Paper Menu >>
Journal Menu >>
 Neuroscience & Medicine, 2010, 1, 60-63 doi:10.4236/nm.2010.12009 Published Online December 2010 (http://www.SciRP.org/journal/nm) Copyright © 2010 SciRes. NM Cerebrospinal Fluid Magnesium Level in Different Neurological Disorders Haensch Carl-Albrecht Department of Neurology, University of Witten/Herdecke, HELIOS Klinikum Wuppertal, Germany Email: carl-albrecht.haensch@helios-kliniken.de Received August 30th, 2010; revised September 19th, 2010; accepted September 26th, 2010 ABSTRACT Magnesium (Mg) is an essential cofactor for many en zymatic reaction s, esp ecia lly those in vo lved in en ergy metabolism. The aim of the present study was to determine the CSF concentration of Mg in various neurological disorders (n = 72) and in healthy subjects (n = 75). The control group included 35 males and 40 females, aged 16-89 years (mean age 53 years) who were subjected to a lumbar puncture for diagnostic reasons. The CSF examination was normal mainly as concerns the macroscopically examination, the leukocyte count and the protein level. The determination of Mg was performed with xylidyl-blue photometry. Our normal CSF Mg mean value was 0.97 ± 0.08 mmol/l (range 0.6-1.4 mmol/l). In the group of patients (n = 11) with convulsive seizures a slightly but significantly lower Mg were revealed (0.92 ± 0.03 mmol/l; p = 0.001; paired two-tailed S tuden t’s t-tests). No statistically significant change of CSF Mg levels was noted in patients su ffering from alcohol withdrawal syndrome, multiple sclerosis or Bell’s palsy. Our results indi- cate that magnesium deficiency may play a role for seizure manifestation even in patients with a moderate low Mg without neurological signs. Low CSF magnesium is associated with epilepsy, further studies may determine the influ- ence of anti-epileptic drug therapy on CSF magnesium levels. Keywords: Magnesium, Cerebrospinal Fluid, Seizures, Epilepsy 1. Introduction The significance of trace elements concentration in the serum and various body fluids has been demonstrated in a number of publications. However, magnesium deter- minations in the cerebrospinal fluid (CSF) in neurologi- cal diseases has been reported only in a small number of communications [1-3]. Recently, a greater emphasis has been given to the role of trace elements in the function of the nervous syste