B. ENGMANN
unfit for work at admission
pensioner or othersnoyesMissing
Count
300
200
100
0
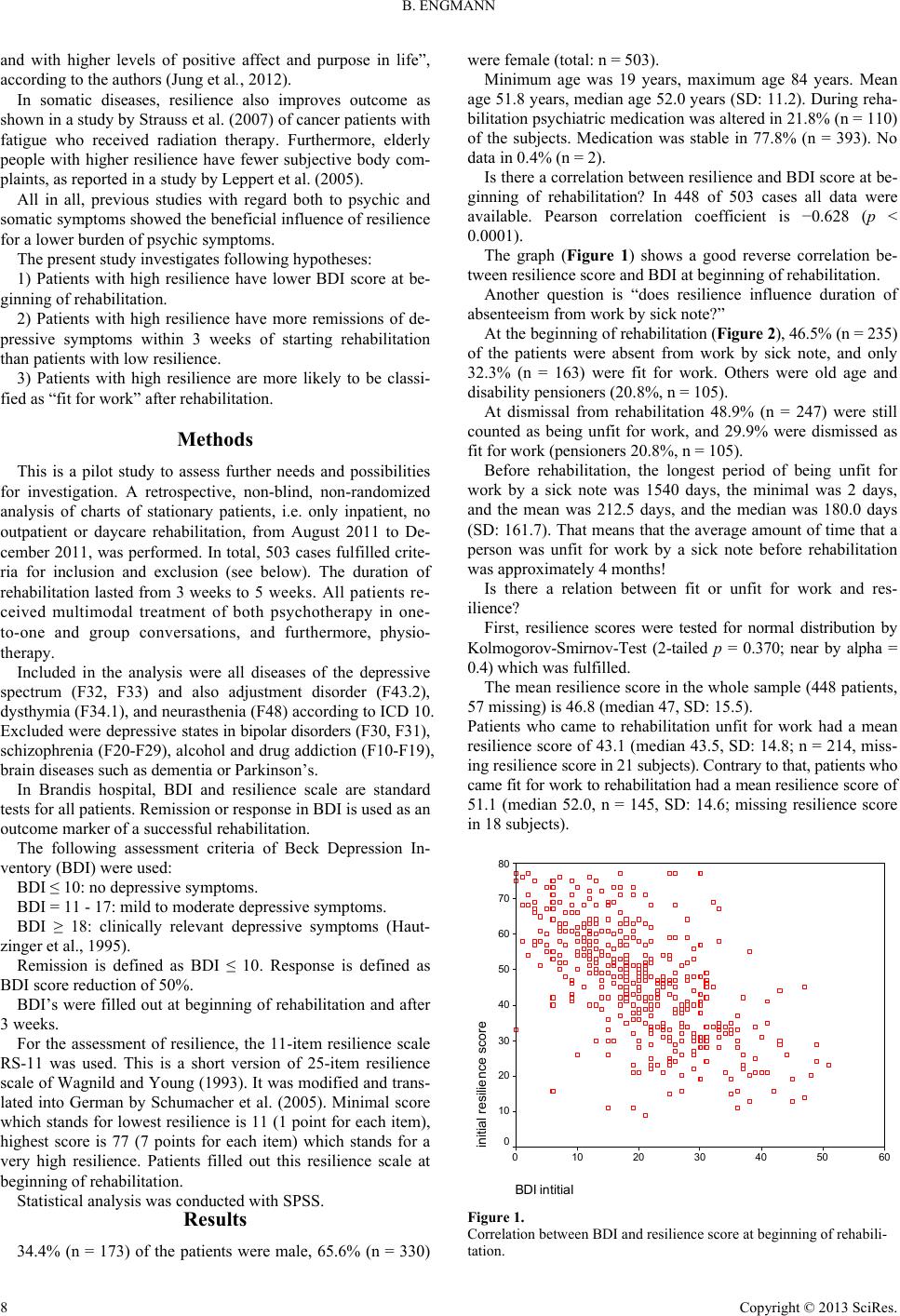
Figure 2.
Status of being fit or unfit for work at the beginning of rehabilitation.
Similar findings exist for dismissal. In patients who were re-
leased unfit for work from rehabilitation mean resilience score
was 42.97 (median 43.0, n = 223, SD: 14.8; missing resilience
score in 14 subjects). Patients who were released fit for work
had a mean resilience score of 51.99 (median 52.50, n = 136,
SD: 14.1; missing resilience score in 15 subjects).
In conclusion, there is a trend that patients who either came
fit for work or left rehabilitation fit for work had higher resil-
ience scores.
Does resilience predict outcome of depressive symptoms?
Patients who had a remission after 3 weeks rehabilitation had
a mean resilience score of 53.56 (median 54.0, SD: 12.3; n = 61,
0 missing).
