Paper Menu >>
Journal Menu >>
 Surgical Science, 2010, 1, 31-39 doi:10.4236/ss.2010.12007 Published Online October 2010 (http://www.SciRP.org/journal/ss) Copyright © 2010 SciRes. SS Basic Experimental Pancreatitis Models for Beginners Baris D. Yildiz1, Erhan Hamaloglu2 1Ankara Numune Teaching Hospital 6th General Surgery, Ankara,Turkey 2Hacettepe University Faculty of Medicine General Surgery Department, Sihhiye, Turkey E-mail: baris104@yahoo.com, barisy@hacettepe.edu.tr Received July 6, 2010; revised August 3, 2010; accepted August 10, 2010 Abstract Efforts to find an ideal model for pancreatitis date back to 1960’s. Many models are suggested since then. Every model has its own advantages and disadvantages. Some of these models test etiology while others simulate the complications of pancreatitis. An ideal model which by itself demonstrates all aspects of pan- creatitis including systemic changes is yet to be described. In this review we tried to gather the basic, easy to construct models. Keywords: Pancreatitis, Experimental Models, Closed Duodenal Loop, Arginine Induced, Ex Vivo Perfusion Model, Duct Obstruction, Taurocholate Injection, Vascular Induced 1. Introduction Acute pancreatitis (AP) is inflammation of pancreatic tissue which can present in a wide spectrum ranging from edema of the organ to necrosis and hemorrhage. Acute pancreatitis is a multi-etiology disease with con- troversial physiopathology. Thus, it has an unpredictable course without a targeted treatment [1] which results in high morbidity and mortality. In the clinical setting gallstone obstruction is the most common cause (30%-50%) of AP. Alcoholism is the second most common cause and recurrent alcoholic AP leads to chronic pancreatitis. Infection, autoimmune re- sponse, trauma, hyperlipidemia, hyperparathyroidism account for nearly 10% of AP cases [2]. There are many experimental studies which try to ide- ntify the pathogenesis and treatment options for pan- creatitis. In this review we tried to evaluate the differ- ences between models and the particular methodologies of each experimental model with outline of evolution of each technique. 2. Closed Duodenal Loop (CDL) Induced Pancreatitis In physiological conditions there is a pressure difference between pancreatic duct (PD), sphincter of Oddi and duodenum. This prevents duodenopancreatic reflux. CDL, by violating this normal state, increases intraduo- denal luminal pressure causing reflux of duodenal fluid to PD causing pancreatitis. Closed loop is constructed with duodenum surrounding the opening of the PD. This model was first described by Seidel and popular- ized later by Pfeffer [1]. The first species used were dogs but rats were used later on. In dogs, duodenum is re- sected distal to pylorus and opening of PD then double layer sutured. The continuity of the gastrointestinal tract is maintained by gastrojejunostomy and common bile duct is obliterated with sutures [3]. Mc Cutcheon and Race injected barium sulphate in to the loop and retrieved it inside the PD intraoperatively [4]. The same authors after severing the mucosal valvu- lae of Oddi found that under physiologic intraduodenal pressures reflux into PD occured [5]. In this model if PD is sutured pancreas atrophies. Byme and Joison’s modi- fication enables easy suturing of distended PD after in- jection of secretin [6]. Contributions to this method were made by Chetty et al. via either filling the duodenum with Proteus and E coli infected human bile [2] or filling duodenum with auto- claved human bile [7]. This model also explains the hyperamylasemia and duodenopancreatic reflux in afferent loop obstruction after Billroth 2 gastrectomy [8]. The histopathological changes in pancreas after this method are studied in detail by Rao et al. Mild to moderate pancreatitis is seen in six hours and hemorrhagic pancreatitis becomes widespread after 18 hours. Although changes similar to human pancreatitis is encountered, this could also be the result of systemic  B. D. YILDIZ ET AL. Copyright © 2010 SciRes. SS 32 response to duodenal surgery [9]. Dickson et al. assessed the applicability of CDL on humans [7]. Their criticism was as follows: - Generally mild pancreatitis occurs - Infected duodenal fluid flows into PD and causes bacterial infiltration of pancreas while this is not the usual case in human pancreatitis - Transmural duodenal necrosis and cholangitis kill the animal - Peritoneal sepsis and bacteremia accompanies the pancreatitis at all times in CDL whereas This is not a common finding in human pancreatitis [10]. 