 Psychology 2013. Vol.4, No.6A1, 45-49 Published Online June 2013 in SciRes (http://www.scirp.org/journal/psych) http://dx.doi.org/10.4236/psych.2013.46A1007 Copyright © 2013 SciRes. 45 Is Interpersonal Fairness in the Doctor-Patient Relationship Associated with Long-Term Compliance in Patients with Schizophrenia?* Eva Jonas1, Guenter W. Maier2, Werner Kissling3, Johannes Hamann3 1Department of Psychology, University of Salzburg, Salzburg, Austria 2Department of Psychology, Bielefeld University, Bielefeld, Germany 3Psychiatric Department, Technical University Munich, Munich, Germany Email: eva.jonas@sbg.ac.at Received March 28th, 2013; revised April 29th, 2013; accepted May 26th, 2013 Copyright © 2013 Eva Jonas et al. This is an open access article distributed under the Creative Commons Attri- bution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Does an interpersonal fair treatment of patients with schizophrenia by their hospital psychiatrists improve patients’ intentions to take the antipsychotic medicine when leaving the hospital, long-term compliance and the perceived quality of medical treatment? 71 acutely ill in-patients with a diagnosis of schizophre- nia and their doctors were included in this study. At hospital discharge patients received a questionnaire measuring their interpersonal fairness perceptions, the perceived quality of medical treatment, and inten- tion to take the medicine. After 6 month we also measured patients’ long-term compliance. Data were analyzed by correlational analyses and path model. The results indicated that interpersonal fairness in- creased patients’ long-term compliance, which was mediated by the intention to take the medicine when leaving the hospital and the perceived quality of medical attendance. Thus, without consuming more time, an interpersonal fair treatment of patients by their doctors seems to have beneficial effects on patients’ perceived quality of medical care and long-term compliance. Theoretical and practical implications of the results are briefly discussed. Keywords: Interpersonal Fairness; Schizophrenia; Therapeutic Relationship; Adherence; Compliance; Justice Introduction Psychiatric patients see the therapeutic relationship as the most valuable part of satisfactory psychiatric care (Johansson & Eklund, 2003). Even more importantly, individuals who view their treatment and the therapeutic relationship more positively are more likely to have better treatment results, which include less severe symptoms, a lower rate of rehospitalization, and higher quality of life, as well as better social functioning (e.g., Frank & Gunderson, 1990; Hewitt & Coffey, 2005; Priebe & Gruyters, 1995). Thus, a superior therapeutic relationship seems to cause patients to be more accepting of their treatment, which then positively influences the overall outcome (Chue, 2006). This is especially the case for patients with schizophrenia (Kik- kert et al., 2006; Misdrahi, Verdoux, Lancon, & Bayle, 2009; Misdrahi, Petit, Blanc, Bayle, & Llorca, 2012). Despite the importance attributed to the therapeutic alliance there is relatively little knowledge as to what actually consti- tutes good therapeutic alliance or to how psychiatrists should communicate with their patients (McCabe & Priebe, 2008). Recent research has emphasized on procedural fairness that is, how fair do patients perceive the procedures undertaken? Here, most notably the issues of coercion and hospital admis- sion (e.g., Day et al., 2005; Galon & Wineman, 2010; Jaeger & Rossler, 2010; Lidz et al., 1998) and of shared decision making (e.g., Hamann, Leucht, & Kissling, 2003) have been investi- gated. Surprisingly little attention has been paid to interpersonal fairness, that is, whether patients feel treated with respect, po- liteness and dignity. The Concept of Interpersonal Fairness Research from different areas in psychology shows that fair- ness in various situations in daily professional and private life affects a wide range of human emotion, attitude and behavior. For example in organizational