B. K. SARKAR ET AL.
Copyright © 2013 SciRes. WJCS
121
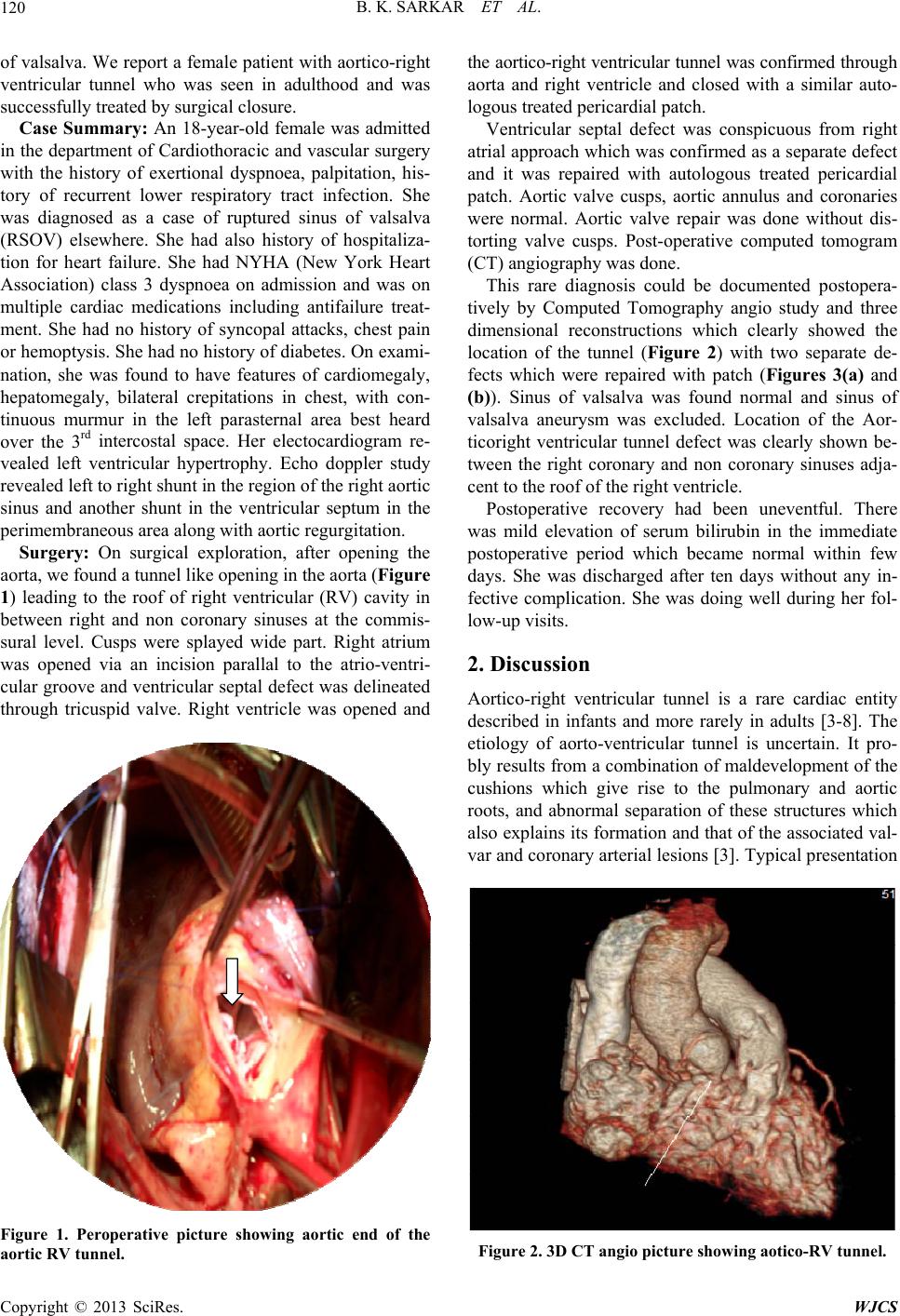
(a)
Patch closing aortico to
RV tunnel
RV
aorta
(b)
Figure 3. (a) showing patch closing VSD; (b) showing patch
closing aortic-RV tunnel.
has been a critically sick newborn with cyanosis, a “to
and fro” murmur, and signs of right heart failure [3,8].