3. Diet Induced Pancreatitis The relationship between feeding with ethionine and acute pancreatitis is well known [11]. Ethionine is toxic to pancreatic acinar cells [12]. It inhibits phospholipid metabolism intracellularly [13,14]. Lombardi et al induced acute hemorrhagic pancreatitis in female mice with 0.5% ethionine enriched diet [15]. Widespread intra-abdominal fatty necrosis follows pan- creatitis. If feeding is limited to 24 hours mortality is 55-60%. If fed ad libidum this diet is 100% lethal in 5 days [16]. Histopathologic and gross examination of pancreas between 48-72 hours after 24 hours feed did not show any pancreatic damage [17]. When animals are fed with choline, pancreatitis does not develop [18]. Choline takes up the ethyl groups liberated during breakdown of ethionine. Female sex steroids seem to promote development of pancreatitis so either young female mice or oestrogen treated male mice are pre- ferred [19]. Diet without choline exerts synergistic effect to ethi- onine causing intraparanchymal activation of zymogens leading to massive hemorrhagic necrosis. The subcellu- lar mechanism underlying this is the inhibition of mem- brane lipid synthesis resulting in breakdown of endo- plasmic reticulum and release of autophagic vacuoles. The end result is autolysis [20-22]. The diet model appears to be a good approximation of severe necrotizing human pancreatitis. Both the gross and histological appearance of the pancreatic and peri- pancreatic inflammation as well as the clinical and bio- chemical course of diet-induced pancreatitis resemble human disease. Ascites, acidosis, hypoxia and hypo- volemia occur in this model like in human pancreatitis. The time course of the morphological and biochemical alterations have extensively been studied and are thus well defined in this model. However, small size of the animals used is a limitation for evaluation of surgical procedures and new diagnostic tools [23]. 4. Arginine Induced Pancreatitis Apart from ethionine, other amino acids like arginine can also induce pancreatitis. High dose intraperitoneal injec- tion of 500 mg/100 gr arginine can cause acute necrotiz- ing pancreatitis in rats, rabbits and mice [24-28]. The possible mechanisms underlying the effect of ar- ginine is via excessive nitric oxide production, lipid per- oxidation and inhibition of protein synthesis [29-31]. Dose and exposure of arginine determines the severity of pancreatitis in this model. The changes range between interstitial edema, inflammatory infiltration, acinar de- granulation to massive necrosis after 250 mg/kg and 450 mg/100 kg of injections respectively [32,33]. In addition to ease in controlling the destruction, argi- nine exerts minimal effect on other tissues which makes this model a plausible non invasive method for experi- mental pancreatitis [34]. The only drawback is its weak clinical relevance which made this method get replaced by other models. 5. Secretagogue Induced Pancreatitis Cerulein is a decapeptide analogue of cholecystokinin (CCK) derived from the skin of the amphibian Hyra caerula. When given either 1-5 ng/kg intravenous (iv) bolus or 0.25-1 ng/kg/min iv infusion or 50-100 ng/kg subcutaneously this substance increases pancreatic secre- tions [22]. If administered in supramaximal doses it causes edematous pancreatitis by increasing pancreatic protein secretions [35]. Cerulein interferes with packaging of zymogens and lysosomal hydrolases after synthesis in endoplasmic re- ticulum leading to intracellular activation of trypsinogen [36]. In 48 hours after infusion zymogen granules start fusion with lysosomes resulting in inflammation and acute pancreatitis [37,38]. The usual way of administration is by a catheter in- serted in internal jugular vein of the rat at a rate of 1-2 ml/hour [39,40]. Cerulein can be diluted in normal saline and infused iv in 3-5 hours [41,42]. Cerulein can also be administered intraperitoneally [43- 45]. Multiple injections can be done in one hour intervals with 5-200 g/kg doses. Subcutaneous delivery can be achieved in multiple in- jections with 25-50 g/kg dose [46,47]. In order to increase the degree of pancreatitis more than one model can be used. Schmidt et al. combined iv cerulein (5 g/kg/hr) with low pressure intraductal gly- codeoxycholic acid infusion [48]. They observed that edema, acinar necrosis, inflammation and hemorrhage were profound. Schoenberg et al. infused cerulein (5 micrograms/kg per hour) for 30 minutes, 3.5 hours, and 12 hours in rats.  B. D. YILDIZ ET AL. Copyright © 2010 SciRes. SS 33 No damage was seen after 30 minutes whereas after 3.5 hours interstitial edema, intravascular migration of gran- ulocytes, zymogen degranulation and acinar cell necrosis was seen. After 12 hours, histological evaluation showed pronounced zymogen degranulation, extensive tissue necrosis, and migration of granulocytes into the tissue. Amylase and lipase activities increased 15 and 35-fold respectively during this time [49]. 