psychology research differenti- ates between four aspects of fairness: distributive (how fair are resources distributed?), procedural (how fair are the used pro- cedures?), informational (is the provision of information ade- quate?) and interpersonal fairness (Colquitt, Conlon, Wesson, Porter, & Ng, 2001). Interpersonal fairness (Greenberg, 1993) refers to the interpersonal treatment in an organization, typi- cally by the supervisor, for example do people feel they are treated with respect and propriety? Interpersonal fairness posi- tively influences psychological outcomes such as evaluation of *Financal Discolsure: Dr. Hamann has received honoraria and/or research support from Janssen-Cilag, Eli Lilly, Astra Zeneca, and Otsuka. Dr. Kissling has received honoraria from Janssen-Cilag, San-ofi-Aventis, Johnson & Johnson, Pfizer, Bristol-Myers Squibb, AstraZeneca, Lundbeck, ovartis, and Eli Lilly.  E. JONAS ET AL. an authority, job satisfaction, well-being, affective commitment toward the company and organizational citizenship behavior (Colquitt et al., 2001). Interpersonal fairness and the quality of the relationship between supervisors and subordinates are strongly related (Roch & Shanock, 2006). In psychiatric research fairness is also an important topic, al- though the focus has been more on procedural justice. Several studies, especially in the context of civil commitment hearings1 suggest that the procedural fairness patients perceive is a major issue in the context of psychiatric treatment. For example, it was found that patients who thought their point of view had been heard and taken into consideration (Susman, 1994), that is, who experienced procedural justice, rated the process as more fair than patients who did not feel like they had been heard sufficiently or taken seriously. Procedural fairness and the rat- ings of outcome fairness were also strongly related. Yet, interpersonal fairness has also been shown to be impor- tant in the context of civil commitment hearings. To many pa- tients testifying psychiatrists, state attorneys, and judges ap- peared to be disrespectful, untrusting and disinterested (Greer, O’Regan, & Traverso, 1996). In addition, the testimony of the psychiatrist often discloses private information concerning the details of the patients’ illness, which leads to embarrassment on the side of the patient. Along with Tyler we suggest that coop- eration can be improved by the way mentally ill persons view their participation, the treatment of their dignity, and trust dur- ing such hearings (Tyler, 1992). The respectful and dignified treatment of respondents by legal authorities during hearings, as well as a chance at stating their case (i.e., voice), may cause patients to be more agreeable to the notion of involuntary com- mitment. This may then lead to a domino effect, as this kind of acceptance may increase their participation within the therapeu- tic environment and, ultimately, incidents of aggressive behav- ior that necessitate seclusion and restraints may even decrease (Cascardi, Poythress, & Hall, 2000). Yet, with regard to the perceived fairness during psychiatric hospital admissions the picture may be different. In one study it was, for example, found that 80% of participants were treated with “fairness” in the admission process-whereby the volun- tary sample perceived having been treated significantly more fairly than the involuntary sample (McKenna, Simpson, Cover- dake, & Laidlaw, 2001). Does this render fairness to be a less important topic when looking at the stay in the hospital? We think not. There is evidence that procedural justice can signifi- cantly lessen the perception of coercion during hospital admis- sion (Galon & Wineman, 2010). However, what about inter- personal fairness regarding the doctor’s behavior? Building on the research reported above on the findings of interpersonal fairness in organizations we predict that interpersonal fairness in the doctor-patient relationship also positively affects the patients’ attitude towards their medication and