B. Wang, X. B. Huang / Advances in Reproductive Sciences 1 (2013) 1-5
4
the traditional open testicular biopsy, FNA is a quick,
low cost, less invasive and reliable procedure [21]. We
employed this method in 306 patients with NOA and had
67 cases of successful sperm recovery. Th e probability o f
sperm retrieval in our study was 21.89% that was lower
than other study (such as 26.4% in the study of Bettella,
A.). If we make a pre-operation evaluation of sperm re-
covery in terms of the combined parameters of inhibin B,
FSH and LH, the probability of sperm retrieval in FNA
may increase.
In our study, there was statistically significant differ-
ence between successful and unsuccessful sperm recov-
ery groups in terms of mean serum inhibin B, FSH and
LH levels. But individual hormone is not reliable in pre-
diction of sperm recovery before invasive procedures. In
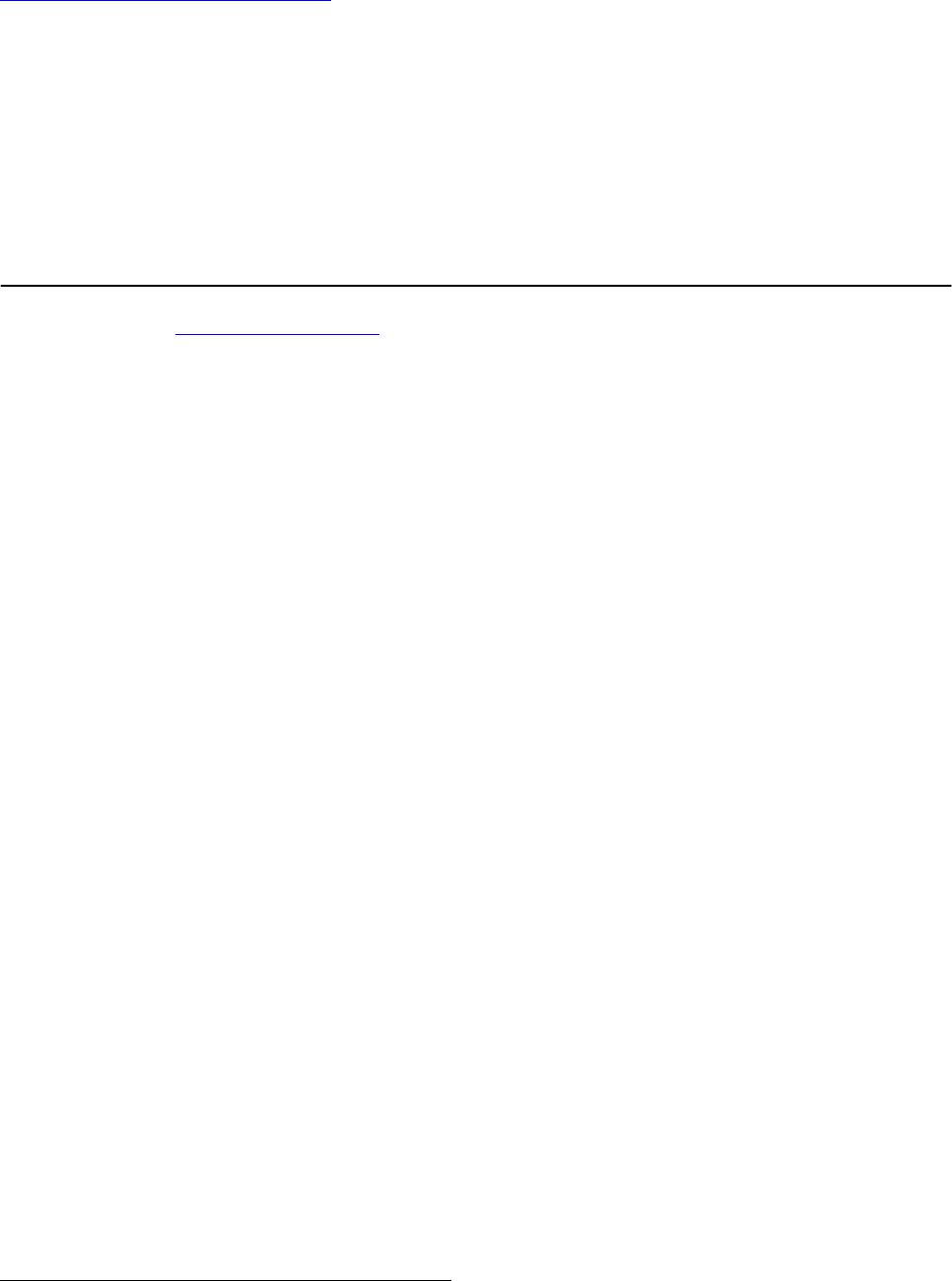
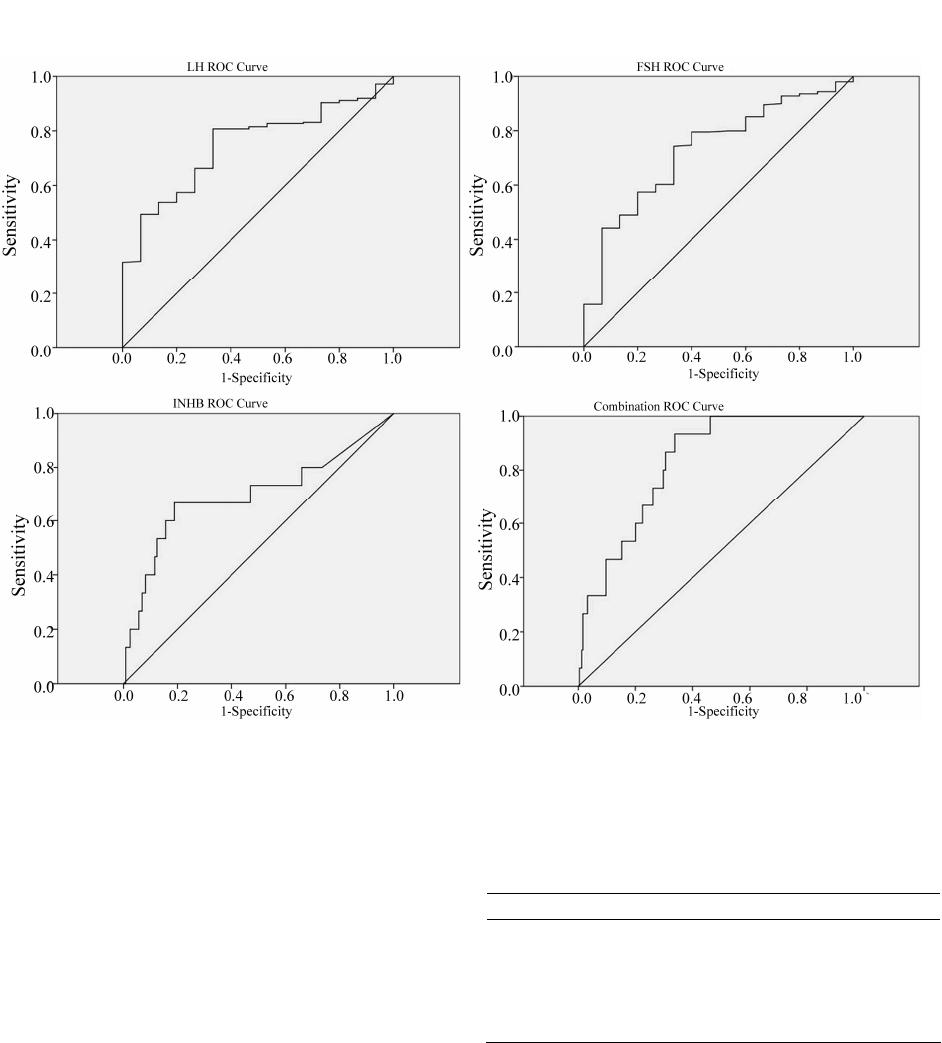
order to obtain more reliable prediction, ROC curve is
used to evaluate the results. We found that the area under
the curve of inhibin B, FSH and LH were 0.696, 0.729
and 0.747 respectively. When three of them were as-
sessed together, we found that the area under the curve