m both in normal and pathological con- ditions. However, the results are variable and the object remains open for further investigation. It has been sug- gested that low serum Mg has occasionally been associ- ated with significant effects on the central nervous sys- tem especially in epilepsy and alcoholism. Magnesium deficiency-dependent seizures may be a relevant factor for epileptogenesis. Further studies in the future may determine the influence of anti-epileptic drug therapy on CSF magnesium levels. The existing knowledge about the impact of magnesium on epilepsy and other neuro- logical diseases is poor and controversial. Therefore, in this study, we purposed evaluation of the level of CSF concentration of Mg in a total of seventy-two neurologi- cal patients and seventy-five healthy controls. 2. Methods 2.1. Patients We studied prospectively all patients over 16 years who were subjected to a lumbar puncture for diagnostic rea- sons. The control group (n = 75) had mainly attended the Neurological Department because of headache or psycho- neurosis and the CSF examination was normal as con- cerns the mac roscopica lly examination, the leuko cyte c o unt and the protein level. Patients who were treated with magnesium or calcium supplements or any drugs that contain these electrolytes were excluded. A contraindica- tion for lumbar puncture or a loss of indication for per- formance was also exclusion criteria. Every patient had a detailed history taken and clinical ex amination, including general and neurological status by a neurologist. The lum- bar puncture was mainly performed on admission. CSF and serum magnesium levels were checked immediately afterwards. 2.2. Chemical Analysis The determination of Mg was performed with xylidyl- blue photometry (Hitachi 717). CSF analysis included: 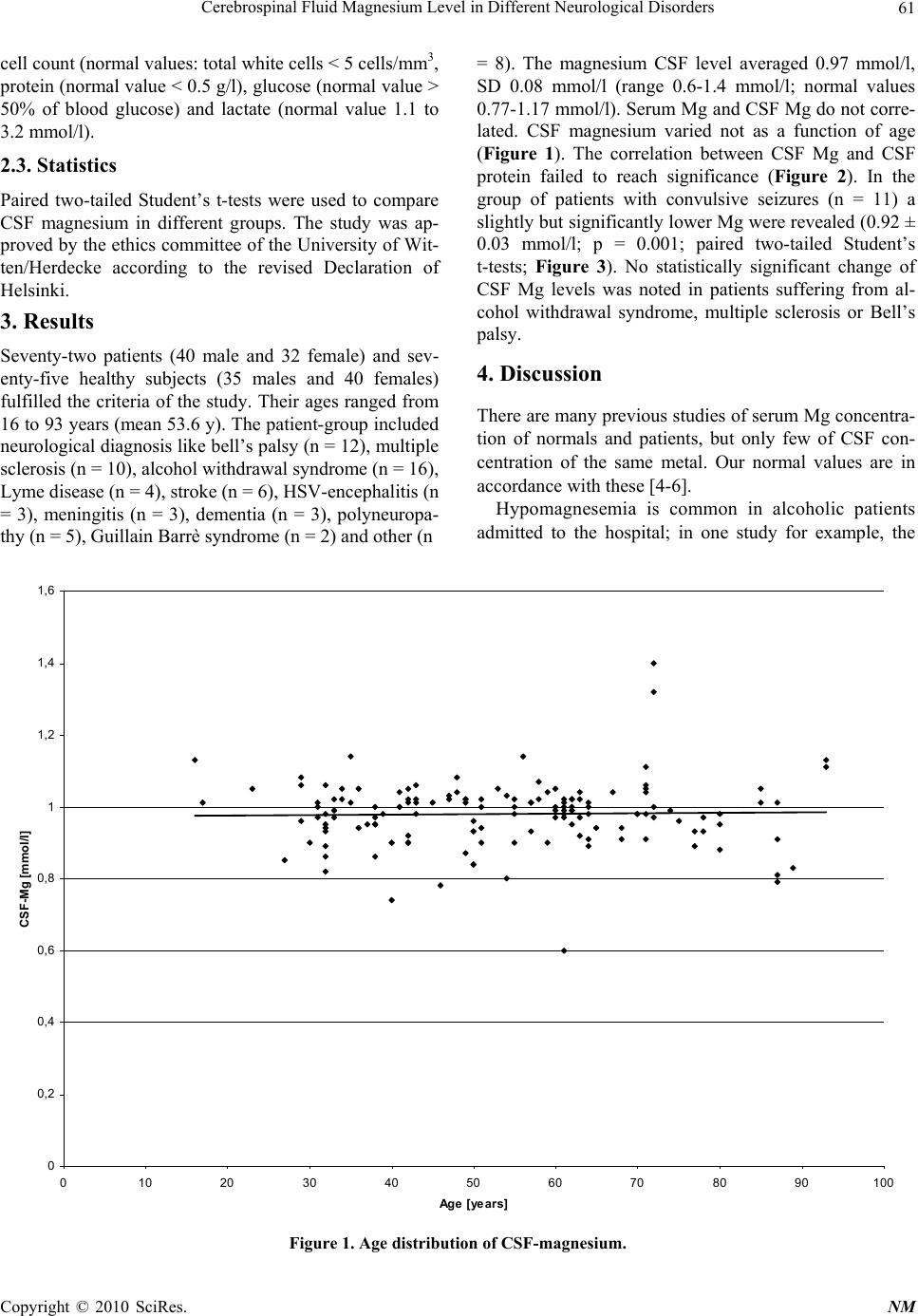 Cerebrospinal Fluid Magnesium Level in Different Neurological Disorders Copyright © 2010 SciRes. NM 61 cell count (normal values: total white cells < 5 cells/ mm3, protein (normal value < 0.5 g/l), glucose (normal value > 50% of blood glucose) and lactate (normal value 1.1 to 3.2 mmol/l). 2.3. Statistics Paired two-tailed Student’s t-tests were used to compare CSF magnesium in different groups. The study was ap- proved by the ethics committee of th e University of Wit- ten/Herdecke according to the revised Declaration of Helsinki. 