 Open Journal of Respiratory Diseases, 2013, 3, 31-38 http://dx.doi.org/10.4236/ojrd.2013.32006 Published Online May 2013 (http://www.scirp.org/journal/ojrd) Differential Mechanis ms of the Effect of Peroxisome Proliferator-Activated Receptor Gamma Agonists on Bleomycin-Induced Lung Fibrosis Keisuke Miyamoto1, Sadatomo Tasaka1*, Yasushi Nakano1, Hiromi Shinoda1, Hirofumi Kamata1, Wakako Yamasawa2, Makoto Ishii1, Naoki Hasegawa3, Tomoko Betsuyaku1 1Division of Pulmonary Medicine, Keio University School of Medicine, Tokyo, Japan 2Department of Laboratory Medicine, Keio University School of Medicine, Tokyo, Japan 3Center for Infectious Diseases and Infection Control, Keio University School of Medicine, Tokyo, Japan Email: *tasaka@cpnet.med.keio.ac.jp Received March 1, 2013; revised April 3, 2013; accepted April 11, 2013 Copyright © 2013 Keisuke Miyamoto et al. This is an open access article distributed under the Creative Commons Attribution Li- cense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. ABSTRACT Background and Objectives: Peroxisome proliferator-activated receptor- (PPAR- ) is a nuclear receptor whose acti- vation regulates inflammation and fibrosis in various organs. We aimed to investigate the effect of two PPAR- ligands, telmisartan and rosiglitazone, on lung injury and fibrosis induced by intratracheal bleomycin (BLM). Methods: Lung injury and fibrosis was induced in female C57Bl/6 mice by intratracheal instillation of 1.0 mg/kg of BLM. Some of the animals received rosiglitazone intraperitoneally or telmisartan in drinking water. Bronchoalveolar lavage (BAL) was performed 2, 7, 14 or 21 days after BLM instillation for cell counting and measurement of mediators in the lung. In a separate series, the lungs were sampled for collagen assay and histopathological evaluation. Results: Treatment with rosiglitazone or telmisartan significantly attenuated the BLM-induced increases in lung collagen content, pathological score, and inflammatory cells in BAL fluid. Rosiglitazone significantly suppressed BLM-induced elevation of TGF- 1, MCP-1, and IL-6 levels in the lung. In contrast, telmisartan made no changes in these cytokines, whereas it mitigated the BLM-induced increase in prostaglandin F2 in the lung. Higher concentrations of rosiglitazone and telmisartan at- tenuated proliferation of lung fibroblasts in vitro. Conclusions: Two PPAR- ligands, rosiglitazone and telmisartan, exert protective effects on BLM-induced lung fibrosis through the suppression of different profibrotic mediators. Keywords: Peroxisome Proliferator-Activated Receptor- ; Bleomycin; Pulmonary Fibrosis; Transforming Growth Factor- 1; Prostaglandin F2 1. Introduction Idiopathic pulmonary fibrosis is a progressive, life- threatening, interstitial lung disease that is characterized morphologically by thickening of the alveolar septa with collagen deposition and myofibroblast proliferation, and by a diffuse inflammatory infiltrate [1]. Much of the in- formation regarding the development of pulmonary fi- brosis has been acquired with a well-characterized ani- mal model in which lung fibrosis is induced by intratra- cheal administration of the antineoplastic agent bleomy- cin (BLM) [2]. In rodents, BLM administration induces acute inflammatory response followed by fibroblast pro- liferation and increased collagen content in the lung [3]. Various mediators are involved in the pathogenesis of pulmonary fibrosis, although the detailed mechanisms are still not well understood [4,5]. Peroxisome proliferator-activated receptor- (PPAR- ), which is a member of a family of ligand-activated nu- clear transcriptional factors, plays a critical role in nor- mal lung development, injury, and repair [6,7]. PPAR- ligands inhibit a variety of inflammatory actions in macrophages, including expression of inducible nitric oxide synthase, superoxide dismutase, gelatinase, matrix metalloproteinase and several interleukins [8,9]. There is accumulating evidence indicating that PPAR- is an im- portant regulator of inflammation, fibrosis and immune responses in various diseases including pancreatic fibro- sis, liver fibrosis and collagen vascular diseases [10]. *Corresponding author. C opyright © 2013 SciRes. OJRD 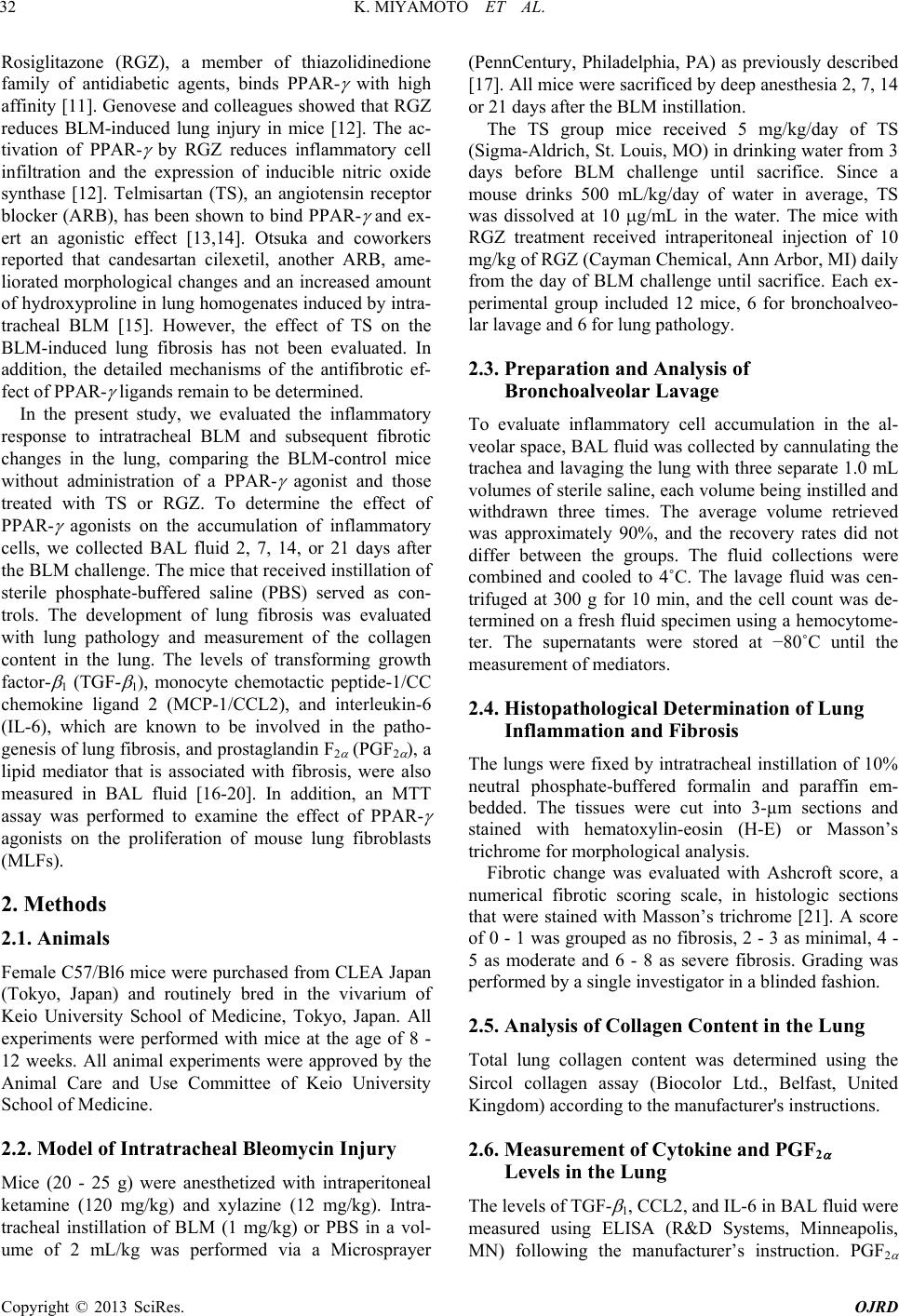 K. MIYAMOTO ET AL. 32 Rosiglitazone (RGZ), a member of thiazolidinedione family of antidiabetic agents, binds PPAR- with high affinity [11]. Genovese and colleagues showed that RGZ reduces BLM-induced lung injury in mice [12]. The ac- tivation of PPAR- by RGZ reduces inflammatory cell infiltration and the expression of inducible nitric oxide synthase [12]. Telmisartan (TS), an angiotensin receptor blocker (ARB), has been shown to bind PPAR- and ex- ert an agonistic effect [13,14]. Otsuka and coworkers reported that candesartan cilexetil, another ARB, ame- liorated morphological changes and an increased amount of hydroxyproline in lung homogenates induced by intra- tracheal BLM [15]. However, the effect of TS on the BLM-induced lung fibrosis has not been evaluated. In addition, the detailed mechanisms of the antifibrotic ef- fect of PPAR- ligands remain to be determined. In the present study, we evaluated the inflammatory response to intratracheal BLM and subsequent fibrotic changes in the lung, comparing the BLM-control mice without administration of a PPAR- agonist and those treated with TS or RGZ. To determine the effect of PPAR- agonists on the accumulation of inflammatory cells, we collected BAL fluid 2, 7, 14, or 21 days after the BLM challenge. The mice that received instillation of sterile phosphate-buffered saline (PBS) served as con- trols. The development of lung fibrosis was evaluated with lung pathology and measurement of the collagen content in the lung. The levels of transforming growth factor- 1 (TGF- 1), monocyte chemotactic peptide-1/CC chemokine ligand 2 (MCP-1/CCL2), and interleukin-6 (IL-6), which are known to be involved in the patho- genesis of lung fibrosis, and prostaglandin F2 (PGF2 ), a lipid mediator that is associated with fibrosis, were also measured in BAL fluid [16-20]. In addition, an MTT assay was performed to examine the effect of PPAR- agonists on the proliferation of mouse lung fibroblasts (MLFs). 2. Methods 2.1. Animals Female C57/Bl6 mice were purchased from CLEA Japan (Tokyo, Japan) and routinely bred in the vivarium of Keio University School of Medicine, Tokyo, Japan. All experiments were performed with mice at the age of 8 - 12 weeks. All animal experiments were approved by the Animal Care and Use Committee of Keio University School of Medicine. 2.2. Model of Intratracheal Bleomycin Injury Mice (20 - 25 g) were anesthetized with intraperitoneal ketamine (120 mg/kg) and xylazine (12 mg/kg). Intra- tracheal instillation of BLM (1 mg/kg) or PBS in a vol- ume of 2 mL/kg was performed via a Microsprayer (PennCentury, Philadelphia, PA) as previously described [17]. All mice were sacrificed by deep anesthesia 2, 7, 14 or 21 days after the BLM instillation. The TS group mice received 5 mg/kg/day of TS (Sigma-Aldrich, St. Louis, MO) in drinking water from 3 days before BLM challenge until sacrifice. Since a mouse drinks 500 mL/kg/day of water in average, TS was dissolved at 10 g/mL in the water. The mice with RGZ treatment received intraperitoneal injection of 10 mg/kg of RGZ (Cayman Chemical, Ann Arbor, MI) daily from the day of BLM challenge until sacrifice. Each ex- perimental group included 12 mice, 6 for bronchoalveo- lar lavage and 6 for lung pathology. 2.3. Preparation and Analysis of Bronchoalveolar Lavage To evaluate inflammatory cell accumulation in the al- veolar space, BAL fluid was collected by cannulating the trachea and lavaging the lung with three separate 1.0 mL volumes of sterile saline, each volume being instilled and withdrawn three times. The average volume retrieved was approximately 90%, and the recovery rates did not differ between the groups. The fluid collections were combined and cooled to 4˚C. The lavage fluid was cen- trifuged at 300 g for 10 min, and the cell count was de- termined on a fresh fluid specimen using a hemocytome- ter. The supernatants were stored at −80˚C until the measurement of mediators. 2.4. Histopathological Determination of Lung Inflammation and Fibrosis The lungs were fixed by intratracheal instillation of 10% neutral phosphate-buffered formalin and paraffin em- bedded. The tissues were cut into 3-µm sections and stained with hematoxylin-eosin (H-E) or Masson’s trichrome for morphological analysis. Fibrotic change was evaluated with Ashcroft score, a numerical fibrotic scoring scale, in histologic sections that were stained with Masson’s trichrome [21]. A score of 0 - 1 was grouped as no fibrosis, 2 - 3 as minimal, 4 - 5 as moderate and 6 - 8 as severe fibrosis. Grading was performed by a single investigator in a blinded fashion. 2.5. Analysis of Collagen Content in the Lung Total lung collagen content was determined using the Sircol collagen assay (Biocolor Ltd., Belfast, United Kingdom) according to the manufacturer's instructions. 