A. DEMIRTAS ET AL. 183
while the progressive scarring rate was 10.5 % in the sur-
gical group and 11.6% in the conservative group. No
significant difference was noted between the two groups
in terms of infection rates [21]. In the “International Re-
flux Study Group” study in which centers from America
and Europe collaborated 60% of cases had scarring at the
beginning, with subsequent new scarring rates of 14.6%
and 14.5% in surgical and conservative groups, respec-
tively [22].
It has been reported, and many authors agree, that
modest refluxes following megaureter surgery may re-
cover by themselves in a period of 2 - 3 months, and thus
require no therapy [23]. As further surgery in patients
with residual reflux carries the risk of ischemia and is
technically demanding, endoscopic substance infusion is
recommended. A success rate of 80% has been reported
following a single endoscopic in jection to 20 u reters with
ongoing reflux (Grade III or above in 13 ureters) follow-
ing ureteroneocystostomy [24].
Obstruction, the other common co mplication, is the re-
sult of fibrosis due to deranged ureter blood supply par-
ticularly following excisional constriction or plication.
Entry of the ureteric hiatus into the bladder from an ex-
cessive cranial and lateral aspect also causes obstruction.
In such a situation a second operation is needed. Tempo-
rary obstruction seen postoperatively, on the other hand,
is the result of edema at the lower end of the ureter and
nephrostomy usually suffices. Although our sample size
was small, we did not observe obstruction or stricture
development, suggesting that a minimal trauma to the
ureter ensues. No infection or worsening of renal func-
tion due to residual urine in the pelvicaliceal system was
observed after surgery. King reported that there is no
need for constriction to repair ureter peristaltism [1]. In
Whitaker test, a pressure gradient above 22 cm H2O be-
tween the renal pelvis an d the bladder during administra-
tion of 10 ml isotonic saline is considered diagnostic for
obstruction while 15 - 22 cm H2O suggests obstruction,
and below 15 cm H2O indicates no obstruction [8]. In
one study it has been suggested that administration of
isotonic saline at a rate of 10 ml/min may not suffice to
show obstruction in dilated urinary systems and a rate of
12 - 20 ml/min may be more appropriate [25].
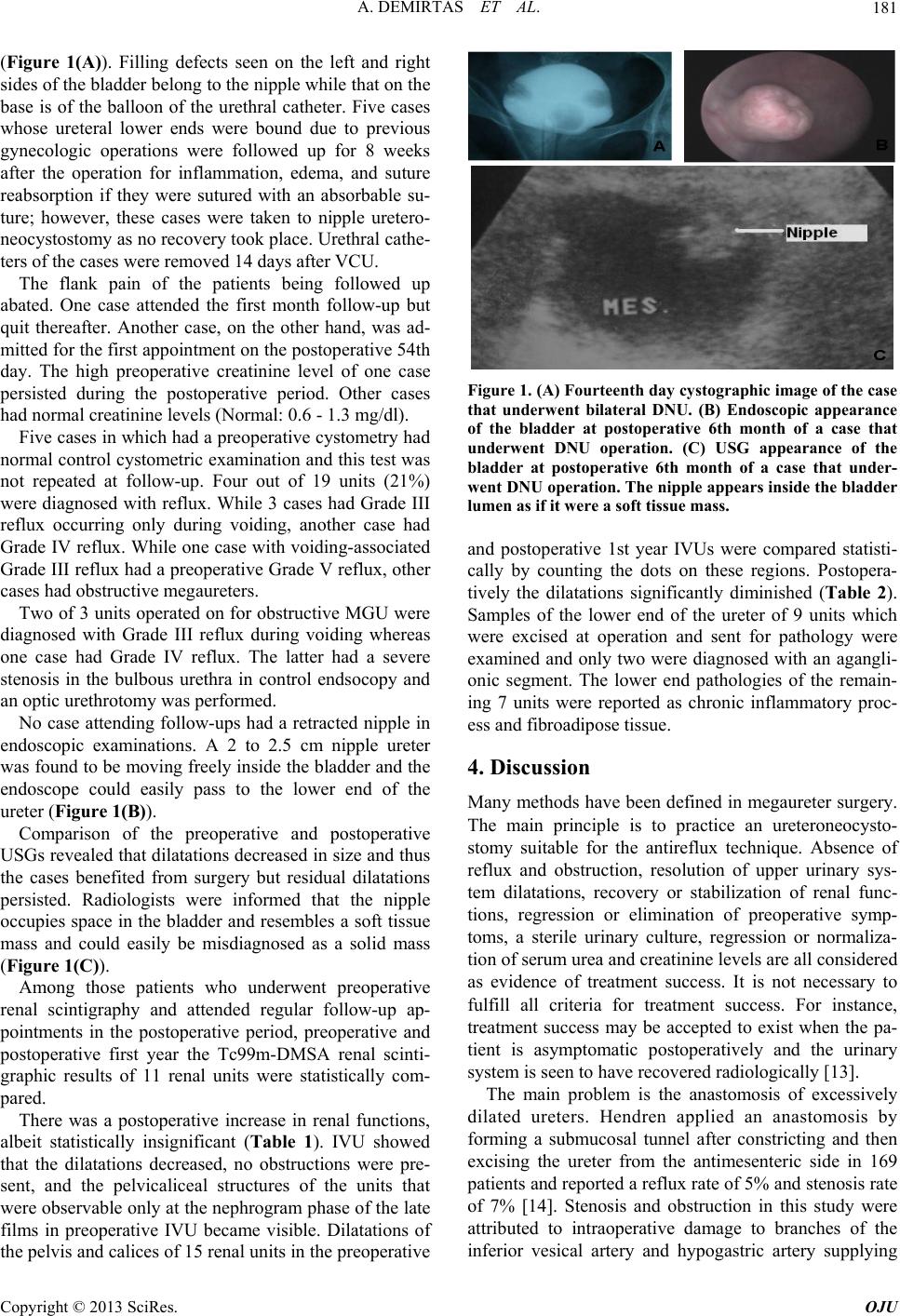
The nipple appears as a smooth-bordered filling defect
in the bladder in postoperative cystograms and IVUs
while it is observed as a soft tissue mass in the bladder in
USG. Endoscopically, the nipple prolapsing into the lu-
men is easily seen on the lateral superior wall of the
bladder and it is easy to advance through the ureter with
a cystoscope in the postoperative period. It has been cli-
nically and cystometrically shown that the nipple inside