3. Results Seventy-two patients (40 male and 32 female) and sev- enty-five healthy subjects (35 males and 40 females) fulfilled the criteria of the study. Their ages ranged from 16 to 93 years (mean 53.6 y). The patient-group included neurological diagno sis like bell’s palsy (n = 12), multiple sclerosis (n = 10), alcohol withdraw al syndro me (n = 16) , Lyme disease (n = 4), stroke (n = 6), HSV-encephalitis (n = 3), meningitis (n = 3), dementia (n = 3), polyneuropa- thy (n = 5), Guillain Barrè syndrome (n = 2) and other (n = 8). The magnesium CSF level averaged 0.97 mmol/l, SD 0.08 mmol/l (range 0.6-1.4 mmol/l; normal values 0.77-1.17 mmo l/l). Serum Mg and CSF Mg do not corre- lated. CSF magnesium varied not as a function of age (Figure 1). The correlation between CSF Mg and CSF protein failed to reach significance (Figure 2). In the group of patients with convulsive seizures (n = 11) a slightly but significantly lower Mg were revealed (0 .92 ± 0.03 mmol/l; p = 0.001; paired two-tailed Student’s t-tests; Figure 3). No statistically significant change of CSF Mg levels was noted in patients suffering from al- cohol withdrawal syndrome, multiple sclerosis or Bell’s palsy. 4. Discussion There are many previous studies of serum Mg concentra- tion of normals and patients, but only few of CSF con- centration of the same metal. Our normal values are in accordance with these [4-6]. Hypomagnesemia is common in alcoholic patients admitted to the hospital; in one study for example, the Figure 1. Age distribution of CSF-magnesium. 0 0,2 0,4 0,6 0,8 1 1,2 1,4 1,6 0 102030405060708090100 Age [years] CSF-Mg [mmol/l] 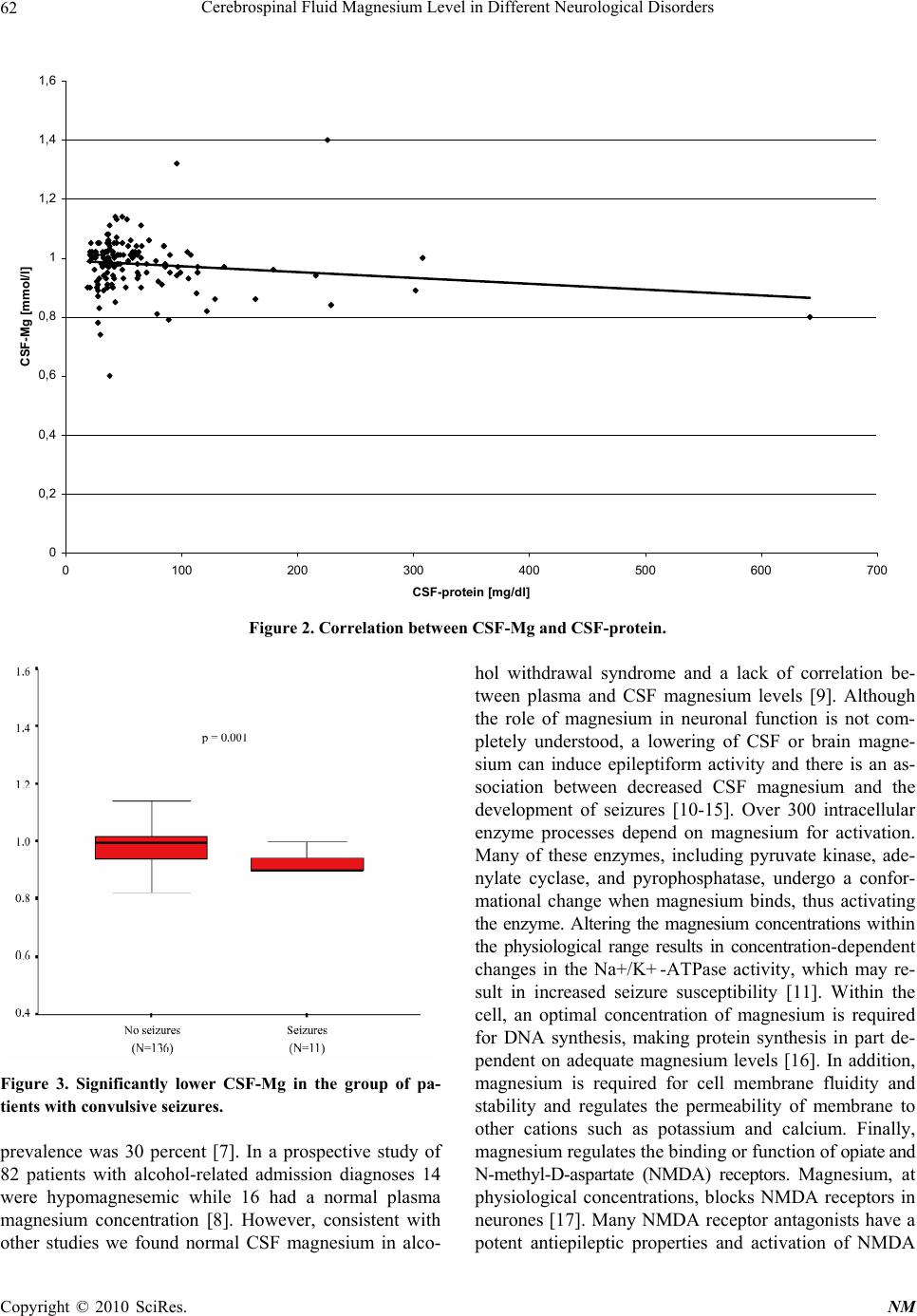 Cerebrospinal Fluid Magnesium Level in Different Neurological Disorders Copyright © 2010 SciRes. NM 62 Figure 2. Correlation betw e e n CSF-Mg and CSF-protein. Figure 3. Significantly lower CSF-Mg in the group of pa- tients with convulsive seizures. prevalence was 30 percent [7]. In a prospective study of 82 patients with alcohol-related admission diagnoses 14 were hypomagnesemic while 16 had a normal plasma magnesium concentration [8]. However, consistent with other studies we found normal CSF magnesium in alco- hol withdrawal syndrome and a lack of correlation be- tween plasma and CSF magnesium levels [9]. Although the role of