2.6. Measurement of Cytokine and PGF2 Levels in the Lung The levels of TGF- 1, CCL2, and IL-6 in BAL fluid were measured using ELISA (R&D Systems, Minneapolis, MN) following the manufacturer’s instruction. PGF2 Copyright © 2013 SciRes. OJRD  K. MIYAMOTO ET AL. 33 level was measured with EIA (Cayman Chemical, Ann Arbor, MI). 2.7. Isolation of Mouse Lung Fibroblasts Lungs from untreated mice were digested for 45 min at 37˚C in RPMI with 0.28 U/mL liberase blendzyme 3 and 60 U/ml DNase I, passed through a 70 m filter, centri- fuged at 540 × g at 4˚C, and plated in tissue culture flasks in Dulbecco’s modified Eagle’s medium (DMEM) with 15% fetal bovine serum (FBS). Cells were passaged when subconfluent after harvest with trypsin-EDTA. Cells were used for experiments at passages 3 and 4. 2.8. Cell Proliferation Assay The effect of PPAR- agonists on cell proliferation was assessed by an MTT assay. MLFs (2 × 103/100L) were seeded into the 96-well culture plates and incubated until they reached subconfluence. Thereafter, cells were washed with PBS, and original medium was replaced with medium containing no FBS. MLFs were cultured for another 24 h until treatment with 10% FBS in se- rum-free medium in the presence of RGZ or TS for 24 and 48 hours; MTT (0.5 mg/mL) was added in the last 3 hours. After the removal of the medium and the addition of DMSO to the flask, the absorbance at 570 nm was measured by use of a microplate reader in controls. 2.9. Statistical Analysis Data are reported as mean ± SEM. Differences among groups were determined using analysis of variance fol- lowed by post hoc analysis with the Bonferroni’s test for multiple comparisons. A p value less than 0.05 was con- sidered statistically significant. 3. Results 3.1. Inflammatory Cell Accumulation in the Airspace after Bleomycin Administration To examine the effect of PPAR- ligands on BLM-in- duced accumulation of inflammatory cells, we examined the number of inflammatory cells in BAL fluid obtained on days 2, 7, 14, and 21 (Figure 1). Intratracheal BLM significantly increased the cell count in BAL fluid on day 2, compared with the control mice that received PBS instillation (p < 0.05). Further accumulation of inflam- matory cells occurred on days 7, 14, and 21. Either RGZ or TS significantly suppressed the BLM-induced cell accumulation on days 7, 14, and 21 as compared with the mice without a PPAR- ligand (p < 0.05). 3.2. Lung Histopathology Since the most prominent accumulation of inflammatory Figure 1. Cell counts in BAL fluid after the intratracheal instillation of PBS or BLM. The BLM challenge induced significant increases in the cell counts on day 2 and later compared with the control mice that received PBS. In the groups treated with TS (gray column) or RGZ (closed col- umn), the BLM-induced increases in the cell counts were significantly attenuated compared with those without a PPAR- agonist (open column). All values are expressed as the mean SE (n = 6). *p < 0.05 was considered to be sig- nificantly different from the corresponding value of the control mice with PBS instillation. †p < 0.05 was considered to be significantly different from the corresponding value of the mice that received BLM alone. cells into the airspace was observed on day 7 and later, we evaluated lung pathology using the H-E stained sam- ples obtained on day 7. Representative microscopic find- ings are shown in Figure 2. Compared with the control mice, the BLM administration induced marked hemor- rhages and congestion with infiltration of inflammatory cells, which were ameliorated by the treatment with ei- ther RGZ or TS. To examine the effect of PPAR- agonists on BLM- induced fibrotic changes, lung pathology on day 21 were evaluated. Representative microscopic findings after Masson’s trichrome staining are shown in Figure 3. In the animals without a PPAR- agonist treatment, the BLM administration caused marked thickening of the alveolar septa and infiltration predominated by mononu- clear cells with significant collagen expression. In the mice treated with TS or RGZ, these pathological changes induced by intratracheal BLM were significantly miti- gated. The Ashcroft sores for more quantitative assessment of the lung fibrotic changes were shown in Figure 4. On day 7 and later, the scores were significantly higher in the mice treated with BLM than in those with PBS (p < 0.05). On days 14 and 21, the treatment with either TS or RGZ significantly attenuated the BLM-induced increases in the score compared with the group without a PPAR- agonist (p < 0.05). 