compliance be- havior. However, what does this mean in specific? Can doctors influence the patients’ compliance by just being polite, respect- ful and considerate of the patients’ dignity? Interpersonal fairness is part of the doctor’s conduct toward the patient but the crucial point is how fair the doctor’s conduct is subjectively perceived by the patient. We propose that the perception of fairness increases the patients’ motivation to take their medicine after they have left the hospital because the per- ception of fairness should increase the patients’ perception of quality of the medical treatment and their intention (to take the medication), which has been shown to be an immediate antici- pant of behavior (Ajzen, 1991); both of which should then in- crease the patients’ long-term compliance to follow the recom- mended treatment. Finally, one might ask whether interpersonal fair treatment is doable. Do doctors have sufficient time for a fair treatment of their patients-considering the high workload of doctors in the German health system? Yet, does it actually take longer to treat patients with interpersonal fairness? It was the aim of the present analysis to test the hypothesis that an interpersonal fair treatment of patients with schizophre- nia increases patients’ long-term compliance. In addition we investigated whether this effect was mediated by patients’ in- tention to take the recommended medicine when leaving the hospital and their perception of the quality of medical treatment. Finally, we tested whether it actually took longer to treat pa- tients with interpersonal fairness. Method Seventy one acutely ill in-patients (37 [52.1%] women, 34 [47.9%] men) with a diagnosis of schizophrenia and their doc- tors were included in this study. The study took place from February 2003 to January 2004 in two psychiatric state hospitals in Germany. The data collection was embedded in a larger interventional study on a shared deci- sion making program on antipsychotic drug choice (Hamann et al., 2006; Hamann, Cohen, Leucht, Busch, & Kissling, 2007). For the present analysis we used all patients with complete data irrespectively to their allocation (intervention/control group) in the original trial. On average, the participants were 37.7 years old (SD = 11.4, range: 21 - 64 years), they had been ill for 9.6 years (SD = 9.17), had been hospitalized with schizophrenia for 4 times (SD = 5) (including the present stay), 22 (31%) had been treated because of compulsory admission, and they had stayed on av- erage for 14 days (SD = 9) on the ward when the study began and for 33 days (SD = 28) when they were discharged. The following measures were applied before hospital discharge: Interpersonal fairness. As the independent variable, three items adapted from the scale interpersonal justice of the German ver- sion of organizational justice scales (Maier, Streicher, Jonas & Woschée, 2007) were used (i.e., To what extent has the physi- cian treated you 1) in a polite manner, 2) with dignity, 3) with respect). The items were measured with scales ranging from 1 (not at all) to 5 (absolutely), Cronbach’s alpha = .83. Dependent variables. At the time of discharge from hospital (time 1), patients were asked to complete the following scales: 1) A self-report measure of the patients’ intention to take their medication, which consisted of four self-constructed items with scales ranging from 1 (totally disagree) to 5 (totally agree) (Items: I am firmly committed to take the medication. I will continue to take the medication in any case. I can well imagine to autonomously stop the mediation one day (inverted). I will surely never autonomously stop the medication), Cronbach’s alpha = .70; 1In civil commitment hearings a decision is made regarding whether or not a person who is mentally ill and who might be a danger to him/herself or others and/or who might be unable to care for him/herself without the help of another person needs an involuntary psychiatric hospitalization. 