 Journal of Cancer Therapy, 2013, 4, 1-6 http://dx.doi.org/10.4236/jct.2013.47A001 Published Online August 2013 (http://www.scirp.org/journal/jct) 1 A Comparison of Breast Surgeon and Nomogram-Generated Risk Predictions of Sentinel and Non-Sentinel Node Metastases* Luisa Sugaya1, Paulo R. de Alcantara Filho1,2, Bruna Salani Mota1, Sujata Patil3, Kimberly J. Van Zee2, José Luiz B. Bevilacqua1# 1Hospital Sirio-Libanes, Sao Paulo, Brazil; 2Breast Service, Department of Surgery, Memorial Sloan-Kettering Cancer Center, New York, USA; 3Department of Epidemiology and Biostatistics, Memorial Sloan-Kettering Cancer Center, New York, USA. Email: #bevilacqua@hsl.org.br Received June 3rd, 2013; revised July 2nd, 2013; accepted July 9th, 2013 Copyright © 2013 Luisa Sugaya et al. This is an open access article distributed under the Creative Commons Attribution Li- cense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. ABSTRACT Memorial Sloan-Kettering Cancer Center (MSKCC) has developed 2 nomograms: the Sentinel Lymph Node Nomo- gram (SLNN), which is used to predict the lik elihood of sentin el lymph node (SLN ) metastases in patien ts with invasive breast cancer, and the Non-Sentinel Lymph Node Nomogram (NSLNN), which is used to predict the likelihood of re- sidual axillary disease after a positive SLN biopsy. Our purpose was to compare the accuracy of MSKCC nomogram predictions with those made by breast surgeons. Two questionnaires were built with characteristics of two sets of 33 randomly selected patients from the MSKCC Sentinel Node Database. The first included only patients with invasive breast cancer, and the second included only patients with invasive breast cancer and positive SLN biopsy. 26 randomly selected Brazilian breast surgeons were asked abou t the probability of each patient in the first set having SLN metasta- ses and each patient in the second set having additional non-SLN metastases. The predictions of the nomograms and breast surgeons were compared. There was no correlation between nomogram risk predictions and breast surgeon risk prediction estimates for either the SLNN or the NSLNN. The area under the receiver operating characteristics curves (AUCs) were 0.871 and 0.657 for SLNN and breast surgeons, respectively (p < 0.0001), and 0.889 and 0.575 for the NSLNN and breast surgeons, respectively (p < 0.0001). The nomograms were significantly more accurate as prediction tools than the risk predictions of breast surgeons in Brazil. This study demonstrates the potential utility of both nomo- grams in the decision-making process for patients with invasive breast cancer. Keywords: Sentinel Lymph Node Biopsy; Nomogram; Predictions; Breast Cancer; Completion Axillary Lymph Node Dissection 1. Introduction Over the last decades, public awareness, medical edu- cation, and increased use of screening mammography have resulted in earlier detection and treatment of invasive breast cancer, greatly improving the prognosis of those patients [1 ,2]. The adopti on of sentinel ly mph node bi opsy (SLNB) has allowed those with no ax illary metastases to avoid axillary lymph node dissection (ALND), and has reduced morbidity as a result. Since the adoption of SLNB to stage the axilla, the stand ard management of a positive SLNB has included ALND. However, only 40% - 50% of patients with positive sentinel lymph nodes (SLNs) who undergo completion axillary lymph node dissection (cALND) have additional non-SLN metastases, with favorable sub- sets of women having an even lower risk of non-SLN metastases. Women without residual nodal disease are unlikely to benefit from cALND, but are exposed to the risk of lymphedema and other morbidities. A