the bladder does not produce symptoms of bladder irrita-
tion. None of the patients had irritative symptoms in the
preoperative period.
5. Conclusion
As the technique is an easy-to-perform one, the learning
curve is substantially short. Unlike the previously men-
tioned techniques, this method does not need a submu-
cosal tunnel, ureteric plication, or tapering, thus shorten-
ing surgical time and anesthetic complications, and lim-
iting the frequency of major surgical complications such
as ureteral stenosis. Lack of the need for a ureteral stent
protects the patient from stent-induced irritation and an
additional endosco pic pro cedu re. A read ily seen nipple in
the bladder and easily performed endoscopy in the post-
operative period facilitates intervention. Its potential to
be performed in obstructive and reflexive megaureter
cases including ureter dilatations caused by a variety of
etiologies such as iatrog enic ureteric lower end dilatation
may be cause to prefer the direct nipple ureteroneo-
cystostomy technique.
REFERENCES
[1] L. R. King, “Megaloureter: Definition, Diagnosis and
Management,” The Journal of Urology, Vol. 123, No. 2,
1980, pp. 222-223.
[2] A. Atala, “Vesicoureteral Reflux and Megaureter,” In: P.
C. Walsh, Ed ., Campbell’s Urology, W. B. Saunders Co.,
Philadelphia, 2002, pp. 2059-2116.
[3] H. H. Bakker, R. J. Scholtmeijer and P. J. Klopper, “Co m-
parison of 2 Different Tapering Techniques in Megau-
reters,” The Journal of Urology, Vol. 140, No. 5, 1988,
pp. 1237-1239.
[4] R. M. Ehrlich, “The Ureteral Folding Technique for Me-
gaureter Surgery,” The Journal of Urology, Vol. 134, No.
4, 1985, pp. 668-670.
[5] R. F. Mattingly, “Operative Injuries of the Ureter,” In: R.
W. Te Linde, Ed., Te Linde’s Operative Gynecology, JB
Lippincott, Philedelphia, 1995, p. 325.
[6] A. Liapis, P. Bakas, V. Giannopoulos, et al., “Ureteral
Injuries during Gynecological Surgery,” International
Urogynecology Journal and Pelvic Floor Dysfunction,
Vol. 12, No. 6, 2001, pp. 391-393.
doi:10.1007/PL00004045
[7] M. Rafique and M. H. Arif, “Management of Iatrogenic
Ureteric Injuries Associated with Gynecological Sur-
gery,” International Urology and Nephrology, Vol. 34,
No. 1, 2002, pp. 31-35. doi:10.1023/A:1021320409583
[8] R. H. Whitaker, “The Whitaker Test ,” The Urologic Clin-
ics of North America, Vol. 6, No. 3, 1979, pp. 529-539.
[9] A. Tatlisen and O. Ekmekcioglu, “Direct Nipple Ureter-
oneocystostomy in Adults with Primary Obstructed Me-
gaureter,” The Journal of Urology, Vol. 173, No. 3, 2005,
pp. 877-880. doi:10.1097/01.ju.0000152533.93716.3c
[10] N. Roberts, M. J. Puddephat and V. McNulty, “The
Benefit of Stereology for Quantitative Radiology,” The
British Journal of Radiology, Vol. 73, No. 871, 2000, pp.
679-697.
[11] J. R. Nyengaard, “Stereologic Methods and Their Appli-
Copyright © 2013 SciRes. OJU