2) Perceived quality of treatment, which was assessed with 8 items (e.g., How would you judge the quality of treatment you received?), on scales ranging from 1 (low quality) to 4 (high Copyright © 2013 SciRes. 46 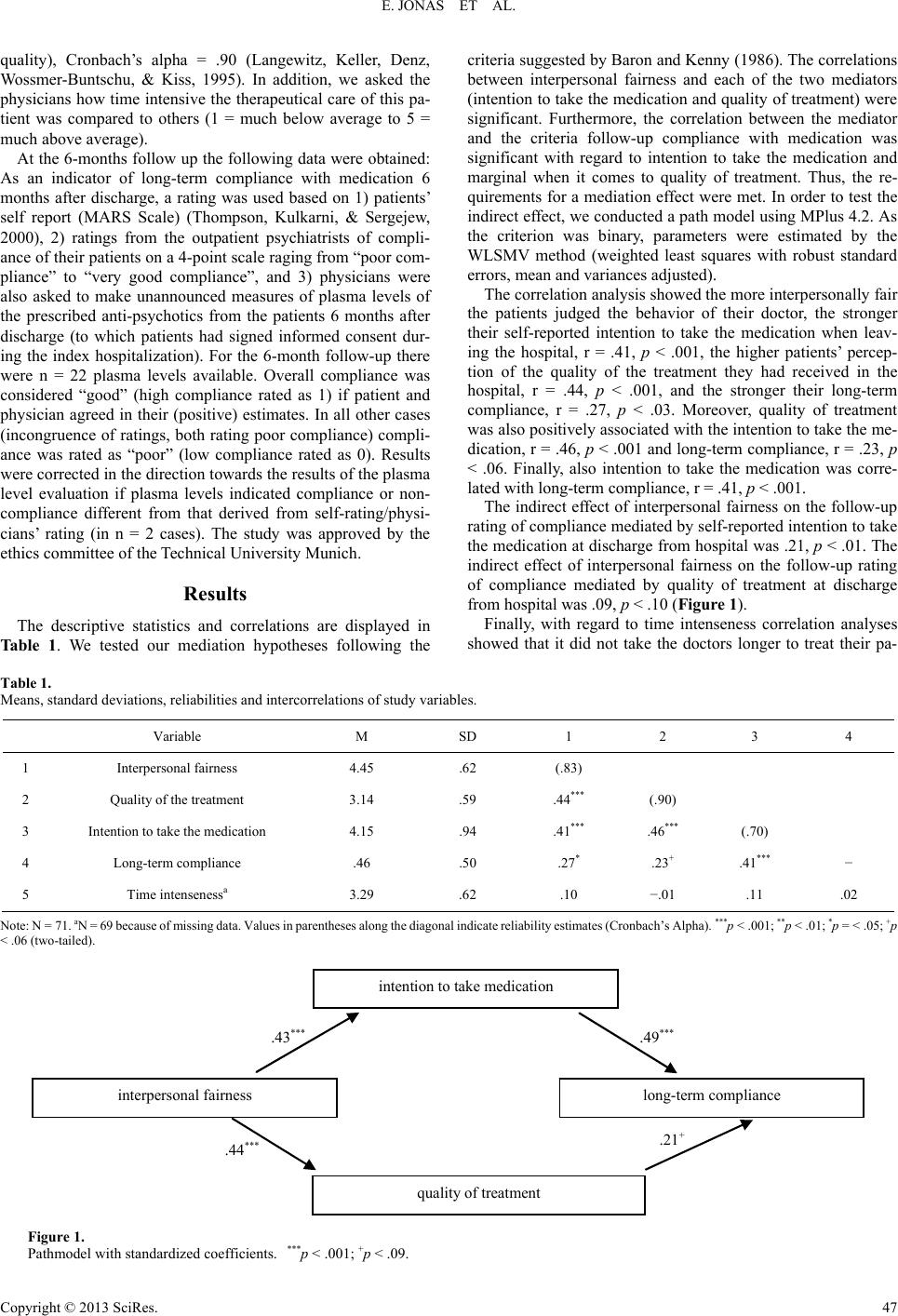 E. JONAS ET AL. Copyright © 2013 SciRes. 47 criteria suggested by Baron and Kenny (1986). The correlations between interpersonal fairness and each of the two mediators (intention to take the medication and quality of treatment) were significant. Furthermore, the correlation between the mediator and the criteria follow-up compliance with medication was significant with regard to intention to take the medication and marginal when it comes to quality of treatment. Thus, the re- quirements for a mediation effect were met. In order to test the indirect effect, we conducted a path model using MPlus 4.2. As the criterion was binary, parameters were estimated by the WLSMV method (weighted least squares with robust standard errors, mean and variances adjusted). quality), Cronbach’s alpha = .90 (Langewitz, Keller, Denz, Wossmer-Buntschu, & Kiss, 1995). In addition, we asked the physicians how time intensive the therapeutical care of this pa- tient was compared to others (1 = much below average to 5 = much above average). At the 6-months follow up the following data were obtained: As an indicator of long-term compliance with medication 6 months after discharge, a rating was used based on 1) patients’ self report (MARS Scale) (Thompson, Kulkarni, & Sergejew, 2000), 2) ratings from the outpatient psychiatrists of compli- ance of their patients on a 4-point scale raging from “poor com- pliance” to “very good compliance”, and 3) physicians were also asked to make unannounced measures of plasma levels of the prescribed anti-psychotics from the patients 6 months after discharge (to which patients had signed informed consent dur- ing the index hospitalization). For the 6-month follow-up there were n = 22 plasma levels available. Overall compliance was considered “good” (high compliance rated as 1) if patient and physician agreed in their (positive) estimates. In all other cases (incongruence of ratings, both rating poor compliance) compli- ance was rated as “poor” (low compliance rated as 0). Results were corrected in the direction towards the results of the plasma level evaluation if plasma levels indicated compliance or non- compliance different from that derived from self-rating/physi- cians’ rating (in n = 2 cases). The study was approved by the ethics committee of the Technical University Munich. The correlation analysis showed the more interpersonally fair the patients judged the behavior of their doctor, the stronger their self-reported intention to take the medication when leav- ing the hospital, r = .41, p < .001, the higher patients’ percep- tion of the quality of the treatment they had received in the hospital, r = .44, p < .001, and the stronger their long-term compliance, r = .27, p < .03. Moreover, quality of treatment was also positively associated with the intention to take the me- dication, r = .46, p < .001 and long-term compliance, r = .23, p < .06. Finally, also intention to take the medication was corre- lated with long-term compliance, r = .41, p < .001. The indirect effect of interpersonal fairness on the follow-up rating of compliance mediated by self-reported intention to take the medication at discharge from hospital was .21, p < .01. The indirect effect of interpersonal fairness on the follow-up rating of compliance mediated by quality of treatment at discharge from hospital was .09, p < .10 (Figure 1). Results Finally, with regard to time intenseness correlation analyses showed that it did not take the doctors longer to treat their pa- The descriptive statistics and correlations are displayed in Table 1. We tested our mediation hypotheses following the Table 1. Means, standard deviations, reliabilities and intercorrelations of study variables. Variable M SD 1 2 3 4 1 Interpersonal fairness 4.45 .62 (.83) 2 Quality of the treatment 3.14 .59 .44*** (.90) 3 Intention to take the medication 4.15 .94 .41*** .46*** (.70) 4 Long-term compliance .46 .50 .27* .23+ .41*** − 5 Time intensenessa 3.29 .62 .10 −.01 .11 .02 Note: N = 71. aN = 69 because of missing data. Values in parentheses along the diagonal indicate reliability estimates (Cronbach’s Alpha). ***p < .001; **p < .01; *p = < .05; +p < .06 (two-tailed). intention to take medication interpersonal fairness long-term compliance quality of treatment .43 *** .49 *** .21 + .44 *** Figure 1. Pathmodel with standardized coefficients. ***p < .001; +p < .09.  