3.3. Collagen Contents in the Lung The lungs harvested on day 2, 7, 14, or 21 were analyzed Copyright © 2013 SciRes. OJRD  K. MIYAMOTO ET AL. 34 Figure 2. Representative examples of lung pathology 7 days after the instillation of PBS or BLM. Hematoxylin-eosin stain. Original magnification ×200. Bars, 50 m. n = 6 in each group. Twenty fields were examined per section. Figure 3. Representative examples of lung pathology 21 days after the instillation of PBS or BLM. Masson’s trichrome stain. Original magnification ×200. Bars, 50 m. n = 6 in each group. Twenty fields were examined per sec- tion. for collagen content (Figure 5). In the mice without a PPAR- agonist, intratracheal BLM caused significant increases in the collagen content of the lungs on days 14 and 21, compared with those administered with PBS (p < 0.05). On day 21, the collagen content in the lungs was significantly less in the groups treated with TS or RGZ than in those without administration of a PPAR- ligand (p < 0.05). 3.4. Levels of Profibrotic Cytokines in the Lung To validate the effect of PPAR- agonists on BLM-in- duced upregulation of the cytokines associated with fi- brosis, the levels of TGF- 1, CCL2/MCP-1, and IL-6 were measured in BAL fluid with ELISA. On days 7 and 14, the TGF- 1 levels in the lung were significantly increased in the BLM-treated mice (Figure 6(a)). Whereas the increase in the TGF- 1 level on days Figure 4. The Ashcroft sores for quantitative assessment of the lung fibrotic changes after the intratracheal instillation of PBS or BLM. In the BLM-treated mice, the scores on days 7, 14, and 21 were significantly higher than in the con- trol mice with PBS instillation. In the groups treated with TS (gray column) or RGZ (closed column), the BLM-in- duced increases in the score were significantly suppressed on days 14 and 21 as compared with those without treat- ment with a PPAR- agonist (open column). All values are expressed as the mean SE (n = 6). *p < 0.05 was consid- ered to be significantly different from the corresponding value of the control mice with PBS instillation. †p < 0.05 was considered to be significantly different from the corre- sponding value of the mice administered BLM alone. Figure 5. Collagen contents in the lung after the instillation of PBS or BLM. Intratracheal BLM caused significant in- crease in the collagen content in the lungs. In the groups treated with TS (gray column) or RGZ (closed column), the BLM-induced increase in the collagen content was signifi- cantly suppressed on day 21 as compared with those with- out a PPAR- agonist (open column). All values are ex- pressed as the mean SE (n = 6). *p < 0.05 was considered to be significantly different from the corresponding value of the control mice with PBS instillation. †p < 0.05 was consid- ered to be significantly different from the corresponding value of the mice that received BLM alone. 7 and 14 was significantly suppressed by RGZ (p < 0.05), there were no significant differences in the TGF- 1 levels between the TS-treated mice and those without treatment with a PPAR- agonist. In the animals without a PPAR- agonist, the levels of CCL2 in BAL fluid were significantly elevated 2 and 7 days after the BLM challenge (Figure 6(b)). In the RGZ-treated animals, the BLM-induced elevation of the Copyright © 2013 SciRes. OJRD  K. MIYAMOTO ET AL. Copyright © 2013 SciRes. OJRD 35 3.6. Proliferation of Lung Fibroblast CCL2 level was significantly suppressed on day 2 (p < 0.05). The levels of CCL2 were not different between the TS-treated mice and those without a PPAR- agonist at any time point. The number of MLFs was higher, by 1.51- and 0.97-fold with 10% FBS incubation after 24 and 48 h, respectively, than in controls (p < 0.01) (Figure 7). At 24 h, 10 or 20 mol/L of TS significantly suppressed the proliferation of MLFs, which was induced by 10% FBS alone (p < 0.05) (Figure 7(a)). Although 5 mol/L of RGZ made no change in the MLF number, 10 or 20 mol/L of RGZ significantly decreased the cell number at 24 h, compared with FBS alone (p < 0.05). At 48 h, whereas 5 mol/L of TS made no change in the proliferation of MLFs, 10 or 20 mol/L of RGZ significantly reduced the number of MLFs, compared with FBS alone (p < 0.05) (Figure 7(b)). After co-incubation with FBS and 10 or 20 mol/L of RGZ for 48 h, the number of MLFs was lower than in the FBS alone (p < 0.05). The BLM challenge significantly elevated the levels of IL-6 in the lung 2, 7, or 14 days after the intratracheal challenge (Figure 6(c)). Whereas the increases in the IL-6 levels on days 2, 7, and 14 were significantly sup- pressed by RGZ (p < 0.05), there was no significant dif- ference in the IL-6 levels between the TS-treated mice and those without administration of a PPAR- agonist. 