6. Duct Obstruction Induced Pancreatitis This model mimics benign and malignant partial or com- plete obstruction of PD. The model reflects tumors, gall- stone disease, trauma in the clinical setting. The surgical manipulation is simple, requiring either ligation of the common biliopancreatic duct or obstruction of the pan- creatic duct by vertical cannulation or insertion of a bal- loon-tipped catheter. The point of obstruction is close to the entry to duodenum, much like gallstone obstruction at the ampulla of Vater [50,51]. Duct obstruction leads to acinar atrophy without caus- ing pancreatitis. The physiological mechanism of this model is thought to be similar to that of the CDL tech- nique. It is postulated that bile reflux by triggering intra- pancreatic digestive enzyme activation accounts for the major pathological factor in this model. Duct obstruction induced pancreatitis can be complicated with other stimulations and surgical manipulations. For example, caerulein or secretin can be administered to the animal together with duct ligation to exaggerate the pancreatic secretions [52-54]. The severity of pancreatitis produced by the duct ob- struction model varies depending on the animal species used for experiment. In dogs physiological pressure in PD is 30 cmH2O [55]. When PD is ligated pressure rises to 40-80 cmH2O in 6-12 hours. Fluid accumulation in PD starts in 10-30 hours and continues up to 40 hours [56, 57]. After 24 hours the equilibrium between secretion and PD obstrucion is maintained which stops further PD pressure rise and parenchymal water content [55,56]. One week after PD ligation acinar cell zymogen content was found to be decreased, rough endoplasmic reticulum is fragmented, golgi apparatus function is lost, autophagic vacuoles appear and exocrine pancreas is replaced with fibrous tissue [57]. These changes occur faster in rats than dogs. In rats, main bile duct passes through pancreas and many small pancreatic ducts join with it. In order to pre- vent flow of only pancreatic secretions, duodenum is separated from transverse colon and a polyethylene tube inserted in to the proximal part of main bile duct [58]. In rabbits PD obstruction does not lead to the mor- phological changes of pancreatic trauma or inflammation but exocrine pancreas atrophies. PD is directly cannu- lated and located in vertical direction in rabbits. This is thought to mimic obstructive biliary pancreatitis in hu- mans [59]. This technique had been also utilized for as- sessment of effect of pancreatic enzymes on small intes- tine brush border enzyme activity [60]. Oppossums were also used for this model. Oppos- sum’s bile structure closely resembles human biliary system. Bile tract has a single terminal end combining with PD 2-3 cm before opening into duodenum. Occlusion of the common bilipancreatic duct causes acute hemorrhagic pancreatitis and results in 100% mor- tality in 14 days [61]. When it is sutured adjacent to duodenum, pancreatic edema forms in 6 hours and peaks in 12 hours. At this stage fatty necrosis and parenchymal hemorrhage start to appear and infiltration by inflammatory cells occurs [61- 63]. Another variant of this techique is partial obstruction of the pancreatic duct studied on cats. After exposure of the PD it is partially sutured proximally. PD is cannu- lated from the tail and secretions are collected. The se- cretion is increased with secretin and CCK. It was found that changes in pancreas depend on the degree of ob- struction. If it exceeds 75%, acinar atrophy and decrease in response to secretin and CCK stimulation occurs. Lesser degrees of obstruction only impairs enzymatic secretions. Three months after recovery from obstruction neither enzyme nor bicarbonate secretions return to nor- mal and tissue regeneration does not occur [64]. The disadvantage of this technique is difficulty in determin- ing the degree of obstruction which is assessed by in- stilling vinyl chloride in retrograde fashion in to PD and examining it under microscope. The duct obstruction model has high clinical relevance in that it simulates obstruction induced AP. Moreover, this induction method is quick and does not require so- phisticated surgical techniques. These advantages have made this model a favorite for investigating the patho- physiology, as well as the therapeutic treatment of ob- struction induced pancreatitis. It does not require ad- ministration of systemically active substances. Although not used as frequently as it had been, it should be kept in mind when experimenting chronic obstructive pancreati- tis as acinar cell loss and fibrosis is encountered in long term ductal obstruction. 