increased to 0.832. The predictive power was signifi-
cantly improved by the combination of inhibin B, FSH
and LH. The cut-off points were 27.31 pg/ml for inhibin
B, 11.68 IU/L for FSH, and 4.04 IU/L for LH. We noted
that in the successful sperm recovery group, there were
58 of 67 (86.5%) patients with a serum level of inhibin B
> 27.31 pg/mL, FSH < 11.68 IU/L, and LH < 4.40 IU/L.
While in the unsuccessful sperm recovery group, only 4
of 239 (1.67%) reached that level. The result can give a
clue to clinical counseling. When the patients have a
serum level of inhibin B > 27.31 pg/mL, FSH < 11.68
IU/L, and LH < 4.40 IU/L at the same time, the probabil-
ity of sperm recovery is quite high. However, in other
individuals with a serum level of inhibin B < 27.31
pg/mL, FSH > 11.68 IU/L, and LH > 4.40 IU/L are not
able to predict absence of sperm due to multifactor in-
fluence spermatogenesis in testes. So the cut-off points
of these three hormones may be set up as a powerful pre-
dictor for successful sperm retrieval for patients with
NOA. For patients whose values of inhibin B, FSH and
LH are over the cut-off points, if sperm retrieval failed,
we advise them to take open microsurgical biopsies.