3.5. PGF2 Levels in the Lung Since the levels of the profibrotic cytokines were not changed by TS, the level of PGF2 , a lipid mediator, was measured in BAL fluid with EIA (Figure 6(d)). The in- creases in the PGF2 levels on days 2, 7, and 14 were significantly suppressed by TS (p < 0.05), whereas there was no significant difference in the PGF2 level between the RGZ-treated mice and those without treatment with a PPAR- agonist. 4. Discussion In the present study, it was found that two PPAR- ligands, RGZ and TS, attenuated the BLM-induced in- flammatory and fibrotic changes of the lung. The BLM- (a) (b) (c) (d) Figur e 6. Le vels of TG F- 1, CCL2, IL-6, and PGF2 in BAL fluid. (a) TGF- 1 levels were elevated 7, 14, and 21 days after the BLM challenge, which was significantly attenuated by treatment with RGZ; (b) CCL2 level in the lung was elevated 2 and 7 days after the BLM challenge. The treatment with RGZ significantly suppressed the increase on day 2; (c) IL-6 levels were elevated 7, 14, and 21 days after the BLM challenge, which was significantly attenuated by the treatment with RGZ; (d) PGF2 levels were elevated on days 2, 7, and 14 after the BLM challenge, which was significantly suppressed by treatment with TS. All values are expressed as the mean SE (n = 6). Open, gray, and closed columns indicate mice without treatment with a PPAR- agonist, those treated with TS, and those treated with RGZ, respectively. *p < 0.05 was considered to be sig- nificantly different from the corresponding value of the control mice with PBS instillation. †p < 0.05 was considered to be ignificantly different from the corresponding value of the mice administered BLM alone. s  K. MIYAMOTO ET AL. 36 (a) (b) Figure 7. Effect of RSG and TS on proliferation of lung kines im induced EMT contributes to the de novo appearance of myofibroblasts in the lung. We considered that, in the fibroblast. (a) At 24 h, 10 or 20 mol/L of TS or RGZ sig- nificantly suppressed proliferation of lung fibroblast; (b) After incubation with 10 or 20 mol/L of TS or RGZ for 48 h, the number of murine lung fibroblast was lower than in the FBS alone. All values are expressed as the mean SE. *p < 0.05 was considered to be significantly different from the corresponding value of the FBS contro l. duced increases in the levels of profibrotic cytoin TGF- 1, CCL2, and IL-6 were suppressed by the admini- stration of RGZ. In the TS-treated mice, whereas the lev- els of these cytokines were not changed, the elevation of PGF2 , a lipid mediator associated with fibrosis, after the BLM challenge was attenuated. These results might in- dicate protective effects of PPAR- ligands against the development of lung fibrosis through suppression of cy- tokines or a lipid mediator associated with fibrosis. Among the cytokines and chemokines that have been plicated in the pathogenesis of BLM toxicity, particu- lar relevance has been given to TGF- 1 [16]. In this study, we observed that the RGZ treatment attenuated the BLM-induced increase in TGF-β1 in the lung, which is comparable with the results of previous studies [22,23]. Recently, Tan and coworkers showed that RGZ sup- pressed TGF-β1-induced upregulation of E-cadherin, suggesting the inhibition of epithelial mesenchymal tran- sition (EMT) by activation of PPAR- [24]. TGF-β1- animals treated with RGZ, the suppression of TGF-β1 production might be critical for the attenuation of the BLM-induced lung fibrosis. In addition to TGF- 1, a relative contribution to lung fibrosis of members of the CC chemokines, such as monocyte chemotactic protein-1 (MCP-1/CCL2), has been proposed [17,25]. In this study, CCL2 was elevated in the lung 2 days after the BLM challenge, and it is sig- nificantly fallen by day 14. CCL2, a chemokine respon- sible for mononuclear cell recruitment, is secreted by a variety of cell types such as lymphocytes, macrophages, fibroblasts, and endothelial cells [17]. We considered that, in the RGZ-treated mice, the decreased release of CCL2 might contribute not only to the attenuation of lung fi- brosis but also to the