7. Ex Vivo Perfusion Model This model was first described by Saharia et al. in 1977. It enables experimentation of different etiologies of pan- creatitis [65]. The technical details are as follows: Pancreas of the dog is mobilized with the duodenal segment adjacent to it. Splenic artery and superior mesenteric artery distal to  B. D. YILDIZ ET AL. Copyright © 2010 SciRes. SS 34 inferior pancreaticoduodenal artery is cannulated. Portal vein is cannulated and incoming venous blood is col- lected in a reservoir. A 16 G polyethylene catheter is placed in PD via a small duodenotomy. The circulation in this model is first started with 200ml of autologous blood. Human serum albumin (2.5 g), glucose (500 mg) and sodium bicarbonate (20 ml) is added to the perfused blood. During the experiment pH should be kept at 7.40. Blood glucose level is fixed at 100 mg/dl [65,66]. After the pancreas is harvested it is stored on a plexi- glass surface in a humid environment. The blood in ve- nous reservoir is passed through 95% oxygen and 5% carbondioxide suppyling oxygenator. Another pump pu- shes back the blood via the splenic and superior mesen- teric arteries. The index for blood flow is either 20-30 ml/min or 1 ml/min/6 gr of tissue [67]. Temperature of the perfusate is adjusted to 37°C. Partial obstruction can be added to the model by inserting 25 G catheter in to pancreas [68]. Increasing the blood flow results is edema [65]. Albumin added previously decreases edema and hemorrhage of the pancreas [69]. Alcoholic pancreatitis can be induced by adding free fatty acids or acetaldehyde in to perfusate [65,70-73]. Different etiologies can be studied by changing the flow rate, oxygen content, delaying perfusion or adding ceru- lein [71,74,75]. Although expensive, ex vivo perfusion model is a plausible model as the organ is isolated from body pre- venting systemic factors intervening. A complex equip- ment which has a propensity for breakdown in about 4 hours made this model remain inpopular. 8. Duct Infusion Pancreatitis Cannulation of the pancreatic duct provides another way of inducing an experimental AP model. Once the cannula has been implanted, an exogenous substance can be in- fused into the pancreas via the pancreatic ductal system. Several substances have been used as inducers of pan- creatitis in this method. These have included stimulating factors and toxic substances such as bile acids (tauro- cholate or glycodeoxycholic acid), ethyl alcohol, perace- tate and tert-butyl hydroperoxide. The most common of all these substances are bile acids [76-78]. In rats biliopancreatic duct is catheterized with 24 G polyethylene tube and ligated [79]. Main hepatic duct is clamped under liver and intraductal infusion is started. Glycodeoxycholic acid prepared in glycylglycine buffer (pH = 8) is recommended as infusate. Infusion should be in 1.5 minutes, with 30 mmHg pressure and 0.1-0.5 ml volume. In dogs trypsin is used along with bile acids [80]. After duodenectomy accessory pancreatic duct is cannulated with 1.5 mm tube and bile acids and trypsin in 1:1 ratio, 0.5 ml/kg solution is given with 140-150 mmHg pressure. Infusion of bile acids is a fast and cheap way of inducing pancreatitis resembling human pancreatitis. Mortality can be controlled with changing the quantity of the in- fusate. Both edematous and hemorrhagic pancreatitis can be induced. Major disadvantage is different response of different species to infusion. Taurodeoxycholate (0.2 ml, 0.025 molar, glycylgly cine-NaOH, pH: 8.0) is the second most used substance. In rats it is delivered 0.04 ml/min with an infusion pump [81]. Schoenberg et al. recommend that the pressure does not exceed 15 cmH2O during infusion [82]. In 3.5 hours 20% of rats die while in 57% die in 12 hours. After 3.5 hours fulminant hemorrhagic pancreatitis is seen under light microscope. Zymogen degranulation, 50% cell ne- crosis, mild tissue edema, inflammatory cell infiltration is observed. In 12 hours almost all of the acinar cells undergo necrosis. In dogs 20 G catheter is placed in pancreatic duct and 1.8 gr sodium taurocholate with 250.000 U benzoyl L- arginine ethyl ester hydrochloride crystal trypsine in 20 ml sorenson buffer infusion is carried on for 30 minutes not exceeding a pressure of 30 cmH2O [83]. Intraductal taurocholate infusion causes severe pancreatitis. Inflam- mation is not homogenous and mostly on the head of pancreas [84]. The repeatability and clinical relevance associated with the duct perfusion induced pancreatitis make it an excellent experimental model for pancreatitis