The defect is more common in males and usually is seen
in infancy with a to and fro murmur, bounding peripheral
pulses, cardiomegaly, and dilatation of the aortic root.
The majority of patients have congestive cardiac failure,
and a precordial diastolic thrill may be palpable. These
findings may also occur with ruptured sinus of valsalva
and large coronary artery fistula. Rarity of the condition
makes its diagnosis difficult. The correct diagnosis can
be made echo-cardiographically and confirmed by car-
diac catheterization [3] but the condition may be missed
or misdiagnosed as in our case. Our initial diagnosis was
ruptured sinus of valsalva with a ventricular septal defect
with aortic regurgitation. The diagnosis was made per-
operatively and further documented post-operatively with
a CT angiography and three dimensional reconstructions
[4]. Lin and associates have described this entity in an
adult male which was successfully corrected surgically.
The diagnosis was preoperatively suspected on the basis
of echocardiography with doppler study and it was con-
firmed by a three-dimensional computed tomographic
scan. There may be associated anomaly of coronary ar-
tery origin, right ventricular outflow tract, aortic valve
abnormality and ventricular septal defect [5-8]. Talwar [5]
in their study described an anomalous right coronary
artery originating from the distal end of the tunnel. Var-
gas et al. [6] reported this anomaly in an infant and they
found the origin of the aortico-right ventricular tunnel
independently from the left coronary ostium and above
the sinus of valsalva.
Aortico-right ventricular tunnel should be considered
in the differential diagnosis in a critical patient with a “to
and fro” murmur, and signs of right heart failure. Before
surgical intervention, every effort should be made to di-
agnose the coronary artery anatomy and surgery should
be undertaken soon after the diagnosis is made. The sur-
gical intervention should be individualized based on
unique cardiac anomaly of each patient.
REFERENCES
[1] T. Generali, A. Garatti, A. Biondi, A. Varrica and L. Me-
nicanti, “Aorta to Right Atrial Shunt Due to the Rupture
of a Degen-Erative Aneurysm of the Noncoronary Sinus
of Valsalva,” Journal of Cardiovascular Medicine, Vol.
14, No. 1, 2013, pp. 71-73.
doi:10.2459/JCM.0b013e3283528f8c
[2] B. Topi, J. John, A. Agarwal, N. Nerella, V. Shetty, A.
Sadiq and J. Shani, “An Uncommon Cause of a Conti-
nuous Murmur,” Experimental & Clinical Cardiology, Vol.
17, No. 3, 2012, pp. 148-149.
[3] R. McKay, “Aorto-Ventricular Tunnel,” Orphanet Journal
of Rare Diseases, Vol. 2, 2007, p. 41.
doi:10.1186/1750-1172-2-41
[4] B. S. Lin, X. H. Zhang, Y. Z. Jiang, B. M. Zhang, D. Gao
and J. Song, “Diagnosis and Surgical Treatment of Adult
Aortico-Right Ventricular Tunnel,” The Annals of Thora-
cic Surgery, Vol. 89, No. 6, 2010, pp. 2024-2026.
doi:10.1016/j.athoracsur.2009.10.073
[5] S. Talwar, U. K. Choudhary, S. S. Kothari and B. Airan,
“Aortico-Right Ventricular Tunnel,” International Jour-
nal of Cardiology, Vol. 70, No. 2, 1999, pp. 201-205.
doi:10.1016/S0167-5273(99)00059-5
[6] F. J. Vargas, A. Molina, J. C. Martinez, M. E. Ranzini
and J. C. Vazquez, “Aortico-Right Ventricular Tunnel,”
The Annals of Thoracic Surgery, Vol. 66, No. 5, 1998, pp.
1793-1795. doi:10.1016/S0003-4975(98)00927-8
[7] J. A. Van Son, J. Hambsch, P. Schneider and F. W. Mohr,
“Repair of Aortico-Right Ventricular Tunnel,” European
Journal Cardio-Thoracic Surgery, Vol. 14, No. 2, 1998,
pp. 214-217. doi:10.1016/S1010-7940(98)00168-7
[8] S. Westaby and N. Archer, “Aortico-Right Ventricular
Tunnel,” The Annals of Thoracic Surgery, Vol. 53, No. 6,
1992, pp. 1107-1109.
doi:10.1016/0003-4975(92)90401-O