recent randomized co ntrolled tr ial of cALND (Ame- rican College of Surgeons Oncology Group [ACOSOG] Z0011) was carried out in a selected group of clinically node-negative women with early-stage breast cancer un- dergoing breast-conserving surgery and whole breast radiation, with positive SLN. With over 6 years of follow- *The authors have no conflicts of intere st to declare. The autho rs have no funding sources to declare. #Corresponding author. Copyright © 2013 SciRes. JCT  A Comparison of Breast Surgeon and Nomogram-Generated Risk Predictions of Sentinel and Non-Sentinel Node Metastases 2 up, no statistically significant differences in local or re- gional recurrence were found in the groups that had SLNB alone and those that underwent cALND [3]. These find- ings support previous studies that suggested there is a subgroup of patients with favorable characteristics who could avoid ALND and be treated with breast-conserving surgery, radiotherapy, and adjuvant systemic therapy [4- 9]. A recent study from Memorial Sloan-Kettering Cancer Center (MSKCC) analyzed the possible impact of Z0011 on the rate of ALND using the criteria of that trial [10]. The study concluded that if the Z0011 trial criteria were applied to the MSKCC SLN database popul ation, the need for ALN D would ha ve been reduc ed by 13% i n the overall breast cancer patient population and by 48% in the subset of patients with positive SLNs. In fact, in the United States, many of those with SL N mi crometastases have not been undergoing cALND; an analysis of the National Cancer Data Base showed that in 2005 almost 50% of those with microscopic metastases in the SLN did not undergo ALND [11] . In order to estimate the likelihood of SLN metastases or to select women in whom the risk of having residual axillary disease is low, it is necessary to weigh multiple, different factors which have been shown to be predictive: tumor; sentinel node; and patient characteristics. It is difficult for a clinician to appropriately weigh all of the various factors, which increase or decrease the risk of disease simultaneously. Nomograms are useful tools that improve the accuracy of clinical judgment [12-16] and help clinicians to deal with these very complex tasks. No- mograms are prediction instruments based on regression analysis of multiple variables that translate complex cal- culations to simple graphical tools or simple software. In addition, nomograms also permit clinicians to provide more precise and comprehensible in formation to p atients, who are increasingly interested in their disease and who are increasingly taking part in the decisions regarding their treatment [17]. MSKCC has built 2 prognostic nomograms, one to predict the lik elihood of SLN metastases in patients with invasive brea st cancer (the MSKCC SLN nomogram ) [18], and one to predict the likelihood of non-SLN metastases in patients with a positive SLN biopsy (the MSKCC Non-SLN nomogram) [19]. Both are available from the MKSCC website at http://www.mskcc.org/cancer-care/ adult/breast/prediction-tools and at www.nomograms.org. The MSKCC SLN nomogram (SLNN) incorporates 9 cha- racteristics of primary breast cancer, includi ng age, tum or size, tumor type, lymphovascular invasion, tumor location, multifocality, nuclear grade, and presence of hormone receptors. The MSKCC non-SLN nomogram (NSLNN) includes the same variables, except for age and tumor location, plus characteristics of the SLNs. The NSLNN has been validated worldwide, showing its robustness in populations different from the one in which it was developed [20-24]. However, a no mogram’s utility is determined by its superiority over clinical judgment [25]. In contrast to use in the United States and Europe, the use of nomograms in Brazil and other developing countries is limited. Here we seek to compare the risk predictions of SLN metastases generated by both nomo- grams with risk predictions of SLN metastases based on the clinical judgment of breast surgeons in Brazil. 