E. JONAS ET AL. tients fairly, r = .10, p > .40; patients did not perceive the qual- ity of treatment to be higher when they had spent more time with their doctor, r = −.01, p > .90, nor did their intention to take the medication, r = .11, p > .35, or their long-term compli- ance r = .02, p > .85 depend on the time the doctors spent for the treatment. Discussion The results supported our hypotheses: Interpersonal fairness was shown to increase patients’ long-term compliance with medication, which was mediated by their intention to take the medication when leaving the hospital and the perceived quality of treatment in the hospital. Moreover, a fairer treatment was not associated with the length of interaction the doctor had with the patients. We think these results have important implications. There is a body of literature on patient compliance in schizophrenia treatment (e.g., Fenton, Blyler, & Heinssen, 1997) suggesting that compliance is a complex issue. Elaborate interventions to improve compliance have been developed and have proven their efficacy (e.g., Velligan et al., 2010). However, our evi- dence also suggests that the simple fact whether a patient feels treated in a polite manner might make a difference when it comes to acceptance of and adherence with medication. As research by Hamann et al. (2011) suggests the stronger partici- pants’ perception of fairness the less important it seems to them to be involved in participating in the medical decision process. And in fact, our results even showed that there is an association between interpersonal fairness and long-term compliance. This association is mediated by patients’ intention at discharge whe- ther they want to pursue with their medication or not, which was positively influenced by the perception of interpersonal fairness regarding their doctor’s behavior. With regard to theoretical implications the therapeutic rela- tionship has been proven to be crucial for achieving good treatment results (e.g., Chue, 2006; Frank & Gunderson, 1990; Hewitt & Coffey, 2005; Priebe & Gruyters, 1995). However, what constitutes a good therapeutic relationship and which theoretical concepts help to understand the therapeutic rela- tionship? Our research suggests that the perception of interper- sonal fairness might play an especially important role in con- stituting a good therapeutic relationship. Further research is needed to better understand how the concept of interpersonal fairness is related to other aspects constituting a good therapeu- tic relationship and which aspect is crucial in achieving long- term compliance among patients. Our findings also have important practical implications. First, physicians as well as other staff members must be aware that despite the complexity of a hospital stay and despite the proven efficacy of other therapeutic strategies patients appear to be strongly influenced by a seemingly small variable—how staff talks to them. Thus, the awareness of psychiatrists that they offer a service to patients and that client satisfaction is one ma- jor goal of service provision should be adopted more thor- oughly in clinical practice. Probably this issue is often ne- glected under time pressure but it is important to keep in mind that interpersonal fairness (e.g. to apologize for a delay, to ac- cept complaints) is necessary and influences long-term out- comes. As shown, interpersonal fairness is also doable since it did not cost the psychiatrists in our study more time. Second, obviously the quality of long-term