M. ESTIVALS ET AL.
Copyright © 2013 SciRes. OJRD
43
responsible for almost 50% of deaths [6], so intensive
initial treatment is recommended.
Two years after initial diagnosis, the patient remains
treated with azathioprine and small doses of corticoster-
oids (5 mg/day of prednisone). There has been no relapse
at the cardiovascular level, but respiratory function re-
mains below normal (LVEF = 3.4 liters at 100% of theo-
retical values, Tiffeneau = 73%, and mean peak expira-
tory flow 25/75 at 2.73 liters so 73% of theoretical values).
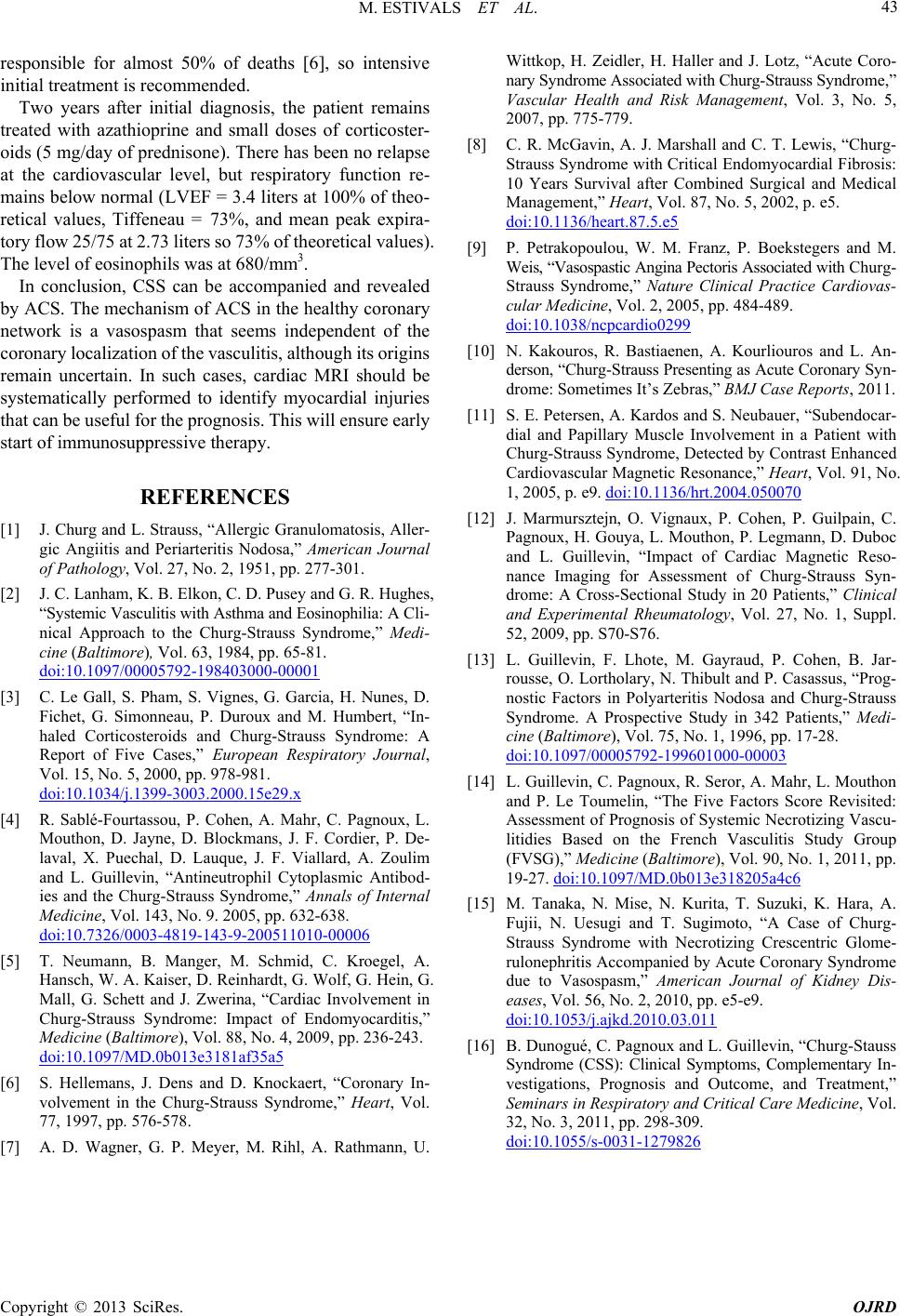
The level of eosinophils was at 6 80/mm3.
In conclusion, CSS can be accompanied and revealed
by ACS. The mechanism of ACS in the healthy coronary
network is a vasospasm that seems independent of the
coronary localization of the vasculitis, although its origins
remain uncertain. In such cases, cardiac MRI should be
systematically performed to identify myocardial injuries
that can be useful for the prognosis. This will ensure early
start of immunosuppressive therapy.
REFERENCES
[1] J. Churg and L. Strauss, “Allergic Granulomatosis, Aller-
gic Angiitis and Periarteritis Nodosa,” American Journal
of Pathology, Vol. 27, No. 2, 1951, pp. 277-301.
[2] J. C. Lanham, K. B. Elkon, C. D. Pusey and G. R. Hughes,
“Systemic Vasculitis with Asthma and Eosinophili a: A Cli-
nical Approach to the Churg-Strauss Syndrome,” Medi-
cine (Baltimore), Vol. 63, 1984, pp. 65-81.
doi:10.1097/00005792-198403000-00001
[3] C. Le Gall, S. Pham, S. Vignes, G. Garcia, H. Nunes, D.