2. Materials and Methods This project was approved by the Institutional Review Boards of Hospital SírioLibanês, São Paulo, Brazil (HSL2008/13) and MSKCC. The NSLNN and SLNN were each developed in a training population, and each was then tested in an independent validation population from MSKCC [18,19]. For the present study, all patient data were de-identified. We randomly selected 33 cases from each of the validation populations used to test the original no mograms. Of 166 breast surgeons registered with the Brazilian Society of Breast Surgeons and work ing in São Paulo, we randomly selected 81 participants. Twenty-six breast surgeons agreed to participate; the others either declined to participate (n = 7) or were unable to be contacted (n = 48). All participants were volunteers and provided signed informed consent. Most of these breast surgeons were unfamiliar with the nomograms, and none had incorpo- rated their use into their clinical practice at the time of the study. Two questionnaires were adm inistered to each surgeon. In the first, data from 33 patients randomly selected from the SLNN validation population were provided: age; tu- mor size; tumor type; presence of lymphovascular inva- sion; tumor location; multifocality; nuclear grade; and estrogen and progesterone receptor status. For each pa- tient, breast surgeons were asked: “Of 100 women with invasive breast cancer with these characteristics, how many of them would you expect to have one or more po- sitive sentinel lymph nodes?” In the second questionnaire, data were presented from 33 cases from the NSLNN validation population: patho- logical size; tumor type; nuclear grade; lymphovascular invasion; multifocality and estrogen-receptor status of the primary tumor; method of detection of SLN metastases; number of positive SLNs; and number of negative SLNs. Breast surgeons were asked: “If 100 women with a positive sentinel node had these characteristics and then received a full axillary dissection, how many of them wou ld yo u e x- pect to have one or more positive non-sentinel lymph nodes?” When a response was provided as a range, the highest Copyright © 2013 SciRes. JCT 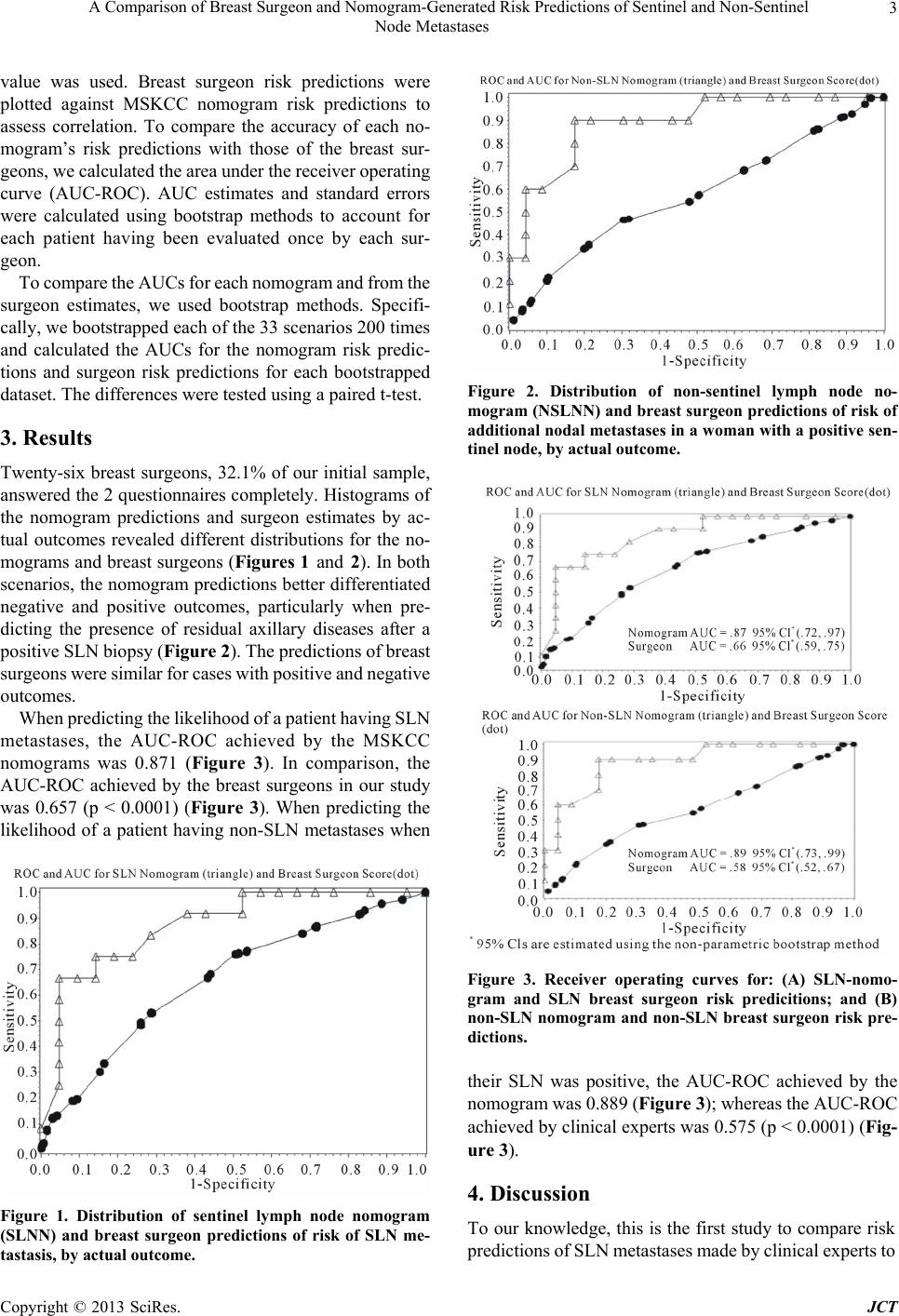 A Comparison of Breast Surgeon and Nomogram-Generated Risk Predictions of Sentinel and Non-Sentinel Node Metastases 3 value was used. Breast surgeon risk predictions were plotted against MSKCC nomogram risk predictions to assess correlation. To compare the accuracy of each no- mogram’s risk predictions with those of the breast sur- geons, we calculated the area under the recei ver operating curve (AUC-ROC). AUC estimates and standard errors were calculated using bootstrap methods to account for each patient having been evaluated once by each sur- geon. To compare the AUCs for each nomogram and from the surgeon estimates, we used bootstrap methods. Specifi- cally, we bootstrapped each of the 33 scenarios 200 times and calculated the AUCs for the nomogram risk predic- tions and surgeon risk predictions for each bootstrapped dataset. The differences were tested using a paired t-test. 3. Results Twenty-six breast surgeons, 32.1% of our initial sample, answered the 2 questionnaires completely. Histograms of the nomogram predictions and surgeon estimates by ac- tual outcomes revealed different distributions for the no- mograms and breast