Z. Ozkan et al. / HEALTH 2 (2010) 1294-1298
Copyright © 2010 SciRes. http://www.scirp.org/journal/HEALTH/
1297
Openly accessible at
Radiographs can mostly identify foreign bodies and
free mediastinal or peritoneal air. The lateral projection
confirms location in the esophagus and may reveal the
presence of more than one coin. However, non-metallic
objects are not readily seen. A contrast examination should
not be performed routinely because of the risk of aspira-
tion and coating of the foreign body and esophageal mu-
cosa compromises subsequent endoscopy. If symptoms
are not clear or specific, a cautious contrast study may
be appropriate to clarify the presence of a foreign body
or its location. Computerized tomography may be useful
in some cases. Metal detectors can detect swallowed me-
tallic objects and may be of use as a screening tool espe-
cially in pediatric patients [14]. Persistent symptoms re-
lated to the esophagus in cases of suspected foreign body
ingestion should be pursued with endoscopy even after
an apparently unrevealing radiographic evaluation.
Management of foreign body ingestion is influenced
by many factors such as patient’s age and clinical condi-
tion; size, shape, and classification of the ingested mate-
rial; the anatomic location in which the object is lodged
[15]. The physician should decide whether endoscopic or
surgical intervention is necessary or not, what degree of
urgency is called for, and by what means. In medication,
smooth-muscle relaxation agents such as benzodiazepi-
nes, and nifedipine and those which improve peristaltic
activity such as glucagon and E-Z Gas may be used. But,
there is not convincing evidence in the literature that the
use of such agents changes clinical outcomes [16].
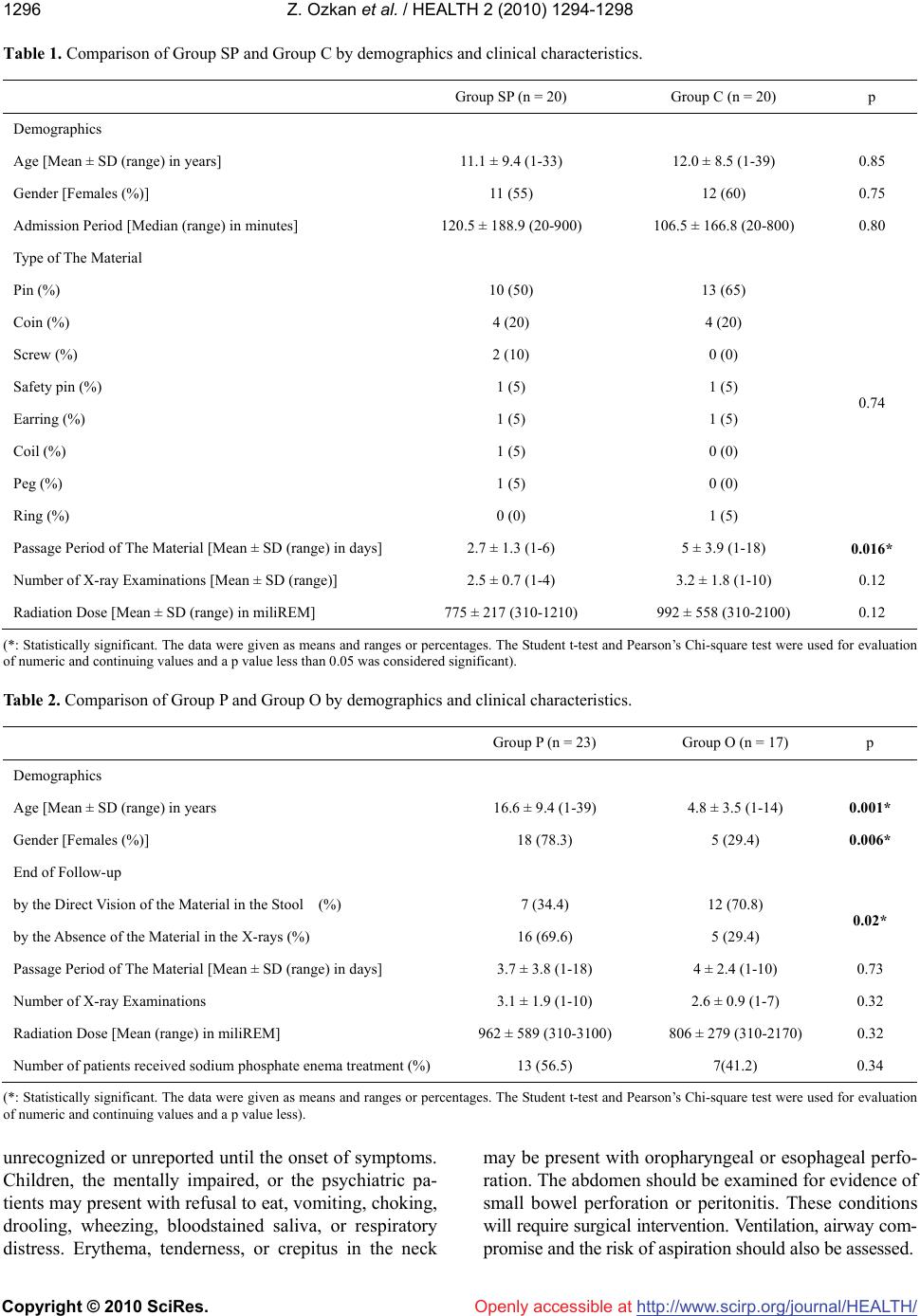
This study is the first to evaluate the effect of sodium
phosphate enema in patients who swallowed foreign ma-
terials. The results of the study indicate that the use of
enema shortens the period between the ingestion and eva-
cuation of the material, however, do not change the num-
ber of necessitated x-rays, or the radiation dose adminis-
trated to the patients. In our opinion, this shortening ef-
fect of enema was due to emptying of the rectum. Rectal
distension with feces produces an inhibitory effect on
jejunal and ileal peristalsis. This effect was termed as
recto-enteric reflex [17]. Rectal emptying by enema de-
creases rectal distension and in this way may inhibit
recto-enteric reflex.