studies. However it requires careful monitoring of perfusion pressure and an invasive surgery. Intraductal infusion of saline alone has been reported to induce mild pancreatitis [85]. Findings demonstrated that pancreatic injury is at- tributable not only to the exogenous substance infused but the combination of the exogenous substance and the hydrostatic pressure associated with the infusion. The presence of exaggerated hydrostatic pressure makes it less clinically relevant relative to other models like the duct obstruction model. Despite this drawback, the duct perfusion model is the most commonly used pancreatitis model because of its similarity to clinical pancreatitis [86,87]. The confounding effects of increased ductal pressure can be ameloriated by antegrade perfusion model which is first studied by Reber et al. [88]. They used cats for this purpose. The technique requires removal of spleen and greater omentum. Two catheters are placed in PD; one through duodenum and the other from the tail of pancreas [89]. Perfusion is maintained by a pump at a rate of 0.2-3.75 ml/hour for two hours. At this rate intra- ductal pressure does not exceed 20 cmH2O. Reber et al. recommend use of certain substances (bile, aspirin, hy- drochloric acid, ethanol, secondary bile acids) to over- come pancreatic canal barrier and increase permeability. 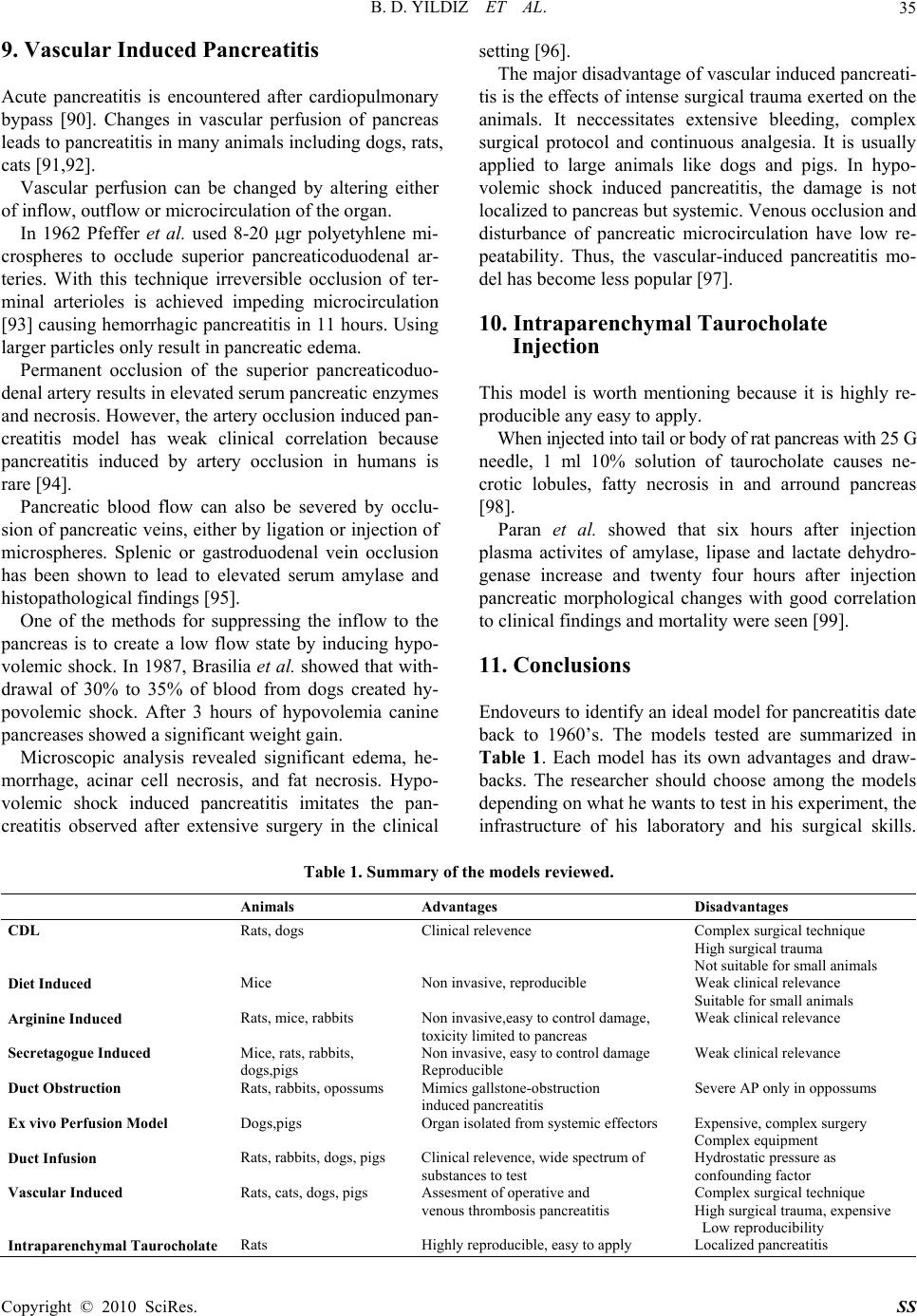 B. D. YILDIZ ET AL. Copyright © 2010 SciRes. SS 35 9. Vascular Induced Pancreatitis Acute pancreatitis is encountered after cardiopulmonary bypass [90]. Changes in vascular perfusion of pancreas leads to pancreatitis in many animals including dogs, rats, cats [91,92]. Vascular perfusion can be changed by altering either of inflow, outflow or microcirculation of the organ. In 1962 Pfeffer et al. used 8-20 gr polyetyhlene mi- crospheres to occlude superior pancreaticoduodenal ar- teries. With this technique irreversible occlusion of ter- minal arterioles is achieved impeding microcirculation [93] causing hemorrhagic pancreatitis in 11 hours. Using larger particles only result in pancreatic edema. Permanent occlusion of the superior pancreaticoduo- denal artery results in elevated serum pancreatic enzymes and necrosis. However, the artery occlusion induced pan- creatitis model has weak clinical correlation because pancreatitis induced by artery occlusion in humans is rare [94]. Pancreatic blood flow can also be severed by occlu- sion of pancreatic veins, either by ligation or injection of microspheres. Splenic or gastroduodenal vein occlusion has been shown to lead to elevated serum amylase and histopathological findings [95]. One of the methods for suppressing the inflow to the pancreas is to create a low flow state by inducing hypo- volemic shock. In 1987, Brasilia et al. showed that with- drawal of 30% to 35% of blood from dogs created hy- povolemic shock. After 3 hours of hypovolemia canine pancreases showed a significant weight gain. Microscopic analysis revealed significant edema, he- morrhage, acinar cell necrosis, and fat necrosis. Hypo- volemic shock induced pancreatitis imitates the pan- creatitis observed after extensive surgery in the clinical setting [96]. The major disadvantage of vascular induced pancreati- tis is the effects of intense surgical trauma exerted on the animals. It neccessitates extensive bleeding, complex surgical protocol and continuous analgesia. It is usually applied to large animals like dogs and pigs. In hypo- volemic shock induced pancreatitis, the damage is not localized to pancreas but systemic. Venous occlusion and disturbance of pancreatic microcirculation have low re- peatability. Thus, the vascular-induced pancreatitis mo- del has become less popular [97]. 10. Intraparenchymal Taurocholate Injection This model is worth mentioning because it is highly re- producible any easy to apply. When injected into tail or body of rat pancreas with 25 G needle, 1 ml 10% solution of taurocholate causes ne- crotic lobules, fatty necrosis in and arround pancreas [98]. Paran et al. showed that six hours after injection plasma activites of amylase, lipase and lactate dehydro- genase increase and twenty four hours after injection pancreatic morphological changes with good correlation to clinical findings and mortality were seen [99]. 