surgeons (Figures 1 and 2). In both scenarios, the nomogram predictions better differentiated negative and positive outcomes, particularly when pre- dicting the presence of residual axillary diseases after a positive SLN biopsy (Figure 2). The predictions of breast surgeons were similar for cases with positive and negative outcomes. When predicting the likelihood of a patient having SLN metastases, the AUC-ROC achieved by the MSKCC nomograms was 0.871 (Figure 3). In comparison, the AUC-ROC achieved by the breast surgeons in our study was 0.657 (p < 0.0001) (Figure 3). When predicting the likelihood of a patient having non-SLN metastases when Figure 1. Distribution of sentinel lymph node nomogram (SLNN) and breast surgeon predictions of risk of SLN me- tastasis, by actual outcome. Figure 2. Distribution of non-sentinel lymph node no- mogram (NSLNN) and breast surgeon predictions of risk of additional nodal metastases in a woman with a positive sen- tinel node, by actual outcome. Figure 3. Receiver operating curves for: (A) SLN-nomo- gram and SLN breast surgeon risk predicitions; and (B) non-SLN nomogram and non-SLN breast surgeon risk pre- dictions. their SLN was positive, the AUC-ROC achieved by the nomogra m was 0. 889 (Figure 3); whereas the AUC-ROC achieved by clinical experts was 0.575 (p < 0.0001) (Fig- ure 3). 4. Discussion To our knowledge, this is the first study to compare risk predictions of SLN m etastases m ade by clini cal experts to Copyright © 2013 SciRes. JCT  A Comparison of Breast Surgeon and Nomogram-Generated Risk Predictions of Sentinel and Non-Sentinel Node Metastases 4 those gener ated by MSKC C’s 2 nom ograms. Our findin gs are in agreement with previous studies [15,25,26] sug- gesting that nomograms outperform clinicians in pre- dicting clinical outcomes related to multiple variables. And, similar to prior studies [25,26], we found that the NSLNN was more accurate than the breast surgeons in our study in predicting the likelihood of non-SLN me- tastases in patients with positive SLN biopsy. Our find- ings suppor t the utility of nomograms in p redicting these outcomes. Several factors may explain the superior accuracy of the MSKCC nomograms. The use of regression models ensures that each variable contributes to the results based on their actual predictive power and relation to the crite- rion of interest. Therefore, if using the same data, nomo- grams always lead to the same conclusion, preventing the influence of random factors that often bias clinical judgment [27]. Furthermore, for clinicians, it is difficult to clearly distinguish between valid and invalid variables, and false beliefs often develop regarding associations between variables. Recall bias, control bias, fatigue, and clinical experience can also influence clinical judgment [28]. Nomograms translate complex equations through simple graphics or software, and are powerful tools that help clinicians and patients balance benefits and risks, while managing the diagnosis and treatment of the dis- ease. The recently published ACOSOG Z0011 randomized controlled trial of axillary node dissection in a selected group of women with early-stage breast cancer and posi- tive SLN underg oin g whole b reast radiation and systemic adjuvant treatment suggested that in women with a low risk of furt her met astasis, ALND m ay have no therapeut ic benefit [3] and results in increased morbidity [29-34]. During the last decade, after the introduction of the NSLNN, there has been a declining rate of ALND in patients with positive SLN [11,19], and several groups have reported a very low rate (<1%) of axillary recurrence among patients selected to no t undergo