S. Demura et al. / Advances in Aging Research 2 (2013) 57-64 63
actions such as slips and missteps which require a step-
ping strategy.
5. CONCLUSION
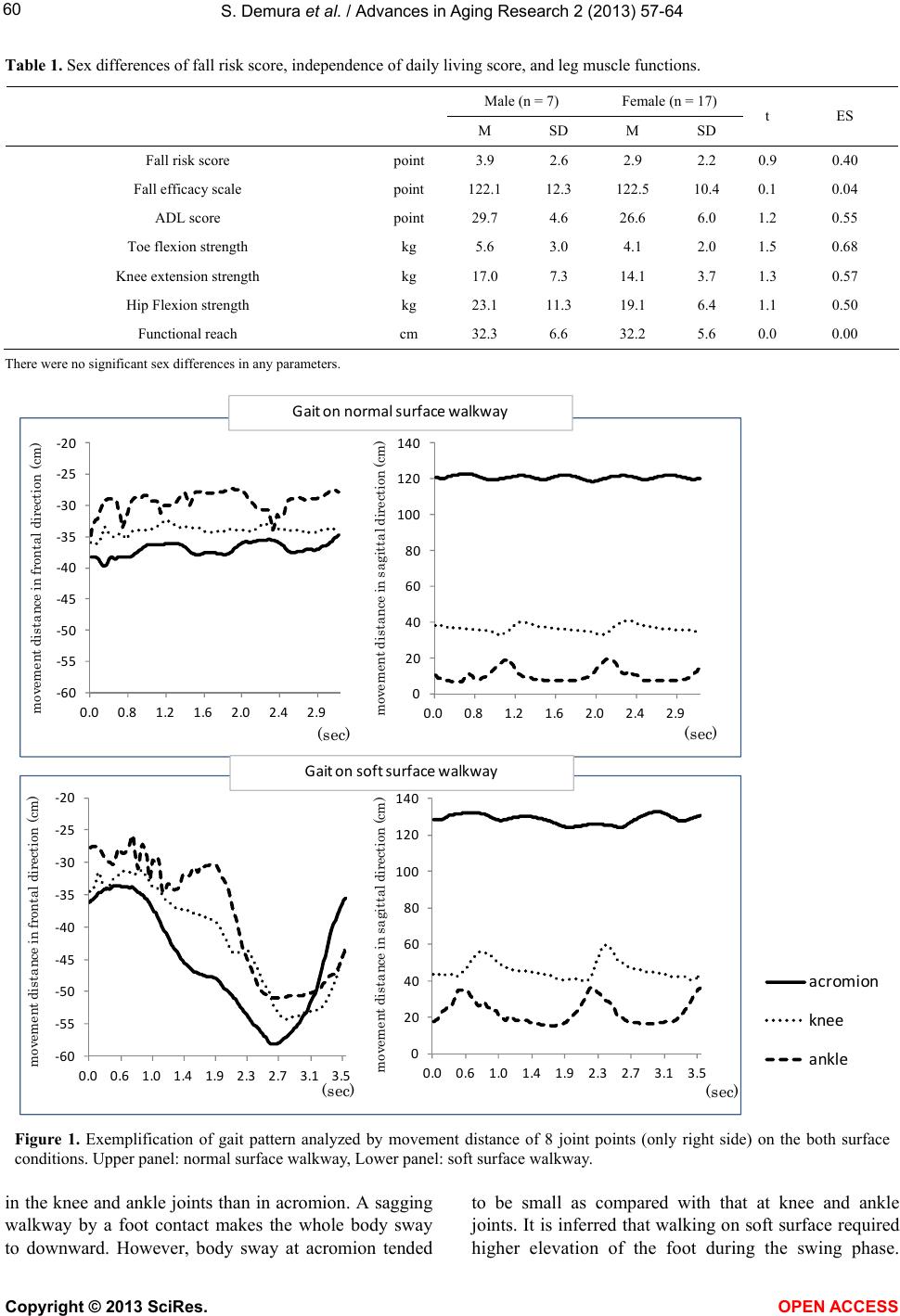
In conclusion, gait properties on soft surfaces which
change the plantar aspect during foot contact differ from
those on a normal surface. Body sway of the acromion in
the frontal direction on a soft surface is larger than that
of knee and ankle joints. Walking on a soft surface may
cause an unanticipated inverted pendulum sway support-
ing a foot contact point because of the disturbance by the
sagging walkway. Gait on the soft surface requires bal-
ance ability (functional reach) rather than leg strength.
REFERENCES
[1] Lord, S.R. and Dayhew, J. (2001) Visual risk factors for
falls in older people. Journal of American Geriatrics So-
ciety, 49, 508-515.
doi:10.1046/j.1532-5415.2001.49107.x
[2] Eke-Okoro, S.T. (2000) A critical point for the onset of
falls in the elderly. A pilot study. Gerontology, 46, 88-92.
doi:10.1159/000022140
[3] Ferrandez, A.M., Pailhous, J. and Durup, M. (1990)
Slowness in elderly gait. Experimental Aging Research,
16, 79-89. doi:10.1080/07340669008251531
[4] Suzuki, T. (2003) Epidemiology and implications of fal-
ling among the elderly. Nippon Ronen Igakkai Zasshi, 40,
85-94. doi:10.3143/geriatrics.40.85
[5] Van der Velde, N., Stricker, B.H., Pols, H.A. and van der
Cammen, T.J. (2007) Withdrawal of fall-risk-increasing
drugs in older persons: Effect on mobility test outcomes.