5. CONCLUSION
In conclu sion, though inhibin B, FSH and LH ar e use-
ful predictors of sperm retrieval in patients with NOA,
the combined evaluation of them would be more power-
ful in the predicting of successful sperm recovery for
patients with NOA before decision making of FNA pro-
cedure.
REFERENCES
[1] Palermo, G., Joris, H., Devroey, P. and Van Steirteghem,
A.C. (1992) Pregnancies after intracytoplasmic injection
of single spermatozoon into an oocyte. Lancet, 340, 17-
18. doi:10.1016/0140-6736(92)92425-F
[2] Devroey, P, Liu, J., Nagy, Z., Goossens, A., Tournaye, H.,
Camus, M., et al. (1995) Pregnancies after testicular
sperm extraction and intracytoplasmic sperm injection in
non-obstructive azoospermia. Human Reproduction, 10,
1457-1460. doi:10.1093/HUMREP/10.6.1457
[3] Su, L.M., Palermo, G.D., Goldstein, M., Veeck, L.L.,
Rosenwaks, Z. and Schlegel, P.N. (1999) Testicular sperm
extraction with intracytoplasmic sperm injection for non-
obstructive azoospermia: Testicular histology can predict
success of sperm retrieval. Journal of Urology, 161, 112-
116. doi:10.1016/S0022-5347(01)62079-2
[4] Seo, J.T. and Ko, W.J. (2001) Predictive factors of suc-
cessful testicular sperm recovery in non-obstructive azo-
ospermia patients. International Journal of Andrology, 24,
306-310. doi:10.1046/j.1365-2605.2001.00307.x
[5] Beierdorffer, H. and Schirren, C. (1979) Peculiarities and
side effects of testicular biopsy. Andrologia, 11, 31 1-319.
d oi :10. 1111/j .1439 -0272.1979.tb02212.x
[6] Bettella, A., Ferlin, A., Menegazzo, M., Ferigo, M., Tavo-
lini, I.M., Bassi, P.F., et al. (2005) Testicular fine needle
aspiration as a diagnostic tool in non-obstructive azoo-
spermia. Asian Journal of Andrology, 7, 289-294.
d oi :10. 1111/j .1745 -7262.2005.00043.x
[7] Burger, H.G. (1993) Clinical review 46: Clinical utility of
inhibin measurements. The Journal of Clinical Endocri-
nology & Metabolism, 76, 1391-1396.
doi:10.1210/jc.76.6.1391
[8] Pierik, F.H., Vreeburg, J.T., Stijnen, T., De Jong, F.H. and
Weber, R.F. (1998) Serum inhibin B as a marker of sper-
matogenesis. The Journal of Clinical Endocrinology &
Metabolism, 83, 3110-3114.
doi:10.1210/jc.83.9.3110
[9] de Kretser, D.M. (1979) Endocrinology of male infertile-
ity. British Medical Bulletin, 35, 187-192.
[10] O’Donnell, L., McLachlan, R.I., Wreford, N.G. and
Robertson, D.M. (1994) Testosterone promotes the con-
version of round spermatids between stages VII and VIII
of the rat spermatogenic cycle. Endocrinology, 135, 2608-
2614. doi:10.1210/en.135.6.2608
[11] Matsumoto, A.M. and Bremner, W.J. (1987) Endocrinol-
ogy of the hypothalamic-pituitary-testicular axis with par-
ticular reference to the hormonal control of spermato-
genesis. Baillière’s Clinical Endocrinology and Metabo-
lism, 1, 71-87. doi:10.1016/S0950-351X(87)80053-8
[12] Ziaee, S.A., Ezzatnegad, M., Nowroozi, M., Jamshidian,
H., Abdi, H. and Hosseini, M.S. (2006) Prediction of suc-
cessful sperm retrieval in patients with nonobstructive
azoospermia. Journal of Urology, 3, 92-96.
[13] von Eckardstein, S., Simoni, M., Bergmann, M., Wein-
bauer, G.F., Gassner, P., Schepers, A.G., et al. (1999) Se-
rum inhibin B in combination with serum follicle-stimu-
lating hormone (FSH) is a more sensitive marker than
serum FSH alone for impaired spermatogenesis in men,
but cannot predict the presence of sperm in testicular tis-
sue samples. The Journal of Clinical Endocrinology &
Copyright © 2013 SciRes. OPEN A CCESS