ALND [6,35- 37]. At MSKCC, when compared to those patients who did undergo cALND after a positive SLN, patients who did not undergo A LND were older, more likely to have breast conservation, and had smaller tumors, fewer high-grade lesions, less lymphovascular invasion, and lower nomo- gram scores o verall [8], suggest ing that the nomogram did identify a group at low risk of axillary recurrence. The universal use of SLN biopsy is less controversial than that of cALND, and therefore, the SLNN would not often result in a change in surgical decision making. However, the SLNN nomogram helps a breast surgeon explain to a woman the risk of nodal metastasis of her disease. The absolute risk prediction provided by the no- mogram is much more useful than knowing a list of risk factors, each associated with a hazard ratio, a nd can as sist in patient education and decision making. Nevertheless , i t is cle ar that n omo grams cannot repl ace clinical judgment. In deciding whether or not to perform SLN biopsy or completion ALND, breast surgeons also need to consider inaccuracies in the diagnoses, uncer- tainties about the progression of the disease, variable responses to treatme nt, im plica tions for system ic therapy, and the individual characteristics of each patient, such as age and psychological factors [38]. With the result s of ACOSOG Z0011, t he increasing use of nomograms, the development of more accurate tools [39,40], and a clearer identification of a subgroup of pa- tients who can safely avoid such procedures, breast sur- geons in Brazil may be encouraged to include the nomo- grams in their decision-m aking proc esses after disc ussing both related advantages and disadvantages, and the im- pact of avoiding the completion of ALND. One may argue that the major limitation of the recent randomized Z0011 trial is that of low external validity because that trial selected patients at very low risk of additional metastases. Indeed, the authors of that trial state that “most of the patients in this trial had a low axillary tumor burden” [3]. Caution at the initiation of the study led to an attempt to assure that women with high tumor burden were not randomized to SLND alone. The Z0011 trial exc luded patients wh o underwent m astectomy, had clinically palpable lymph nodes, had 3 or more posi- tive SLNs, had large tumors, and who received neoadju- vant treatment. As a result of these careful selection cri- teria, in the women randomized to ALND, only 27% had additional nodal disease identified. This is significantly lower than the more typical rate of 40% - 50% in most unselected series of clinically node-negative wo men who are found to have a positive SLN [19,39]. According to NCCN guidelines [41], completion ALND is still a standard of care for positive-SLN patients, especially in those patients who d o not fulfill the criteria of ACOSOG Z0011 (women with larger tumors; women with clinically palpable nodes or 3 or more positive SLNs; women un- dergoing mastectomy or lumpectomy without whole breast radiation). For this population, the nomogram is a useful tool to predict ad ditional metastasis. Although all the d ata in this study that were presented to the breast surgeons were taken from real cases, clinical decisions based on hypothetical situations may not re- produce real clinical scenarios. Other variables, such as years of practice, the type of hospital that the breast sur- geon interviewed worked at, previous contact with other nomograms, and willingness to participate in the study may also have influenced the results. The AUC-ROC of both nomograms were larger than the ones found in the original studies [18,19], and we randomly