Drugs and Aging, 24, 691-699.
doi:10.2165/00002512-200724080-00006
[6] Graham, R.C., Smith, N.M. and White, C.M. (2005) The
reliability and validity of the physiological cost index in
healthy subjects while walking on 2 different tracks. Ar-
chives of Physical Medicine and Rehabilitation, 86, 2041-
2046. doi:10.1016/j.apmr.2005.04.022
[7] Podsiadlo, D. and Richardson, S. (1991) The timed “Up
& Go”: A test of basic functional mobility for frail elderly
persons. Journal of American Geriatrics Society, 39, 142-
148.
[8] Gill, J., Allum, J.H., Carpenter, M.G., Held-Ziolkowska,
M., Adkin, A.L., Honegger, F. and Pierchala K. (2001)
Trunk sway measures of postural stability during clinical
balance tests: Effects of age. The Journals of Gerontology:
Series A, 56, M438-M447.
doi:10.1093/gerona/56.7.M438
[9] Means, K.M. (1996) The obstacle course: A tool for the
assessment of functional balance and mobility in the eld-
erly. Journal of Rehabilitation Research and Develop-
ment, 33, 413-429.
[10] Rubenstein, L.Z., Josephson, K.R., Trueblood, P.R., Ye-
ung, K. and Harker, J.O. (1997) The reliability and valid-
ity of an obstacle course as a measure of gait and balance
in older adults. Aging, 9, 127-135.
[11] Kerrigan, D.C., Lee, L.W., Nieto, T.J., Markman, J.D.,
Collins, J.J. and Riley, P.O. (2000) Kinetic alterations in-
dependent of walking speed in elderly fallers. Archives of
Physical Medicine and Rehabilitation, 81, 730-735.
doi:10.1016/S0003-9993(00)90101-1
[12] Suzuki, T. (2000) Questionnaire for falls assessment of
elderly people and its application. Health Assessment
Manual. Kosei Kagaku Kenkyusho, Tokyo, 142-163.
[13] Hellstrom, K. and Lindmark, B. (1999) Fear of falling in
patients with stroke: A reliability study. Clinical Reha-
bilitation, 13, 509-517.
doi:10.1191/026921599677784567
[14] Ministry of Education, Culture, Sports, Science and Tech-
nology (1999) Guideline for new physical fitness test.
http://www.mext.go.jp/a_menu/sports/stamina/03040901.
htm
[15] Demura, S. and Yamada, T. (2007) Simple and easy ass-
essment of falling risk in the elderly by functional reach
test using elastic stick. Tohoku Journal of Experimental
Medicine, 213, 105-111. doi:10.1620/tjem.213.105
[16] Takenaka, K. and Uechi, H. (2002) Development of fal-
ling self-efficacy scale for elderly people: The reliability
and validity. Japan Journal of Physical Education, Hea-
lth and Sport Sciences, 47, 1-13.
[17] Yasumura, S., Haga, H., Nagai, H., Shibata, H., Iwasaki,
K., Ogawa, Y., Ahiko, T., Ihara, K. and Sakihara, S. (1994)
Risk factors for falls among the elderly living in a Japa-
nese rural community. Nippon Koshu Eisei Zasshi, 41,
528-537.
[18] Campbell, A.J., Spears, G.F. and Borrie, M.J. (1990) Ex-
amination by logistic regression modelling of the vari-
ables which increase the relative risk of elderly women
falling compared to elderly men. Journal of Clinical Epi-
demiology, 43, 1415-1420.
doi:10.1016/0895-4356(90)90110-B
[19] Yasumura, S., Haga, H., Nagai, H., Suzuki, T., Amano, H.
and Shibata, H. (1994) Rate of falls and the correlates
among elderly people living in an urban community in
Japan. Age Aging, 23, 323-327.
doi:10.1093/ageing/23.4.323
[20] Yasumura, S., Haga, H., Nagai, H., Shibata, H., Iwasaki,
K., Ogawa, Y., Ahiko, T. and Ihara, K. (1991) Incidence
of and circumstances related to falls among the elderly in
a Japanese community. Nippon Koshu Eisei Zasshi, 38,
735-742.
[21] Potter, J.M., Evans, A.L. and Duncan, G. (1995) Gait
speed and activities of daily living function in geriatric
patients. Archives of Physical Medicine and Rehabilita-
tion, 76, 997-999. doi:10.1016/S0003-9993(95)81036-6
[22] Means, K.M. and O’Sullivan, P.S. (2000) Modifying a
functional obstacle course to test balance and mobility in
the community. Journal of Rehabilitation Research and
Development, 37, 621-632.
[23] Shin, S. and Demura, S. (2011) Different step-over move-
ment strategies for disturbance stimulations. Perceptual
and Motor Skills, 113, 11-18.
doi:10.2466/25.26.PMS.113.4.11-18
[24] Clark, S., Iltis, P.W., Anthony, C.J. and Toews, A. (2005)
Copyright © 2013 SciRes. OPEN ACCESS