11. Conclusions Endoveurs to identify an ideal model for pancreatitis date back to 1960’s. The models tested are summarized in Table 1. Each model has its own advantages and draw- backs. The researcher should choose among the models depending on what he wants to test in his experiment, the infrastructure of his laboratory and his surgical skills. Table 1. Summary of the models reviewed. Animals Advantages Disadvantages CDL Rats, dogs Clinical relevence Complex surgical technique High surgical trauma Not suitable for small animals Diet Induced Mice Non invasive, reproducible Weak clinical relevance Suitable for small animals Arginine Induced Rats, mice, rabbits Non invasive,easy to control damage, Weak clinical relevance toxicity limited to pancreas Secretagogue Induced Mice, rats, rabbits, Non invasive, easy to control damage Weak clinical relevance dogs,pigs Reproducible Duct Obstruction Rats, rabbits, opossums Mimics gallstone-obstruction Severe AP only in oppossums induced pancreatitis Ex vivo Perfusion Model Dogs,pigs Organ isolated from systemic effectors Expensive, complex surgery Complex equipment Duct Infusion Rats, rabbits, dogs, pigs Clinical relevence, wide spectrum of Hydrostatic pressure as substances to test confounding factor Vascular Induced Rats, cats, dogs, pigs Assesment of operative and Complex surgical technique venous thrombosis pancreatitis High surgical trauma, expensive Low reproducibility Intraparenchymal Taurocholate Rats Highly reproducible, easy to apply Localized pancreatitis  B. D. YILDIZ ET AL. Copyright © 2010 SciRes. SS 36 Some models test etiology while others simulate the complications of pancreatitis. Combination of models can also be used if single model does not fulfill the needs. Ideal model which by itself demonstrates all aspects of pancreatitis including systemic changes is yet to be de- scribed. 12. References [1] C. Wilson and C. W. Imrie, “Experimental Models of Acute Pancreatitis,” In: C. D. Johnson and C. W. Imrie, Eds., Pancreatic Disease: Progress and Prospects, Springer-Verlag London Limited, Great Britain, 1991, pp. 227-239. [2] U. Chetty, H. M. Gilmour and T. V. Taylor, “Experimen- tal Acute Panereatitis in the Rat-A New Model,” Gut, 1980, Vol. 21, No. 2, pp. 115-117. [3] F. C. Nance and J. L. Cain, “Studies of Hemorrhagic Panerearitis in Germ-Free Dogs,” Gastroenterology, Vol. 55, No. 3, 1968, pp. 368-374. [4] A. D. Mc Cutcheon and D. Race, “Experimental Pan- creatitis: A Possible Etiology of Postoperative Pancreati- tis,” Annals of Surgery, Vol. 155, No. 4, 1962, pp. 523- 531. [5] A. D. Mc Cutcheon, “Reflux of Duodenal Contents in the Pathogenesis of Panereatitis,” Gut, Vol. 5, 1964, pp. 260- 265. [6] J. J. Byme and J. Joison, “Bacterial Regurgitation in Ex- perimental Panereatitis,” American Journal of Surgery, Vol. 107, No. 2, 1964, pp. 317-320. [7] A. P. Dickson, A. K. Foulis and C. W. Imrie, “Histology and Bacteriology of Closed Duodenal Loop Models of Experimental Acute Panereatitis in the Rat,” Digestion, Vol. 34, No. 1, 1986, pp. 15-21. [8] T. W. Arends and D. L. Nahrwold, “Gastric Resection and Reconstruction,” In: G. D. Zuidema, Ed., Shakelford’s Surgery of the Alimentarv Tract, 3rd Edition, Vol. II, W.B. Saunders Company, Philadelphia, l991, pp. 149- 172. [9] S. S. Rao, I. A. Watt, L. A. Donaidson, A. Crocket and S. N. Joffe, “A Serial Histologic Study of the Development and Progression of Acute Panereatitis in the Rat,” American Journal of Pathology, Vol. 103, No. 1, 1981, pp. 39-46. [10] A. K. Foulis, W. R. Murray and D. Galloway, et al., “En- dotoxemia and Complement Activation in Acute Pan- creatitis,” Gut, Vol. 23, No. 8, 1982, pp. 656-661. [11] A. Horie, T. Takino, L. Hennan and P. J. Fitzgerald, “Pancreas Acinar Cell Regeneration. Relationship of Acid Phosphatase and β-Glucuronidase to Intracelular Organelles and Ethionine Lesions,” American Journal of Pathology, Vol. 63, No. 2, 1971, pp. 299-318. [12] E. W. Loring and L. J. Hanley, “The Destructive Effects of Dl-Ethionine on the Pancreas. Stomach and Submaxil- lary Glands,” American Journal of Pathology, Vol. 31, No. 3, 1955, pp. 521-533. [13] F. B. Gordon and E. Farbel, “Selective Effects of Ade- nine Triphosphate upon the Hepatic Biochemical Le- sionsinduced by Ethionine,” Archives of Biochemistry and Biophysics, Vol. 112, No. 2, 1965, pp. 233-237. [14] T. Ariyoshi and E. Takabatake, “Effects of Phenobarbital Ethanol and Ethionine on the Content and Fatty Acid Composition of Hepatic Microsomal Phospholipids,” Chemistry and Pharmacology Bulletin, Vol. 20, No. 1, 1972, pp. 170-174. [15] B. Lombardi, L. W. Estes and D. S. Longnecker, “Acute Hemorrhagic Pancreatisis (Massive Necrosis) with Fat Necrosis Induced in Mice by DL-Ethionine Fed with a Choline Defficient Diet,” American Journal of Pathology, Vol. 79, No. 3, 1975, pp. 465-480. [16] M. L. Steer and J. Meldoresi, “The Cell Biology of Ex- perimental Pancreatitis,” New England Journal of Medi- cine, Vol. 316, No. 3, 1987, pp. 144-150. [17] M. Steer, “How and Where Does Acute Pancreatitis Be- gin,” Archives of Surgery, Vol. 127, No. 11, 1992, pp. 1350-1353. [18] L. Gilliland