selected the Copyright © 2013 SciRes. JCT 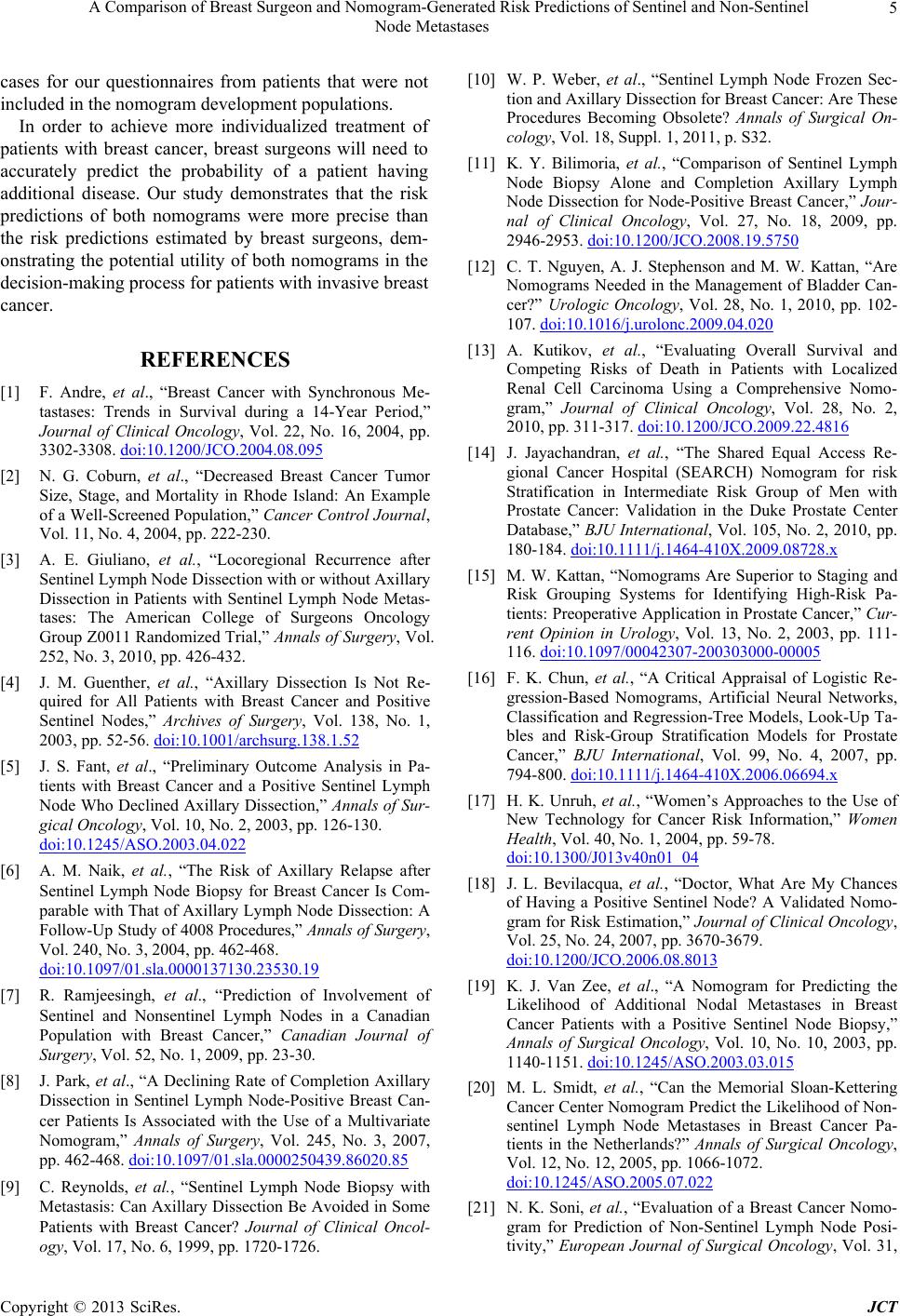 A Comparison of Breast Surgeon and Nomogram-Generated Risk Predictions of Sentinel and Non-Sentinel Node Metastases 5 cases for our questionnaires from patients that were not included in the nomogram development populations. In order to achieve more individualized treatment of patients with breast cancer, breast surgeons will need to accurately predict the probability of a patient having additional disease. Our study demonstrates that the risk predictions of both nomograms were more precise than the risk predictions estimated by breast surgeons, dem- onstrating the potential utility of both nomograms in the decision-making process for patients with invasive breast cancer. REFERENCES [1] F. Andre, et al., “Breast Cancer with Synchronous Me- tastases: Trends in Survival during a 14-Year Period,” Journal of Clinical Oncology, Vol. 22, No. 16, 2004, pp. 3302-3308. doi:10.1200/JCO.2004.08.095 [2] N. G. Coburn, et al., “Decreased Breast Cancer Tumor Size, Stage, and Mortality in Rhode Island: An Example of a Well-Screened Population,” Cancer Control Journal, Vol. 11, No. 4, 2004, pp. 222-230. [3] A. E. Giuliano, et al., “Locoregional Recurrence after Sentinel Lymph Node Dissection with or without Axillary Dissection in Patients with Sentinel Lymph Node Metas- tases: The American College of Surgeons Oncology Group Z0011 Randomized Trial,” Annals of Surgery, Vol. 252, No. 3, 2010, pp. 426-432. [4] J. M. Guenther, et al., “Axillary Dissection Is Not Re- quired for All Patients with Breast Cancer and Positive Sentinel Nodes,” Archives of Surgery, Vol. 138, No. 1, 2003, pp. 52-56. doi:10.1001/archsurg.138.1.52 [5] J. S. Fant, et al., “Preliminary Outcome Analysis in Pa- tients with Breast Cancer and a Positive Sentinel Lymph Node Who Declined Axillary Dissection,” Annals of Sur- gical Oncology, Vol. 10, No. 2, 2003, pp. 126-130. doi:10.1245/ASO.2003.04.022 [6] A. M. Naik, et al., “The Risk of Axillary Relapse after Sentinel Lymph Node Biopsy for Breast Cancer Is Com- parable with That of Axillary Lymph Node Dissection: A Follow-Up Study of 4008 Procedures,” Annals of Surgery, Vol. 240, No. 3, 2004, pp. 462-468. doi:10.1097/01.sla.0000137130.23530.19 [7] R. Ramjeesingh, et al., “Prediction of Involvement of Sentinel and Nonsentinel Lymph Nodes in a Canadian Population with Breast Cancer,” Canadian Journal of Surgery, Vol. 52, No. 1, 2009, pp. 23-30. [8] J. Park, et al., “A Declining Rate of Completion Axillary Dissection in Sentinel Lymph Node-Positive Breast Can- cer Patients Is Associated with the Use of a Multivariate Nomogram,” Annals of Surgery, Vol. 245, No. 3, 2007, pp. 462-468. doi:10.1097/01.sla.0000250439.86020.85 [9] C. Reynolds, et al., “Sentinel Lymph Node Biopsy with Metastasis: Can Axillary Dissection Be Avoided in Some Patients with Breast Cancer? Journal of Clinical Oncol- ogy, Vol. 17, No. 6, 1999, pp. 1720-1726. [10] W. P. Weber, et al., “Sentinel Lymph Node Frozen Sec- tion and Axillary Dissection for Breast Cancer: Are These Procedures Becoming Obsolete? Annals of Surgical On- cology, Vol. 18, Suppl. 