suppression of inflammatory cell accumulation. In a previous report, Genovese and colleagues demon- strated that administration of RGZ reduced mortality rate, accumulation of inflammatory cells in the alveolar com- partment, edema formation, and histological evidence of BLM-induced lung injury [12]. Since our study was fo- cused on the effect of PPAR- agonists on lung fibrosis, the parameters of our study are different from those of theirs. Although the dose of BLM was similar, the sur- vival rate was different between our study and theirs. In the study by Genovese and colleagues, 50% of the BLM- treated mice that had received vehicle died within 15 days [12]. In contrast, none of the animals died during the observation period in our study. We considered that this discrepancy might be due to the difference in the mouse strain and the way of drug administration. In our study, a Microsprayer was used so that the drug solution could be distributed homogenously in the lungs. In the present study, we observed that the levels of profibrotic cytokines in BAL fluid were not affected by TS. It was previously reported that treatment of cultured alveolar epithelial cells with TS reduces TGF- 1-induced collagen I production and cell migration [26]. We there- fore hypothesized that the inhibitory effect of TS might be mediated by other profibrotic mediator and examined the levels of PGF2 in the lungs. PGF2 , is a lipid media- tor, which has been shown to promote BLM-induced lung fibrosis independently of TGF- 1 [20]. We found that the treatment with TS significantly suppressed the BLM-induced increase in PGF2 . Oga and colleagues reported that PGF2 is abundant in BAL fluid of patients with idiopathic pulmonary fibrosis and stimulates prolif- eration and collagen production of lung fibroblasts [20]. We speculated that the inhibitory effect of TS on the BLM-induced fibrosis might be mediated by suppression of PGF2 rather than profibrotic cytokines such as TGF- 1. TS was originally developed as an ARB. Although Copyright © 2013 SciRes. OJRD  K. MIYAMOTO ET AL. 37 some ARBs have PPAR- agonist activity, the agonistic PPAR- effect of TS is known to be greater than that of ther oARBs [27]. Benson and coworkers tested several A ed in some cell types. Benson and coworkers sh - -catenin an creases in pr NCES sensus e European Respiratory Society (ERS),” American Journal of Respiratorycine, Vol. 161, No. RBs for their capacity to activate the expression of PPAR- target genes and found that, at physiological condition, only TS induced a substantial response [27]. On the other hand, renin-angiotensin system is associated with pathogenesis of experimental lung fibrosis. It was reported that intratracheal BLM induced overexpression of angiotensin II type 1 receptor in inflammatory im- mune cells, alveolar type II cells, and fibroblasts [15]. In addition, administration of an angiotensin-converting enzyme inhibitor ramipril reduced collagen deposition after BLM challenge [28]. It remains to be determined whether the antifibrotic effect of TS is through activation of PPAR- pathway or blockade of renin-angiotensin system. In this study, FBS-induced proliferation of MLFs was attenuated by higher concentrations of RGZ and TS. The antiproliferative effects of PPAR- agonists have been demonstrat owed that TS inhibited proliferation of cardiac fibro- blast in a dose-dependent fashion [29]. In addition, Lin and colleagues reported that RGZ treatment inhibits FBS-induced proliferation of cultured human lung fibro- blast [30]. We considered that antiproliferative effects of PPAR- agonists on lung fibroblast might be associated with the attenuation of BLM-induced fibrosis. The molecular mechanisms underlying the antifibrotic effects of PPAR- are the subject of intense investigation. In fibroblasts, ligand-activated PPAR- blocks profi- brotic signaling triggered by TGF- 1 and Wnt d interferes with downstream signal transduction [31, 32]. In this study, we observed reduction of TGF- 1 lev- els in the lung by RGZ as well as suppression of PGF2α by TS. Xu and coworkers showed that stimulation of the human FP prostanoid receptor with PGF2α induces se- quential activation of Ras and Raf kinases, followed by Tcf transcriptional activation [33]. Since Tcf forms a complex with -catenin to activate transcription of Wnt, we speculated that TS-induced suppression of PGF2α might be a key mechanism of its protective effect. The effect of PPAR- ligands on these signaling cascades should be the subject of further investigation. In conclusion, two PPAR- ligands, RGZ and TS, ex- ert protective effects on BLM-induced lung fibrosis pos- sibly through suppression of different profibrotic media- tors. RGZ suppressed the BLM-induced in ofibrotic cytokines, TGF-β, MCP-1, and IL-6, whereas TS mitigated the increases in PGF2 in the lung. Al- though its efficacy remains to be evaluated in a more clinically relevant model, a PPAR- modulator could be considered as a candidate of a therapeutic modality for noninfectious lung injury and subsequent fibrotic changes. 