compliance is in part already certain at the time of discharge, showing the necessity to pick up the issue of compliance in therapeutic communication al- ready during hospital stay. Limitations The significance of our results is limited since we undertook a post hoc analysis. In addition psychiatrists behavior with re- gard to interpersonal fairness was not manipulated which also limits our ability to draw causal conclusions. Conclusion An interpersonally fair treatment of patients by their doctors seems to be very beneficial. Without consuming more time of interaction it increases the perceived quality of medical treat- ment and also improves long-term compliance and is thus ex- pected to reduce re-hospitalizations. Acknowledgements The authors would like to thank all participating patients and physicians. The trial was funded by the German Ministry of Health and Social Security (217-43794-5/9) within the funding project “Der Patient als Partner im medizinischen Entschei- dungsprozess”. REFERENCES Ajzen, I. (1991). Theory of planned behavior. Organizational Behavior and Human Decision Processes, 50, 179-211. doi:10.1016/0749-5978(91)90020-T Baron, R. M., & Kenny, D. A. (1986). The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psy- chology, 51, 1173-1182. doi:10.1037/0022-3514.51.6.1173 Cascardi, M., Poythress, N. G., & Hall, A. (2000). Procedural justice in the context of civil commitment: An analogue study. Behavioral Science and the Law, 18, 731-740. doi:10.1002/bsl.421 Chue, P. (2006). The relationship between patient satisfaction and treat- ment outcomes in schizophrenia. Journal of Psychopharmacology, 20, 38-56. doi:10.1177/1359786806071246 Colquitt, J. A., Conlon, D. E., Wesson, M. J., Porter, C. O., & Ng, K. Y. (2001). Justice at the Millennium: A meta-analytic review of 25 years of organizational justice research. Journal of Applied Psychol- ogy, 86, 425-445. doi:10.1037/0021-9010.86.3.425 Day, J. C., Bentall, R., Roberts, C., Randall, F., Rogers, A., Cattell, D., & Power, C. (2005). Attitudes toward antipsychotic medication: The impact of clinical variables and relationships with health profes- sionals. Archives of General Psychiatry, 62, 717-724. doi:10.1001/archpsyc.62.7.717 Fenton, W. S., Blyler, C. R., & Heinssen, R. K. (1997). Determinants of medication compliance in schizophrenia: Empirical and clinical find- ings. Schizophrenia Bulletin, 23, 637-651. doi:10.1093/schbul/23.4.637 Frank, A. F., & Gunderson, J. G. (1990). The role of the therapeutic alliance in the treatment of schizophrenia. Archives of General Psy- chiatry, 47, 228-236. doi:10.1001/archpsyc.1990.01810150028006 Galon, P. A., & Wineman, N. M. (2010). Coercion and procedural justice in psychiatric care: State of the science and implications for nursing. Archives of Psychiatric Nursing, 24, 307-316. doi:10.1016/j.apnu.2009.12.005 Greenberg, J. (1993). The social side of fairness: Interpersonal and informational classes of organizational justice. In R. Cropanzano (Ed.), Justice in the workplace: Approaching fairness in human re- source management (pp. 79-103). Hillsdale, NJ: Erlbaum. Greer, A., O’Regan, M., & Traverso, A. (1996). Therapeutic jurispru- Copyright © 2013 SciRes. 48  E. JONAS ET AL. dence and patients’ perceptions of procedural due process of civil commitment hearings. In D. Wexler, & B. Winnick (Eds.), Law in a therapeutic key: Developments in therapeutic jurisprudence (pp. 923-934). Durham, NC: Carolina Academic Press. Hamann, J., Cohen, C., Leucht, S., Busch, R., & Kissling, W. (2007). Shared decision making and long term outcome in schizophrenia treatment. Journal of Clinical Psychiatry, 68, 992-997. doi:10.4088/JCP.v68n0703 Hamann, J., Langer, B., Winkler, V., Busch, R., Cohen, R., Leucht, S., & Kissling, W. (2006). Shared decision making for in-patients with schizophrenia. Acta Psychiatrica Scandinavica, 114, 265-273. doi:10.1111/j.1600-0447.2006.00798.x Hamann, J., Leucht, S., & Kissling, W. (2003). Shared decision making in psychiatry. Acta Psychiatrica Scandinavica, 107, 