Patients who had a response but no remission after 3 weeks
rehabilitation had a mean resilience score of 40.11 (median
39.0, n = 17, SD: 7.7; 0 missing).
Patients who had neither remission nor response (“no effort”)
had a mean resilience score of 41.77 (median 42.0, n = 252, SD:
14.4; 4 missing).
In conclusion, a trend could be described that patients with
remission are accompanied by higher resilience compared to
patients with response or “no effort”.
Discussion
The mean resilience score (46.8) in the whole sample is
lower than the medium resilience score of a healthy population
(58.03 according to Schumacher et al., 2005).
The study revealed a good reverse correlation between resil-
ience and BDI. The higher the resilience the lower the BDI
score, indicating a lower burden of depressive symptoms.
Two outcome items were investigated in relation to resilience:
being fit or unfit for work and remission of depressive symp-
toms. There is a trend that patients who either were fit for work
at the beginning of rehabilitation or were dismissed as fit for
work had higher resilience scores that those who were unfit for
work. The same is for patients with higher resilience who were
more likely to have a remission than those with lower resilience.
This finding could only be described as a trend because number
of subjects in subgroups differs to a high degree and thus could
lead to bias.
Patients with depressive disorders in rehabilitation have al-
ready been absent from work approximately 4 months before
the beginning of rehabilitation. This raises a question of when
symptoms may be considered chronic.
It is interesting that there is no major effect of rehabilitation
in relation to whether patients are fit or unfit for work before
and after rehabilitation and the outcome is counterintuitive, in
that there was a slight increase of patients judged unfit for work
after rehabilitation. Perhaps this outcome may be explained by
differences between the physicians responsible for admitting
the patient and the physicians of the rehabilitation clinic, in that
they may have different criteria for being fit for work. Another
question is if different approaches of involved physicians affect
ICD-10 criteria and thus inclusion criteria. Other limitation
factors could be the relatively small sample size, or the severity
of the disease which goes with prolonged absenteeism from
work before rehabilitation. Furthermore the study has no fol-
low-up to assess the duration of absenteeism after dismissal nor
does it contain information about how many patients had been
included in a gradual reintegration program (called “stufen-
weise Wiedereingliederung” or “Hamburg model”) in the old
working place. This program deems one unfit for work until
one achieves a full number of working hours. Such a program
avoids the oversimplification of defining the value of rehabili-
tation entirely by results present at the time of dismissal.
Another factor which weakens the results of the present
study is that psychiatric medications were altered during reha-
bilitation. In addition to it, even cases with no alteration during
rehabilitation could benefit from delayed effects of a medica-
tion which had been started before rehabilitation. Moreover,
patients did not receive a completely “superposable” psycho-
logical and physical treatment. Also, different age groups could
lead to a bias in the study.
In conclusion, the present pilot study encourages further in-
vestigation of the relation of resilience to depressive disorders,
and rehabilitation from them, and reintegration in social life.
Acknowledgements
Professor Dr. Wilfried Mau, Institute of Rehabilitation Me-
dicine, University of Halle, Germany, and Professor Dr. Ger-
hard Schmid-Ott, Berolina Clinic, Bad Oeynhausen, Germany,
for introduction to the topic of resilience.
REFERENCES
Ahmand, S., Feder, A., Lee, E. J., Wang, Y., Southwick, S. M.,
Schlackman, E., Buchholz, K., Alonso, A., & Charney, D. S. (2010).
Earthquake impact in a remote South Asian population: Psychosocial
factors and posttraumatic symptoms. Journal of Traumatic Stress, 23,
408-412.
Cicchetti, D. (2010). Resilience under conditions of extreme stress: A
multilevel perspective. W orld P s y c h i at r y , 9 , 145-154.
Hautzinger, M., Bailer, M., Worall, H., & Keller, F. (1995). Beck-
Depressionis-Inventar (BDI) . Testhandbuch (2nd ed.). Bern: Hans
Huber.
Hjemdal, O., Vogel, P. A., Solem, S., Hagen, K., & Stiles, T. C. (2011).
The relationship between resilience and levels of anxiety, depression,
and obsessive-compulsive symptoms in adolescents. Clinical Psy-
chology & Psychotherapy, 18, 314-321. doi:10.1002/cpp.719
Jung, Y. E., Min, J. A., Shin, A. Y., Han, S. Y., Lee, K. U., Kim, T. S.,
Park, J. E., Choi, S. W., Lee, S. H., Choi, K. S., Park, Y. M., Woo, J.
M., Bhang, S. Y., Kang, E. H., Kim, W., Yu, J. J., & Chae, J. H.
(2012). Positiveness research team of Korea: The Korean version of
the connor-davidson resilience scale: An extended validation. Stress
Copyright © 2013 SciRes. 9