magnesium in neuronal function is not com- pletely understood, a lowering of CSF or brain magne- sium can induce epileptiform activity and there is an as- sociation between decreased CSF magnesium and the development of seizures [10-15]. Over 300 intracellular enzyme processes depend on magnesium for activation. Many of these enzymes, including pyruvate kinase, ade- nylate cyclase, and pyrophosphatase, undergo a confor- mational change when magnesium binds, thus activating the enzyme. Altering the magnesium concentrations within the physiological range results in concentration-dependent changes in the Na+/K+ -ATPase activity, which may re- sult in increased seizure susceptibility [11]. Within the cell, an optimal concentration of magnesium is required for DNA synthesis, making protein synthesis in part de- pendent on adequate magnesium levels [16]. In addition, magnesium is required for cell membrane fluidity and stability and regulates the permeability of membrane to other cations such as potassium and calcium. Finally, magnesium regulates the binding or function of opiate and N-methyl-D-aspartate (NMDA) receptors. Magnesium, at physiological concentrations, blocks NMDA receptors in neurones [17]. Many NMDA receptor antagonists have a potent antiepileptic properties and activation of NMDA 0 0,2 0,4 0,6 0,8 1 1,2 1,4 1,6 0100 200 300 400 500 600 700 CSF-protein [mg/dl] CSF-Mg [mmol/l] 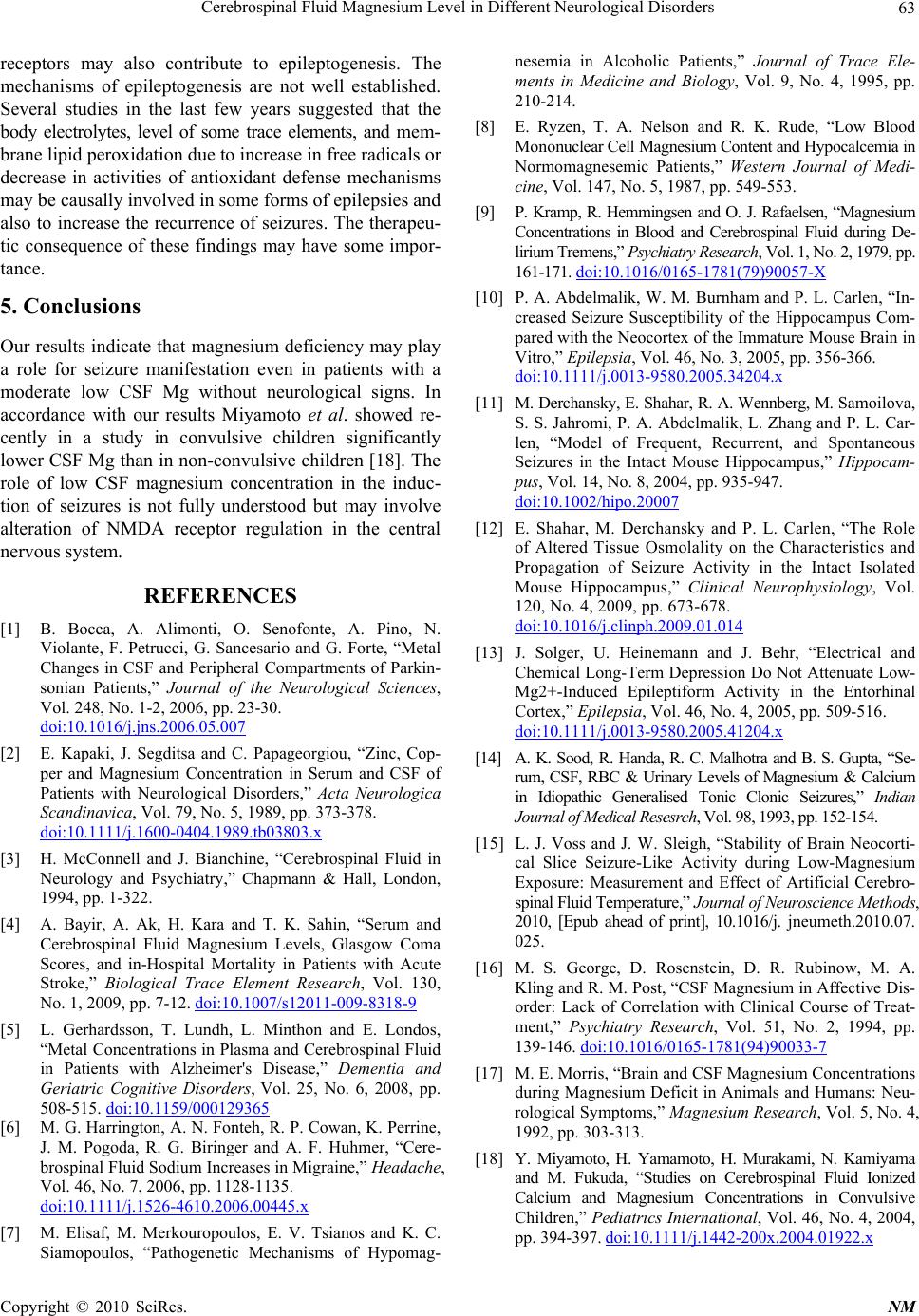 Cerebrospinal Fluid Magnesium Level in Different Neurological Disorders Copyright © 2010 SciRes. NM 63 receptors may also contribute to epileptogenesis. The mechanisms of epileptogenesis are not well established. Several studies in the last few years suggested that the body electrolytes, level of some trace elements, and mem- brane lipid peroxidation due to increase in free radicals or decrease in activities of antioxidant defense mechanisms may be causally involv ed in some forms of ep ileps ies and also to increase the recurrence of seizures. The therapeu- tic consequence of these findings may have some impor- tance. 