1, 2011, p. S32. [11] K. Y. Bilimoria, et al., “Comparison of Sentinel Lymph Node Biopsy Alone and Completion Axillary Lymph Node Dissection for Node-Positive Breast Cancer,” Jour- nal of Clinical Oncology, Vol. 27, No. 18, 2009, pp. 2946-2953. doi:10.1200/JCO.2008.19.5750 [12] C. T. Nguyen, A. J. Stephenson and M. W. Kattan, “Are Nomograms Needed in the Management of Bladder Can- cer?” Urologic Oncology, Vol. 28, No. 1, 2010, pp. 102- 107. doi:10.1016/j.urolonc.2009.04.020 [13] A. Kutikov, et al., “Evaluating Overall Survival and Competing Risks of Death in Patients with Localized Renal Cell Carcinoma Using a Comprehensive Nomo- gram,” Journal of Clinical Oncology, Vol. 28, No. 2, 2010, pp. 311-317. doi:10.1200/JCO.2009.22.4816 [14] J. Jayachandran, et al., “The Shared Equal Access Re- gional Cancer Hospital (SEARCH) Nomogram for risk Stratification in Intermediate Risk Group of Men with Prostate Cancer: Validation in the Duke Prostate Center Database,” BJU International, Vol. 105, No. 2, 2010, pp. 180-184. doi:10.1111/j.1464-410X.2009.08728.x [15] M. W. Kattan, “Nomograms Are Superior to Staging and Risk Grouping Systems for Identifying High-Risk Pa- tients: Preoperative Application in Prostate Cancer,” Cur- rent Opinion in Urology, Vol. 13, No. 2, 2003, pp. 111- 116. doi:10.1097/00042307-200303000-00005 [16] F. K. Chun, et al., “A Critical Appraisal of Logistic Re- gression-Based Nomograms, Artificial Neural Networks, Classification and Regression-Tree Models, Look-Up Ta- bles and Risk-Group Stratification Models for Prostate Cancer,” BJU International, Vol. 99, No. 4, 2007, pp. 794-800. doi:10.1111/j.1464-410X.2006.06694.x [17] H. K. Unruh, et al., “Women’s Approaches to the Use of New Technology for Cancer Risk Information,” Women Health, Vol. 40, No. 1, 2004, pp. 59-78. doi:10.1300/J013v40n01_04 [18] J. L. Bevilacqua, et al., “Doctor, What Are My Chances of Having a Positive Sentinel Node? A Validated Nomo- gram for Risk Estimation,” Journal of Clinical Oncology, Vol. 25, No. 24, 2007, pp. 3670-3679. doi:10.1200/JCO.2006.08.8013 [19] K. J. Van Zee, et al., “A Nomogram for Predicting the Likelihood of Additional Nodal Metastases in Breast Cancer Patients with a Positive Sentinel Node Biopsy,” Annals of Surgical Oncology, Vol. 10, No. 10, 2003, pp. 1140-1151. doi:10.1245/ASO.2003.03.015 [20] M. L. Smidt, et al., “Can the Memorial Sloan-Kettering Cancer Center Nomogram Predict the Likelihood of Non- sentinel Lymph Node Metastases in Breast Cancer Pa- tients in the Netherlands?” Annals of Surgical Oncology, Vol. 12, No. 12, 2005, pp. 1066-1072. doi:10.1245/ASO.2005.07.022 [21] N. K. Soni, et al., “Evaluation of a Breast Cancer Nomo- gram for Prediction of Non-Sentinel Lymph Node Posi- tivity,” European Journal of Surgical Oncology, Vol. 31, Copyright © 2013 SciRes. JCT  A Comparison of Breast Surgeon and Nomogram-Generated Risk Predictions of Sentinel and Non-Sentinel Node Metastases Copyright © 2013 SciRes. JCT 6 No. 9, 2005, pp. 958-964. doi:10.1016/j.ejso.2005.04.011 [22] L. A. Lambert, et al., “Validation of a Breast Cancer Nomogram for Predicting Nonsentinel Lymph Node Me- tastases after a Positive Sentinel Node Biopsy,” Annals of Surgical Oncology, Vol. 13, No. 3, 2006, pp. 310-320. doi:10.1245/ASO.2006.03.078 [23] A. C. Degnim, et al., “Nonsentinel Node Metastasis in Breast Cancer Patients: Assessment of an Existing and a New Predictive Nomogram,” The American Journal of Surgery, Vol. 190, No. 4, 2005, pp. 543-550. doi:10.1016/j.amjsurg.2005.06.008 [24] A. S. Gur, et al., “Predictive Probability of Four Different Breast Cancer Nomograms for Nonsentinel Axillary Lymph Node Metastasis in Positive Sentinel Node Bi- opsy,” Journal of the American College of Surgeons, Vol. 208, No. 2, 2009, pp. 229-235. doi:10.1016/j.jamcollsurg.2008.10.029 [25] M. C. Specht, et al., “Predicting Nonsentinel Node Status after Positive Sentinel Lymph Biopsy for Breast Cancer: Clinicians versus Nomogram,” Annals of Surgical On- cology, Vol. 12, No. 8, 2005, pp. 654-659. doi:10.1245/ASO.2005.06.037 [26] M. L. Smidt, et al., “Can Surgical Oncologists Reliably Predict the Likelihood for Non-SLN Metastases in Breast Cancer Patients?” Annals of Surgical Oncology, Vol. 14, No. 