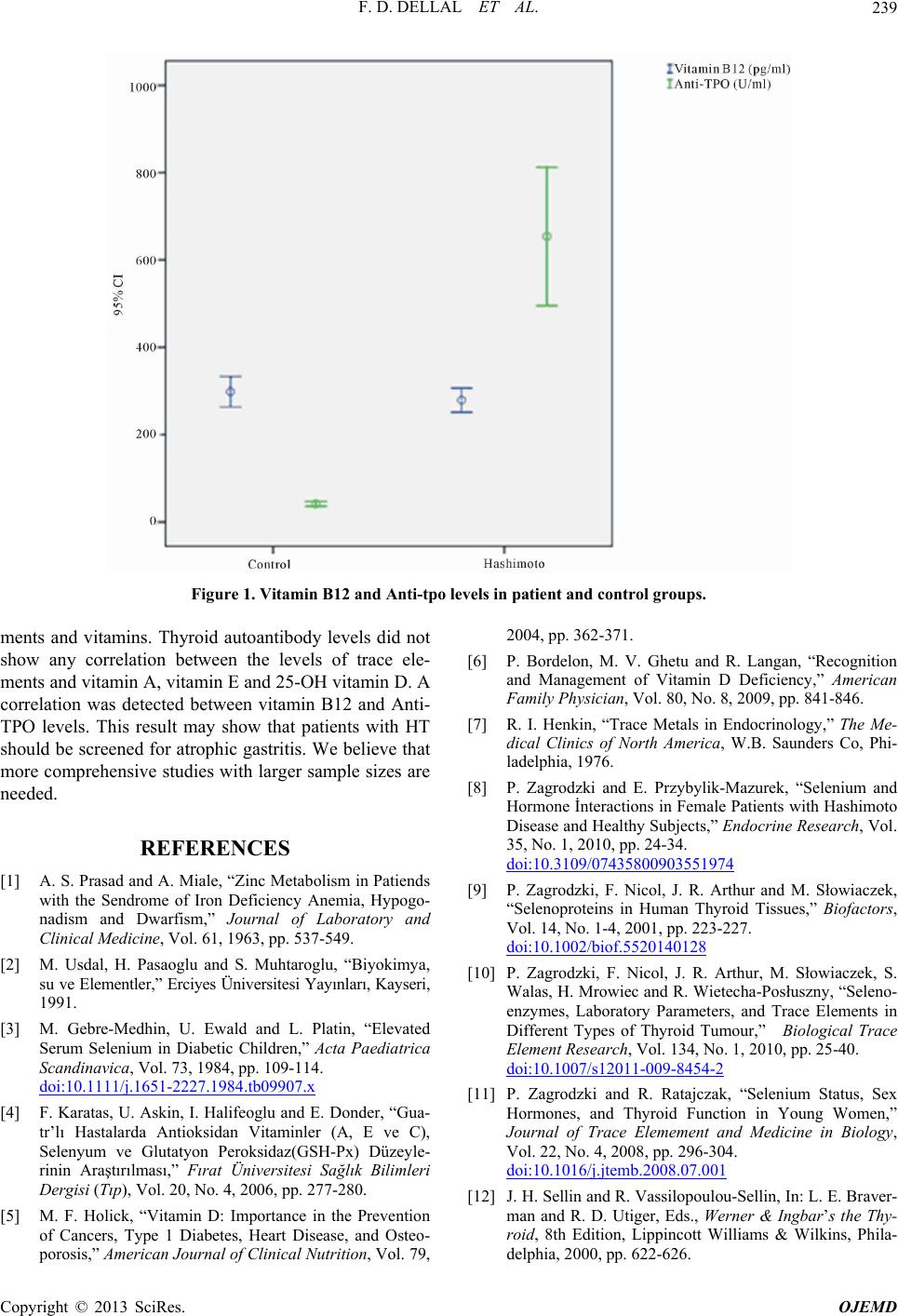
A correlation was detected between vitamin B12 and
Anti-TPO levels (r = −0.226, p = 0.04, Figure 1).
Copyright © 2013 SciRes. OJEMD