5. Acknowledgements The authors thank Dr. Tomomi Ueda and Ms. Miyuki Yamamoto for their excellent technical assistance. REFERE [1] American Thoracic Society, “Idiopathic Pulmonary Fi- brosis: Diagnosis and Treatment. International Con Statement. American Thoracic Society (ATS), and th and Critical Care Medi 2, 2000, pp. 646-664. doi:10.1164/ajrccm.161.2.ats3-00 [2] A. Moeller, K. Ask, D. Warburton, et al., “The Bleomy- cin Animal Model: A Useful Tool to Investigate Treat- ment Options for Idiopathic Pulmonary Fibrosis?” Inter- national Journal of Biochemistry and Cell Biology, Vol. 40, No. 3, 2008, pp. 362-382. doi:10.1016/j.biocel.2007.08.011 [3] D. H. Bowden, “Unraveling Pulmonary Fibrosis: The Bleomycin Model,” Laboratory Investigation, Vol. 50, No. 5, 1984, pp. 487-488. [4] C. Agostini and C. Gurrieri, “C tail in Idiopathic Pulmonary Fibro hemokine/Cytokine Cock- sis,” Proceedings of the American Thoracic Society, Vol. 3, No. 4, 2006, pp. 357- 363. doi:10.1513/pats.200601-010TK [5] R. L. Riha, I. A. Yang, G. C. Rabnott, et al., “Cytokine Gene Polymorphisms in Idiopathic Pulmonary Fibrosis,” Internal Medicine Journal, Vol. 34, No. 3, 2004, pp. 126- 129. doi:10.1111/j.1444-0903.2004.00503.x [6] Y. Wang, J. Santos, R. Sakurai, et al., “Peroxisome Pro- liferator-Activated Receptor Gamma Agonists Enhance Lung Maturation in a Neonatal Rat Model,” Pediatric Research, Vol. 65, No. 2, 2009, pp. 150-155. doi:10.1203/PDR.0b013e3181938c40 [7] T. J. Standiford, V. G. Keshamouni and R. C. Reddy, “Peroxisome Proliferator-Activated Receptor- as a Regu- lator of Lung Inflammation and Repair,” Proceedings of the American Thoracic Society, Vol. 2, No. 3, 2005, pp. 226-231. doi:10.1513/pats.200501-010AC [8] M. Ricote, A. C. Li, T. M. Willson, et al., “The Perox- isome Proliferator-Activated Receptor-Gamma Is a Nega- tive Regulator of Macrophage Activation,” Nature, Vol. 391, No. 6662, 1998, pp. 79-82. doi:10.1038/34178 [9] K. Asada, S. Sasaki, T. Suda, et al., “Antiinflammatory Roles of Peroxisome Proliferators-Activated Receptor Gamma in Human Alveolar Macrophages,” American Journal of Respiratory and Critical Care Medicine, Vol. 169, No. 2, 2004, pp. 195-200. doi:10.1164/rccm.200207-740OC [10] R. A. Daynes and D. C. Jones, “Emerging Roles of PPARs in Inflammation and Immunity,” Nature Reviews Immunology, Vol. 2, No. 10, 2002, pp. 748-759. doi:10.1038/nri912 [11] J. M. Lehmann, L. B. Moore, T. A. Smith-Oliver, et al., “An Antidiabetic Thiazolidinedione Is a High Affinity Ligand for Peroxisome Proliferator-Activated Receptor (PPAR- ),” Journal of Biological Chemistry, Vol. 270, Copyright © 2013 SciRes. OJRD  K. MIYAMOTO ET AL. Copyright © 2013 SciRes. OJRD 38 22.12953 No. 22, 1995, pp. 12953-12956. doi:10.1074/jbc.270. 4 [12] T. Genovese, S. Cuzzocrea, R. Di Paola, et al., “Effect of Rosiglitazone and 15-Deoxy-12,14-Prostaglandin J2 on Bleomycin-Induced Lung Injury,” European Respiratory Journal, Vol. 25, No. 2, 2005, pp. 225-234. doi:10.1183/09031936.05.0004970 oriyama, et al., “A Selec-[13] T. Tagami, H. Yamamoto, K. M tive Peroxisome Proliferator-Activated Receptor-Gamma Modulator, Telmisartan, Binds to the Receptor in a Dif- ferent Fashion from Thiazolidinediones,” Endocrinology, Vol. 150, No. 2, 2009, pp. 862-870. doi:10.1210/en.2008-0502 [14] M. Schupp, J. Janke, R. Clasen, et al., “Angiotensin Type 1 Receptor Blockers Induce Peroxisome Proliferator-Ac- tivated Receptor-Gamma Activity,” Circulation, Vol. 109, No. 17, 2004, pp. 2054-2057. doi:10.1161/01.CIR.0000127955.36250.65 . Shiratori, et al., “Reduction[15] M. Otsuka, H. Takahashi, M of Bleomycin Induced Lung Fibrosis by Candesartan Cilexetil, an Angiotensin II Type 1 Receptor Antagonist,” Thorax, Vol. 59, No. 1, 2004, pp. 31-38. doi:10.1136/thx.2003.000893 [16] T. J. Broekelmann, A. H. Limper, T. V. Colby, et al. No. 15, 73/pnas.88.15.6642 , “Transforming Growth Factor 1 is Present at Sites of Extracellular