Contrary to the literature, pins were the most com-
monly ingested material in our study, because most of
our patients were young Muslim girls who inadvertently
swallowed turban pins. Also, the proportion of children
was less than the western studies in our study because of
high number of young girls [1-3]. Thus we, retrospec-
tively, compared the characteristics between patients who
ingested pins versus other materials. We have found that
the pin ingestion mostly occurs in turbaned young girls.
Thus, in our opinion, pin ingestion is a completely dif-
ferent entity according to demographic evaluation. This
analysis revealed that direct visualization of the pins in
the stool is difficult, so the defecation of material was
inferred by the absence of pins on abdominal radiographs
in almost two-thirds of the patients in this group. Al-
though radiograph of stool would be an option to avoid
radiation exposure to young girls, daily radiography is
frequently necessary in patients who ingest pin.
5. CONCLUSIONS
Sodium phosphate enemas may be beneficial in pa-
tients who suffer from foreign body ingestion, since it is
completely safe, easy-to-use, well-accepted by the patients,
and it may hasten the pass over period of the materials.
As a subgroup of swallowed foreign materials, pin in-
gestion is more common among turbaned young girls in
our country.
REFERENCES
[1] Paul, R.I., Christoffel, K.K., Binns, H.J., Jaffe, D.M. and
the Pediatric Practice Research Group. (1993) Foreign
body ingestion in children: Risk of complication varies
with site of initial health care contact. Pediatrics, 91(1),
121-127.
[2] Hashmonai, M., Kaufman, T. and Schramek, A. (1978)
Silent perforations of the stomach and duodenum by
needles. Archives of Surgery, 113(12), 1406-1409.
[3] Cheng, W. and Tam, P.K.H. (1999) Foreign-body inges-
tion in children: Experience with 1,265 cases. Journal of
Pediatric Surgery, 34(10), 1472-1476.
[4] Kaptanoglu, M., Dogan, K., Onen, A. and Kunt, N. (1999)
Turban pin aspiration: A potential risk for young Islamic
girls. International Journal of Pediatric Otorhinolaryn-
gology, 48(2), 131-135.
[5] Shabb, B., Taha, A.M., Hamada, F. and Kanj, N. (1996)
Straight pin aspiration in young women. Journal of Trauma,
40(5), 827-828.
[6] Ucan, E.S., Tahaoglu, K., Mogolkoc, N., Dereli, S., Ba-
soz-demir, N., Basok, O., Turktas, H., Akkocoglu, A. and
Ates, M. (1996) Turban pin aspiration syndrome: A new
form of foreign body aspiration. Respiratory Medicine,
90(7), 427-428.
[7] Hodge III, D., Tecklenburg, F. and Fleisher, G. (1985)
Coin ingestion: Does every child need a radiograph? An-
nals of Emergency Medicine, 14(5), 443-446.
[8] Kelley, J.E., Leech, M.H. and Carr, M.G. (1993) A safe
and cost-effective protocol for the management of eso-
phageal coins in children. Journal of Pediatric Surgery,
28(7), 898-900.
[9] Robbins, M.I. and Shortsleeve, M.J. (1994) Treatment of
acute esophageal food impaction with glucagons, an ef-
fervescent agent, and water. American Journal of Roent-
genology, 162, 325-328.
[10] Davies, C. (2004) The use of phosphate enemas in the
treatment of constipation. Nursing Times, 100(18), 32-35.
[11] Webb, W.A. (1995) Management of foreign bodies of the
upper gastrointestinal tract: Update. Gastrointest Endosc,