Fichet, G. Simonneau, P. Duroux and M. Humbert, “In-
haled Corticosteroids and Churg-Strauss Syndrome: A
Report of Five Cases,” European Respiratory Journal,
Vol. 15, No. 5, 2000, pp. 978-981.
doi:10.1034/j.1399-3003.2000.15e29.x
[4] R. Sablé-Fourtassou, P. Cohen, A. Mahr, C. Pagnoux, L.
Mouthon, D. Jayne, D. Blockmans, J. F. Cordier, P. De-
laval, X. Puechal, D. Lauque, J. F. Viallard, A. Zoulim
and L. Guillevin, “Antineutrophil Cytoplasmic Antibod-
ies and the Churg-Strauss Syndrome,” Annals of Internal
Medicine, Vol. 143, No. 9. 2005, pp. 632-638.
doi:10.7326/0003-4819-143-9-200511010-00006
[5] T. Neumann, B. Manger, M. Schmid, C. Kroegel, A.
Hansch, W. A. Kaiser, D. Reinhardt, G. Wolf, G. Hein, G.
Mall, G. Schett and J. Zwerina, “Cardiac Involvement in
Churg-Strauss Syndrome: Impact of Endomyocarditis,”
Medicine (Baltimore), Vol. 88, No. 4, 2009, pp. 236-243.
doi:10.1097/MD.0b013e3181af35a5
[6] S. Hellemans, J. Dens and D. Knockaert, “Coronary In-
volvement in the Churg-Strauss Syndrome,” Heart, Vol.
77, 1997, pp. 576-578.
[7] A. D. Wagner, G. P. Meyer, M. Rihl, A. Rathmann, U.
Wittkop, H. Zeidler, H. Haller and J. Lotz, “Acute Coro-
nary Syndrome Associated with Churg-Strauss Syndrome,”
Vascular Health and Risk Management, Vol. 3, No. 5,
2007, pp. 775-779.
[8] C. R. McGavin, A. J. Marshall and C. T. Lewis, “Churg-
Strauss Syndrome with Critical Endomyocardial Fibrosis:
10 Years Survival after Combined Surgical and Medical
Management,” Heart, Vol. 87, No. 5, 2002, p. e5.
doi:10.1136/heart.87.5.e5
[9] P. Petrakopoulou, W. M. Franz, P. Boekstegers and M.
Weis, “Vasospastic Angina Pectoris Associate d with Ch u r g -
Strauss Syndrome,” Nature Clinical Practice Cardiovas-
cular Medicine, Vol. 2, 2005, pp. 484-489.
doi:10.1038/ncpcardio0299
[10] N. Kakouros, R. Bastiaenen, A. Kourliouros and L. An-
derson, “Churg-Strauss Pre senting as Acute Coronary Sy n-
drome: Sometimes It’s Zebras,” BMJ Case Reports, 2011.
[11] S. E. Petersen, A. Kardos and S. Neubauer, “Subendocar-
dial and Papillary Muscle Involvement in a Patient with
Churg-Strauss Syndrome, Detected by Contrast Enhanced
Cardiovascular Magnetic Resonance,” Heart, Vol. 91, No.
1, 2005, p. e9. doi:10.1136/hrt.2004.050070
[12] J. Marmursztejn, O. Vignaux, P. Cohen, P. Guilpain, C.
Pagnoux, H. Gouya, L. Mouthon, P. Legmann, D. Duboc
and L. Guillevin, “Impact of Cardiac Magnetic Reso-
nance Imaging for Assessment of Churg-Strauss Syn-
drome: A Cross-Sectional Study in 20 Patients,” Clinical
and Experimental Rheumatology, Vol. 27, No. 1, Suppl.
52, 2009, pp. S70-S76.
[13] L. Guillevin, F. Lhote, M. Gayraud, P. Cohen, B. Jar-
rousse, O. Lortholary , N. Thibult and P. Casassus, “Prog-
nostic Factors in Polyarteritis Nodosa and Churg-Strauss
Syndrome. A Prospective Study in 342 Patients,” Medi-
cine (Baltimore), Vol. 75, No. 1, 1996, pp. 17-28.
doi:10.1097/00005792-199601000-00003
[14] L. Guillevin, C. Pagnoux, R. Seror, A. Mahr, L. Mouthon
and P. Le Toumelin, “The Five Factors Score Revisited:
Assessment of Prognosis of Systemic Necrotizing Vascu-
litidies Based on the French Vasculitis Study Group
(FVSG),” Medicine (Baltimore), Vol. 90, No. 1, 2011, pp.
19-27. doi:10.1097/MD.0b013e318205a4c6
[15] M. Tanaka, N. Mise, N. Kurita, T. Suzuki, K. Hara, A.
Fujii, N. Uesugi and T. Sugimoto, “A Case of Churg-
Strauss Syndrome with Necrotizing Crescentric Glome-
rulonephritis Accompanied by Acute Coronary Syndrome
due to Vasospasm,” American Journal of Kidney Dis-
eases, Vol. 56, No. 2, 2010, pp. e5-e9.
doi:10.1053/j.ajkd.2010.03.011
[16] B. Dunogué, C. Pagnoux and L. Guillevin, “Churg-Stauss
Syndrome (CSS): Clinical Symptoms, Complementary In-
vestigations, Prognosis and Outcome, and Treatment,”
Seminars in Respiratory and Critical Care Medicine, Vol.
32, No. 3, 2011, pp. 298-309.
doi:10.1055/s-0031-1279826