Matrix Gene Expression in Human Pulmo- nary Fibrosis,” Proceedings of the National Academy of Sciences of the United States of America, Vol. 88, 1991, pp. 6642-6646. doi:10.10 logy [17] R. E. Smith, R. M. Strieter, K. Zhang, et al., “A Role for C-C Chemokines in Fibrotic Lung Disease,” Journal of Leukocyte Biology, Vol. 57, No. 5, 1995, pp. 782-787. [18] I. Shahar, E. Fireman, M. Topilsky, et al., “Effect of IL-6 on Alveolar Fibroblast Proliferation in Interstitial Lung Diseases,” Clinical Immunology and Immunopatho, Vol. 79, No. 3, 1996, pp. 244-251. doi:10.1006/clin.1996.0075 [19] F. Saito, S. Tasaka, K. Inoue, et al., “Role of Interleukin- 6 in Bleomycin-Induced Lung Inflammatory Changes in Mice,” American Journal of Respiratory Cell and Mo- lecular Biology, Vol. 38, No. 5, 2008, pp. 566-571. doi:10.1165/rcmb.2007-0299OC [20] T. Oga, T. Matsuoka, C. Yao, et al., “Prostaglandin F2 Receptor Signaling Facilitates Bleomycin-Induced Pul- monary Fibrosis Independently of Transforming Growth Factor- ,” Nature Medicine, Vol. 15, No. 12, 2009, pp. 1426-1430. doi:10.1038/nm.2066 [21] T. Ashcroft, J. M. Simpson and V. Timbrell, “Simple Method of Estimating Severity of Pulmonary Fibrosis on a Numerical Scale,” Journal of Clinical Pathology, Vol. 41, No. 4, 1988, pp. 467-470. doi:10.1136/jcp.41.4.467 [22] K. Zhang, K. C. Flanders and S. H. Phan, “Cellular Lo- calization of Transforming Growth Factor-Beta Expres- r- ,” Expimental Lung Research, Vol. 28, No. 3, 2002, sion in Bleomycin-Induced Pulmonary Fibrosis,” Ameri- can Journal of Pathology, Vol. 147, No. 2, 1995, pp. 352- 361. [23] N. Khalil, T. V. Parekh, R. N. O’Connor, et al., “Diffe ential Expression of Transforming Growth Factor-Beta Type I and II Receptors by Pulmonary Cells in Bleomy- cin-Induced Lung Injury: Correlation with Repair and Fi- brosis pp. 233-250. doi:10.1080/019021402753570527 [24] X. Tan, H. Dagher, C. A. Hutton, et al., “Effects of PPAR Gamma Ligands on TGF- 1-Induced Epithelial-Mesen- chymal Transition in Alveolar Epithelial Cells,” Respira- tory Research, Vol. 11, 2010, p. 21. doi:10.1186/1465-9921-11-21 [25] K. Zhang, M. Gharaee-Kermani, M. L. Jones, et al., “Lung monocyte Chemoattractant Protein-1 Gene Expression in Bleomycin-Induced Pulmonary Fibrosis,” Journal of Im- munology, Vol. 153, No. 10, 1994, pp [26] S. T. Buckley, C. Medina and C. Ehrhard . 4733-4741. t, “Differential 2010, Susceptibility to Epithelial-Mesenchymal Transition (EMT) of Alveolar, Bronchial and Intestinal Epithelial Cells in Vitro and the Effect of Angiotensin II Receptor Inhibi- tion,” Cell and Tissue Research, Vol. 342, No. 1, pp. 39-51. doi:10.1007/s00441-010-1029-x [27] S. C. Benson, H. A. Pershadsingh, C. I. Ho, et al., “Iden- tification of Telmisartan as a Unique Angiotensin Ii Re- ceptor Antagonist with Selective PPAR Gamma-Modu- lating Activity,” Hypertension, Vol. 43, No. 5, 2004, pp. 993-1002. doi:10.1161/01.HYP.0000123072.34629.57 [28] R. P. Marshall, P. Gohlke, R. C. Chambers, et al., “An- giotensin II and the Fibroproliferative Response to Acute Lung Injury,” American Journal of Physiology Lung Cel- lular and Molecular Physiology, Vol. 286, No. 1, 2004, pp. L156-L164. doi:10.1152/ajplung.00313.2002 [29] S. C. Benson, R. Iguchi, C. I. Ho, et al., “Inhibition of Cardiovascular Cell Proliferation by Angiotensin Recep- tor Blockers: Are All Molecules the Same?” Journal of Hypertension, Vol. 26, No. 5, 2008, pp. 973-980. doi:10.1097/HJH.0b013e3282f56ba5 [30] Q. Lin, L. P. Fang, W. W. Zhou, et al., “Rosiglitazone Inhibits Migration, Proliferation, and Phenotypic Differ- entiation in Cultured Human Lung Fibroblasts,” Experi- mental Lung Research, Vol. 36, No. 2, 2010, pp. 120-128. doi:10.3109/01902140903214659 [31] A. K. Ghosh, S. Bhattacharyya, G. Lakos, et al., “Disrup- tion of Transforming Growth Factor Signaling and Pro- fibrotic Responses in Normal Skin Fibroblasts by Perox- isome Proliferator-Activated Receptor ,” Arthritis and Rheumatism, Vol. 50, No. 4, 2004, pp. 1305-1318. doi:10.1002/art.20104 [32] D. Lu and D. A. Carson, “Repression of -Catenin Sig- naling by PPAR Ligands,” European Journal of Phar- macology, Vol. 636, No. 1-3, 2010, pp. 198-202. doi:10.1016/j.ejphar.2010.03.010 [33] W. Xu, C. L. Chou, D. D. Israel, et al., “PGF Stimulates ication, . 2 FP Prostanoid Receptor Mediated Crosstalk between Ras/Raf Signaling and Tcf Transcriptional Activation,” Biochemical and Biophysical Research Commun Vol. 381, No. 4, 2009, pp. 625-629 doi:10.1016/j.bbrc.2009.02.102
|