and M. L. Steer, “Effects of Ethionine on Digestive Enzyme Synthesis and Discharge by Mouse Pancreas,” American Journal of Physiology, Vol. 239, No. 5, 1980, pp. 418-426. [19] K. N. Rao, P. K. Eagon and K. Okamura, “Acute Hem- orrhagic Pancreatic Necrosis in Mice. Induction in Male Mice Treated with Estradiol,” American Journal of Pa- thology, Vol. 109, No. 7, 1982, pp. 8-14. [20] D. E. Leevathi, S. L. Katyal and B. Lombardi, “Lecithin Depletion in Liver Mitochondria of Rats Fed with Cho- line-Deficint Diet. Effect of β-Hydroxybutyrate Dehy- drogenase,” Life Sciences, Vol. 14, No. 7, 1974, pp. 1203-1210. [21] H. Rinderknecht, “Activation of Pancreatic Zymogens: Normal Activation. Premature Intrapancreatic Activation, Protective Mechanisms against Inappropriate Activation,” Digestive Disease Sciences, Vol. 31, No. 3, 1986, pp. 314-321. [22] K. N. Rao, M. F. Zuretti, F. M. Bacchino and B. Lombardi, “Acute Hemorrhagic Pancreatitis in Mice. The Activity of Lysosomal Enzymes in the Pancreas and the Liver,” American Journal of Pathology, Vol. 98, No. 1, 1980, pp. 45-60. [23] C. Niederau, R. Lüthen, M. C. Niederau, J. H. Grendell and L. D. Ferrell, “Acute Experimental Hemorrhagic- Necrotizing Pancreatitis Induced by Feeding a Cho- line-Deficient, Ethionine-Supplemented Diet. Methodol- ogy and standards,” European Surgical Research, Vol. 24, No. (Suppl. 1), 1992, pp. 40-54. [24] T. Mizunuma, S. Kawamura and Y. Kishino, “Effects of Injecting Excess Arginine on Rat Pancreas,” Journal of Nutrition, Vol. 114, No. 3, 1984, pp. 467-471. [25] Y. Kishino and S. Kawamura, “Pancreatic Damage In- duced by Injecting a Large Dose of Arginine,” Virchows Arch B: Cell Pathology Including Molecular Pathology, Vol. 47, No. 2, 1984, pp. 147-155. [26] S. Tani, H. Itoh, Y. Okabayashi, et al, “New Model of  B. D. YILDIZ ET AL. Copyright © 2010 SciRes. SS 37 Acute Necrotizing Pancreatitis Induced by Excessive Doses of Arginine in Rats,” Digestive Disease Sciences, Vol. 35, No. 3, 1990, pp. 367-374. [27] N. Bulbuller, O. Dogru, H. Umac, et al., “The Effects of Melatonin and Pentoxiphylline on L-Arginine Induced Acute Pancreatitis,” Ulusal Travma Dergisi, Vol. 11, No. 2, 2005, pp. 108-114. [28] H. F. Cui and Z. L. Bai, “Protective Effects of Trans- planted and Mobilized Bone Marrow Stem Cells on Mice with Severe Acute Pancreatitis,” World Journal of Gas- troenterology, Vol. 9, No. 10, 2003, pp. 2274-2277. [29] Q. L. Zhao, C. Y. Huang, Y. Huang, et al., “Study on Acute Pancreatitis-Associated Lung Injury Induced by L-Arginine in Mice,” Sichuan Da Xue Xue Bao Yi Xue Ban, Vol. 35, No. 6, 2004, pp. 839-842. [30] Y. Kishino, S. Takama and S. Kitajima, “Ultracytochem- istry of Pancreatic Damage Induced by Excess Lysine,” Virchows Arch B, Vol. 52, No. 2, 1986, pp. 153-167. [31] T. Takacs, L. Czako, E. Morschl, et al., “The Role of Nitric Oxide in Edema Formation in L-Arginine-Induced Acute Pancreatitis,” Pancreas, Vol. 25, No. 3, 2002, pp. 277-282. [32] L. Czako, T. Takacs, I. S. Varga, et al., “Involvement of Oxygen-Derived Free Radicals in L-Arginine-Induced Acute Pancreatitis,” Digestive Disease Sciences, Vol. 43, No. 8, 1998, pp. 1770-1777. [33] J. Hardman, S. Jamdar, C. Shields, et al., “Intravenous Selenium Modulates L-Arginine-Induced Experimental Acute Pancreatitis,” Journal of Pancreas, Vol. 6, No. 5, 2005, pp. 431-437. [34] M. Tashiro, C. Schafer, H. Yao, et al., “Arginine Induced Acute Pancreatitis Alters the Actin Cytoskeleton and In- creases Heat Shock Protein Expression in Rat Pancreatic Acinar Cells,” Gut, Vol. 49, No. 2, 2001, pp. 241-250. [35] G. Bertaccini, G. de Caro, R. Endean, V. Erspamer and M. Impicciatore, “The Action of Caerulein on Pancreatic Se- cretion of the Dog and Biliary Secretion of the Dog and Rat,” British Journal of Pharmacology, Vol. 37, No. 1, 1969, pp. 185-197. [36] A. Tardini, P. Anversa, C. Bordi, G. Bertaccini and M. Impicciatore, “Ultrastructural and Biochemical Changes after Marked Caerulein Stimulation of the Exocrine Pan- creas in the Dog,” American Journal of Pathology, Vol. 62, No. 1, 1971, pp. 35-47. [37] M. Lampel and H. Kem, “Acute Interstitial Pancreatitis in the Rat Induced by Excessive Doses of a Pancreatic Se- cretagogue,” Virchows Archiv A: Pathological Anatomy and Histopathology, Vol. 373, No. 2, 1977, pp. 107-117. [38] O. Watanabe, M. Baccino, M. L. Steer and J. Meldoresi, “Supramaximal Cerulein Stimulation and Ultrastructure of Rat Pancreatic Acinar Cell, Early Morphological Changes, during Development of Acute Pancreatitis,” American Journal of Physiology, Vol. 246, No. (4 Pt 1), 1984, pp. 457-467. [39] M. L. Steer, J. Meldoresi and C. Figarella, “Pancreatitis: The Role of Lysosomes,” Digestive Disease