5. Conclusions Our results indicate that magnesium deficiency may play a role for seizure manifestation even in patients with a moderate low CSF Mg without neurological signs. In accordance with our results Miyamoto et al. showed re- cently in a study in convulsive children significantly lower CSF Mg than in non-convu lsive children [18]. The role of low CSF magnesium concentration in the induc- tion of seizures is not fully understood but may involve alteration of NMDA receptor regulation in the central nervous system. REFERENCES [1] B. Bocca, A. Alimonti, O. Senofonte, A. Pino, N. Violante, F. Petrucci, G. Sancesario and G. Forte, “Metal Changes in CSF and Peripheral Compartments of Parkin- sonian Patients,” Journal of the Neurological Sciences, Vol. 248, No. 1-2, 2006, pp. 23-30. doi:10.1016/j.jns.2006.05.007 [2] E. Kapaki, J. Segditsa and C. Papageorgiou, “Zinc, Cop- per and Magnesium Concentration in Serum and CSF of Patients with Neurological Disorders,” Acta Neurologica Scandinavica, Vol. 79, No. 5, 1989, pp. 373-378. doi:10.1111/j.1600-0404.1989.tb03803.x [3] H. McConnell and J. Bianchine, “Cerebrospinal Fluid in Neurology and Psychiatry,” Chapmann & Hall, London, 1994, pp. 1-322. [4] A. Bayir, A. Ak, H. Kara and T. K. Sahin, “Serum and Cerebrospinal Fluid Magnesium Levels, Glasgow Coma Scores, and in-Hospital Mortality in Patients with Acute Stroke,” Biological Trace Element Research, Vol. 130, No. 1, 2009, pp. 7-12. doi:10.1007/s12011-009-8318-9 [5] L. Gerhardsson, T. Lundh, L. Minthon and E. Londos, “Metal Concentrations in Plasma and Cerebrospinal Fluid in Patients with Alzheimer's Disease,” Dementia and Geriatric Cognitive Disorders, Vol. 25, No. 6, 2008, pp. 508-515. doi:10.1159/000129365 [6] M. G. Harrington, A. N. Fonteh, R. P. Cowan, K. Perrine, J. M. Pogoda, R. G. Biringer and A. F. Huhmer, “Cere- brospinal Fluid Sodium Increases in Migraine,” Headache, Vol. 46, No. 7, 2006, pp. 1128-1135. doi:10.1111/j.1526-4610.2006.00445.x [7] M. Elisaf, M. Merkouropoulos, E. V. Tsianos and K. C. Siamopoulos, “Pathogenetic Mechanisms of Hypomag- nesemia in Alcoholic Patients,” Journal of Trace Ele- ments in Medicine and Biology, Vol. 9, No. 4, 1995, pp. 210-214. [8] E. Ryzen, T. A. Nelson and R. K. Rude, “Low Blood Mono nuclear Cell Magnesium Conte nt and Hypocalcemia in Normomagnesemic Patients,” Western Journal of Medi- cine, Vol. 147, No. 5, 1987, pp. 549-553. [9] P. Kramp, R. Hemmingsen and O. J. Rafaelsen, “Magnesium Concentrations in Blood and Cerebrospinal Fluid during De- lirium Tremens,” Psychia try Resear ch, Vol. 1, No. 2 , 1979, pp. 161-171. doi:10.1016/0165-1781(79)90057-X [10] P. A. Abdelmalik, W. M. Burnham and P. L. Carlen, “In- creased Seizure Susceptibility of the Hippocampus Com- pared with the Neocortex of the Immature Mouse Brain in Vitro,” Epilepsia, Vol. 46, No. 3, 2005, pp. 356-366. doi:10.1111/j.0013-9580.2005.34204.x [11] M. Derchansky, E. Shahar, R. A. Wennberg, M. Sam oi l ov a, S. S. Jahromi, P. A. Abdelmalik, L. Zhang and P. L. Car- len, “Model of Frequent, Recurrent, and Spontaneous Seizures in the Intact Mouse Hippocampus,” Hippocam- pus, Vol. 14, No. 8, 2004, pp. 935-947. doi:10.1002/hipo.20007 [12] E. Shahar, M. Derchansky and P. L. Carlen, “The Role of Altered Tissue Osmolality on the Characteristics and Propagation of Seizure Activity in the Intact Isolated Mouse Hippocampus,” Clinical Neurophysiology, Vol. 120, No. 4, 2009, pp. 67 3-678. doi:10.1016/j.clinph.2009.01.014 [13] J. Solger, U. Heinemann and J. Behr, “Electrical and Chemical Long-Term Depression Do Not Attenuate Low- Mg2+-Induced Epileptiform Activity in the Entorhinal Cortex,” Epilepsia, Vol. 46, No. 4, 2005, pp. 509-516. doi:10.1111/j.0013-9580.2005.41204.x [14] A. K. Sood, R. Handa, R. C. Malhotra and B. S. Gupta, “Se- rum, CSF, RBC & Urinary Levels of Magnesium & Calcium in Idiopathic Generalised Tonic Clonic Seizures,” Indian Journal of Medical Resesrch, Vol. 9 8, 1993, pp. 152-154. [15] L. J. Voss and J. W. Sleigh, “Stability of Brain Neocorti- cal Slice Seizure-Like Activity during Low-Magnesium Exposure: Measurement and Effect of Artificial Cerebro- spinal Fluid Temperature,” Journal of Neuroscience Methods, 2010, [Epub ahead of print], 10.1016/j. jneumeth.2010.07. 025. [16] M. S. George, D. Rosenstein, D. R. Rubinow, M. A. Kling and R. M. Post, “CSF Magnesium in Affective Dis- order: Lack of Correlation with Clinical Course of Treat- ment,” Psychiatry Research, Vol. 51, No. 2, 1994, pp. 139-146. doi:10.1016/0165-1781(94)90033-7 [17] M. E. Morris, “Brain and CSF Magnesium Concentrations during Magnesium Deficit in Animals and Humans: Neu- rological Symptoms,” Magnesium Research, Vol. 5, No. 4, 1992, pp. 303-313. [18] Y. Miyamoto, H. Yamamoto, H. Murakami, N. Kamiyama and M. Fukuda, “Studies on Cerebrospinal Fluid Ionized Calcium and Magnesium Concentrations in Convulsive Children,” Pediatrics International, Vol. 46, No. 4, 2004, pp. 394-397. doi:10.1111/j.1442-200x.2004.01922.x |