2, 2007, pp. 615-620. doi:10.1245/s10434-006-9150-5 [27] R. M. Dawes, D. Faust and P. E. Meehl, “Clinical versus Actuarial Judgment,” Science, Vol. 243, No. 4899, 1989, pp. 1668-1674. doi:10.1126/science.2648573 [28] A. S. Elstein, “Heuristics and Biases: Selected Errors in Clinical Reasoning,” Academic Medicine, Vol. 74, No. 7, 1999, pp. 791-794. doi:10.1097/00001888-199907000-00012 [29] U. Veronesi, et al., “A Randomized Comparison of Sen- tinel-Node Biopsy with Routine Axillary Dissection in Breast Cancer,” The New England Journal of Medicine, Vol. 349, No. 6, 2003, pp. 546-553. doi:10.1056/NEJMoa012782 [30] L. K. Temple, et al., “Sensory Morbidity after Sentinel Lymph Node Biopsy and Axillary Dissection: A Prospec- tive Study of 233 Women,” Annals of Surgical Oncology, Vol. 9, No. 7, 2002, pp. 654-662. doi:10.1007/BF02574481 [31] M. P. Schijven, et al., “Comparison of Morbidity between Axillary Lymph Node Dissection and Sentinel Node Bi- opsy,” European Journal of Surgical Oncology, Vol. 29, No. 4, 2003, pp. 341-350. doi:10.1053/ejso.2002.1385 [32] S. A. McLaughlin, et al., “Prevalence of Lymphedema in Women with Breast Cancer 5 Years after Sentinel Lymph Node Biopsy or Axillary Dissection: Patient Perceptions and Precautionary Behaviors,” Journal of Clinical On- cology, Vol. 26, No. 32, 2008, pp. 5220-5226. doi:10.1200/JCO.2008.16.3766 [33] S. A. McLaughlin, et al., “Prevalence of Lymphedema in Women with Breast Cancer 5 Years after Sentinel Lymph Node Biopsy or Axillary Dissection: Objective Meas- urements,” Journal of Clinical Oncology, Vol. 26, No. 32, 2008, pp. 5213-5219. doi:10.1200/JCO.2008.16.3725 [34] A. Lucci, et al., “Surgical Complications Associated with Sentinel Lymph Node Dissection (SLND) plus Axillary Lymph Node Dissection Compared with SLND Alone in the American College of Surgeons Oncology Group Trial Z0011,” Journal of Clinical Oncology, Vol. 25, No. 24, 2007, pp. 3657-3663. doi:10.1200/JCO.2006.07.4062 [35] M. A. Chung, M. M. Steinhoff and B. Cady, “Clinical Axillary Recurrence in Breast Cancer Patients after a Negative Sentinel Node Biopsy,” The American Journal of Surgery, Vol. 184, No. 4, 2002, pp. 310-314. doi:10.1016/S0002-9610(02)00956-X [36] D. K. Blanchard, et al., “Relapse and Morbidity in Pa- tients Undergoing Sentinel Lymph Node Biopsy Alone or with Axillary Dissection for Breast Cancer,” Archives of Surgery, Vol. 138, No. 5, 2003, pp. 482-487. doi:10.1001/archsurg.138.5.482 [37] A. E. Giuliano, et al., “Axillary Dissection vs No Axillary Dissection in Women with Invasive Breast Cancer and Sentinel Node Metastasis: A Randomized Clinical Trial,” JAMA, Vol. 305, No. 6, 2011, pp. 569-575. doi:10.1001/jama.2011.90 [38] H. S. Cody 3rd and K. J. Van Zee, “Predicting Nonsenti- nel Node Metastases in Sentinel Node-Positive Breast Cancer: What Have We Learned, Can We Do Better, and Do We Need to?” Annals of Surgical Oncology, Vol. 15, No. 11, 2008, pp. 2998-3002. doi:10.1245/s10434-008-0133-6 [39] G. H. Lyman, et al., “American Society of Clinical On- cology Guideline Recommendations for Sentinel Lymph Node Biopsy in Early-Stage Breast Cancer,” Journal of Clinical Oncology, Vol. 23, No. 30, 2005, pp. 7703-7720. doi:10.1200/JCO.2005.08.001 [40] A. Pal, et al., “A Model for Predicting Non-Sentinel Lymph Node Metastatic Disease When the Sentinel Lymph Node Is Positive,” British Journal of Surgery, Vol. 95, No. 3, 2008, pp. 302-309. doi:10.1002/bjs.5943 [41] F. Petrelli and S. Barni, “Surgery of Primary Tumors in Stage IV Breast Cancer: An Updated Meta-Analysis of Published Studies with Meta-Regression,” Medical On- cology, Vol. 29, No. 5, 2012, pp. 3282-3290.
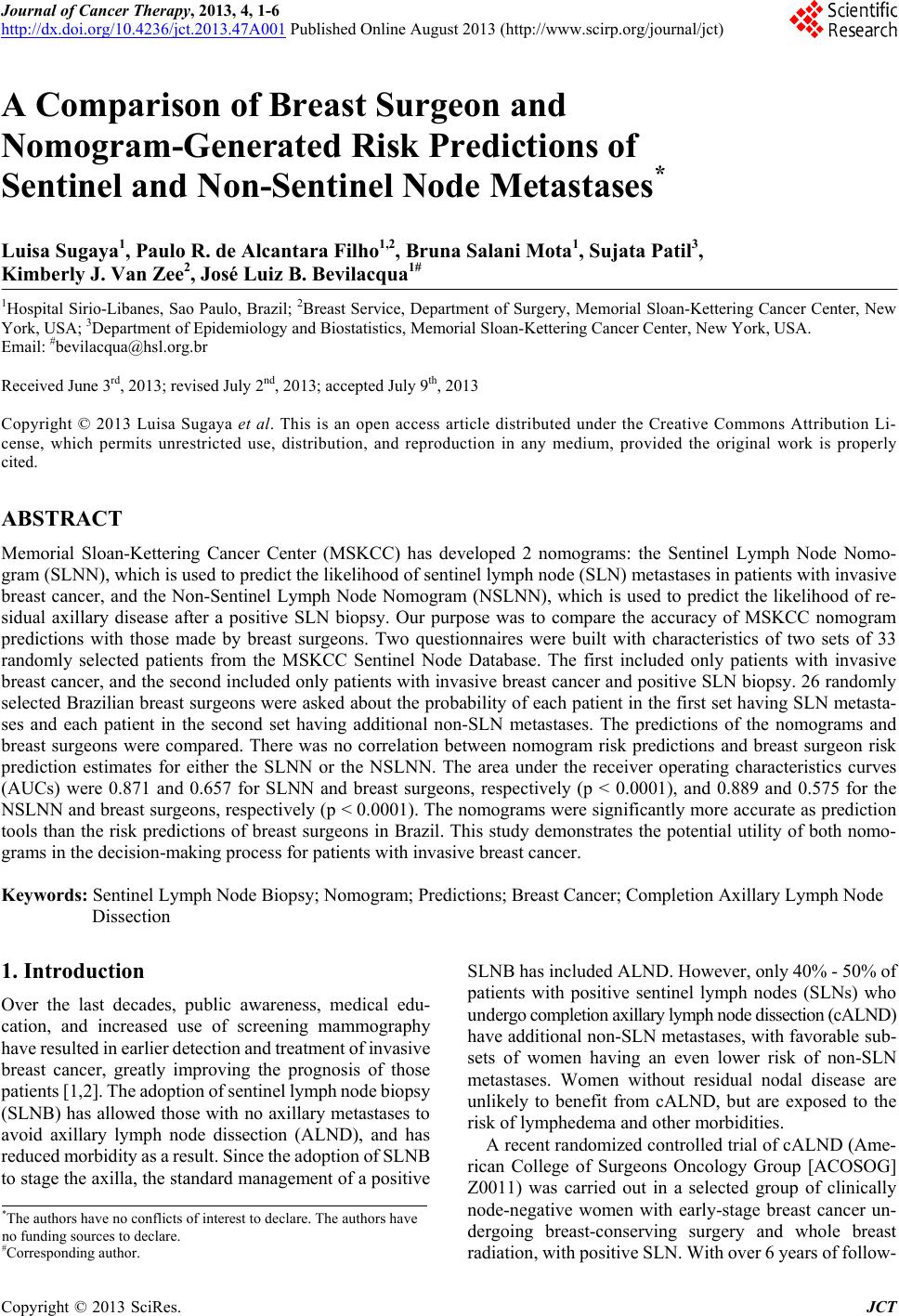
|