403-409. doi:10.1034/j.1600-0447.2003.00130.x Hamann, J., Mendel, R., Reiter, S., Cohen, R. Bühner, M., Schebitz, M., & Berthele, A. (2011). Why do some patients with schizophrenia want to be engaged in medical decision making and others do not? The Journal of Clinical Psychiatry, 72, 1636-1643. doi:10.4088/JCP.10m06119yel Hewitt, J., & Coffey, M. (2005). Therapeutic working relationships with people with schizophrenia: Literature review. Journal of Ad- vanced Nursing, 52, 561-570. doi:10.1111/j.1365-2648.2005.03623.x Jaeger, M., & Rossler, W. (2010). Enhancement of outpatient treatment adherence: Patients’ perceptions of coercion, fairness and effective- ness. Psychiatry Research , 180, 48-53. doi:10.1016/j.psychres.2009.09.011 Johansson, H., & Eklund, M. (2003). Patients’ opinion on what consti- tutes good psychiatric care. Scandinavian Journal of Caring Sciences, 17, 339-346. doi:10.1046/j.0283-9318.2003.00233.x Kikkert, M. J., Schene, A. H., Koeter, M. W., Robson, D., Born, A., Helm, H., & Gray, R. J. (2006). Medication adherence in schizo- phrenia: Exploring patients’, carers’ and professionals’ views. Schi- zophrenia Bulletin, 32, 786-794. doi:10.1093/schbul/sbl011 Langewitz, W., Keller, A., Denz, M., Wossmer-Buntschu, B., & Kiss, A. (1995). The patient satisfaction questionnaire: A suitable tool for quality control in the physician-patient relationship? Psychotherapie, Psychosomatik, Medizinische Psychologie, 45, 351-357. Lidz, C. W., Mulvey, E. P., Hoge, S. K., Kirsch, B. L., Monahan J., Eisenberg, M., & Roth, L. (1998). Factual sources of psychiatric pa- tients’ perceptions of coercion in the hospital admission process. The American Journal of Psychiatry, 155, 1254-1260 Maier, G. W., Streicher, B., Jonas, E., & Woschée, R. (2007). Gere- chtigkeitseinschätzungen in organisationen: Die validität einer deu- tschsprachigen fassung des fragebogens von colquitt. Diagnostica, 53, 97-108. doi:10.1026/0012-1924.53.2.97 McCabe, R., & Priebe, S. (2008). Communication and psychosis: It’s good to talk, but how? British Journal of Psychiatry, 192, 404-405. doi:10.1192/bjp.bp.107.048678 McKenna, B. G., Simpson, A. I., Coverdake, J. H., & Laidlaw, T. M. (2001). An analysis of procedural justice during psychiatric hospital admission. International Journal of Law and Psychiatry, 24, 573- 581. doi:10.1016/S0160-2527(00)00069-8 Misdrahi, D., Petit, M., Blanc, O., Bayle, F., & Llorca, P. M. (2012). The influence of therapeutic alliance and insight on medication ad- herence in schizophrenia. Nordic Journal of Psychiat ry , 66, 49-54. doi:10.3109/08039488.2011.598556 Misdrahi, D., Verdoux, H., Lancon, C., & Bayle, F. (2009). The 4-Point ordinal Alliance Self-report: A self-report questionnaire for assessing therapeutic relationships in routine mental health. Comprehensive Psychiatry, 50, 181-185. doi:10.1016/j.comppsych.2008.06.010 Priebe, S., & Gruyters, T. (1995). Patients’ assessment of treatment predicting outcome. Schizophrenia Bulletin, 21, 87-94. doi:10.1093/schbul/21.1.87 Roch, S. R., & Shanock, L. R. (2006). Organizational justice in an exchange framework: Clarifying organizational justice distinctions. Journal of Management, 32, 299-322. doi:10.1177/0149206305280115 Susman, J. (1994). Resolving hospital conflicts: A study on therapeutic jurisprudence. Journal of Psychiatry and Law, 23, 107-133. Thompson, K., Kulkarni, J., & Sergejew, A. (2000). Reliability and validity of a new Medication Adherence Rating Scale (MARS) for the psychoses. Schizophrenia Research, 42, 241-247. doi:10.1016/S0920-9964(99)00130-9 Tyler, T. R. (1992). The psychological consequences of judicial proce- dures: Implications for civil commitment. SMU Law Review, 46, 433-445. Velligan, D. I., Weiden, P. J., Sajatovic, M., Scott, J., Carpenter, D., Ross, R., & Docherty, J. P. (2010). Strategies for addressing adher- ence problems in patients with serious and persistent mental illness: Recommendations from the expert consensus guidelines. Journal of Psychiatric Practice, 16, 306-324. doi:10.1097/01.pra.0000388626.98662.a0 Copyright © 2013 SciRes. 49
|