Sciences, Vol. 29, No. 10, 1984, pp. 934-938. [40] G. Adler, C. Hahn, H. F. Kem and K. N. Rao, “Cerulein- Induced Panereatitis in Rats: Increased Lysosomal En- zyme Activity and Autophagocytosis,” Digestion, Vol. 32, No. 1, 1985, pp. 10-18. [41] A. Dabrowski, A. Gabryelewicz, U. Wereszynska Siemi- atkowska and L. Chyczewsla, “Oxygen-Derived Free Radicals in Cerulein-Induced Acute Pancreatitis,” Scan- dinavian Journal of Gastroenterology, Vol. 23, No. 10, 1988, pp. 1245-1249. [42] K. S. Guice, D. E. Miller, K. T. Oldham, C. M. Town- send, Jr. and J. C. Thompson, “Superoxide Dismutase and Catalase. A Possible Role in Established Panereatitis,” American Journal of Surgery, Vol. 151, No. 1, 1986, pp. 163-169. [43] A. Dabrowsky and M. Chwiecko, “Oxygen Radicals Me- diate Depletion of Pancreatic Sulfnydryl Compounds in Rats with Cerulein-Induced Acute Pancreatitis,” Diges- tion, Vol. 47, No. 1, 1990, pp. 15-19. [44] J. R. Wisner and I. G. Renner, “Allopurinol Attenuates Caerulein Induced Acute Pancreatitis in the Rat,” Gut, Vol. 29, No. 7, 1988, pp. 926-929. [45] Z. Devenyl, J. L. Orchard and R. E. Powers, “Xanthine Oxidase Activitiy in Mouse Pancreas: Effects of Cae- rulein-Induced Acute Pancreatitis,” Biochemical and Biophysical Research Communications, Vol. 149, No. 3, 1987, pp. 841-845. [46] C. Niderau, L. Ferrel and J. H. Grendell, “Caerulein- Induced Acute Necrotizing Pancreatitis in Mice: Pro- tectjve Effects of Proglumide, Benztript and Secretin,” Gastroenterology, Vol. 88, No. 5, 1985, pp. 1192-1204. [47] H. Yamaguchi, T. Kimura and H. Nawata, “Does Stress Play a Role in the Development of Severe Pancreatitiis in Rats?” Gastroe nterology, Vol. 98, No. 6, 1990, pp. 1682- 1688. [48] K. A. Zucker, T. E. Thomas, J. E. Sussman and I. M. Modlin, “New Potent Cholecystokinine Antagonists Block Cerulein Induced Pancreatitis,” Surgery Forum, Vol. 28, No. 4, 1987, pp. 142-144. [49] B. A. Neuschwander-Tetri, L. D. Ferrell, R. J. Sukhabote and J. H. Grendell, “Glutathione Monoethy Ester Ame- liorates Caerulein-Induced Pancreatiti in the Mouse,” Journal of Clinical Investigation, Vol. 89, No. 6, 1992, pp. 109-116. [50] G. Ohshio, A. Saluja and M. L. Steer, “Effects of Short- Term Pancreatic Duct Obstruction in Rats,” Gastroen- terology, Vol. 100, No. 1, 1991, pp. 196-202. [51] M. M. Lerch, A. K. Saluja, M. Runzi, et al., “Pancreatic Duct Obstruction Triggers Acute Necrotizing Pancreatitis in the Opossum,” Gastroenterology, Vol. 104, No. 3, 1993, pp. 853-861. [52] K. Yoshinaga, M. Washizuka and Y. Segawa, “Chole- cystokinin Acts as an Essential Factor in the Exacerbation of Pancreatic Bile Duct Ligation-Induced Rat Pancreatitis Model Under Non-Fasting Condition,” Japanese Journal of Pharmacology, Vol. 84, No. 1, 2000, pp. 44-50. [53] T. Hirano, T. M. Yotsumoto and K. Ando, “Changes of  B. D. YILDIZ ET AL. Copyright © 2010 SciRes. SS 38 Acinar Cells in the Pancreato-Biliary Duct Ligation with Exocrine Pancreatic Stimulation Model in Rats, Protec- tive Effects of a New Potent Protease Inhibitor, ONO3307,” Nippon Geka Hokan, Vol. 60, 1991, pp. 342- 353. [54] T. Hirano and T. Manabe, “Effect of Short-Term Pan- creatico-Biliary Duct Obstruction with Intraductal Hy- pertension on Subcellular Organelle Fragility and Pan- creatic Adenylate Energy Metabolism in Rats: Protective Effect of a New Protease Inhibitor, E-3123,” Acta Chi- rurgica Belgica, Vol. 94, No. 2, 1994, pp. 80-85. [55] D. W. Elliot, R. D. Williams and R. M. Zollinger, “Al- terations in the Pancreatic Resistance to Bile in the Patho- genesis of Acute Pancreatitis,” Annals of Surgery, Vol. 146, No. 4, 1975, pp. 669-682. [56] A. E. Dumont and A. B. Martelli, “Pathogenesis of Pan- creatic Edema Following Exocrine Duct Obstruction,” Annals of Surgery, Vol. 168, No. 2, 1968, pp. 302-309. [57] A. Churg and W. R. Richter, “Early Changes in the Exo- crine Pancreas of the Dog and Rat after Ligation of the Pancreatic Duct. A Light and Electron Microscopy Study,” American Journal of Pathology, Vol. 63, No. 3, 1971, pp. 521-526. [58] T. Tsuzuki, N. Watanabe and A. P. Thal, “The Effect of Obstruction of the Pancreatic Duct and Acute Alcoholism on Pancreatic Protein Synthesis,” Surgery, Vol. 57, 1965, pp. 724-729. [59] A. Saluja, M. Saluja, A. Villa, P. Rutledge, J. Meldoresi and M. Steer, “Pancreatic Duct Obstruction in Rabbits Causes Digestive Zymogen and Lysosomal Enzyme Colocalization,” Journal of Clinical Investigation, Vol. 84, No. 4, 1989, pp. 1260-1266. [60] M. Hauer Jensen, M. Christensen, H. D. Wilson and H. P. Schedel, “Intestinal Disaccharidase Acitivity Following Pancreatic Duct Occlusion in the Rat,” Pancreas, Vol. 2, No. 3, 1987, pp. 295-302. [61] N. Senninger, F. G. Moody, D. H. Van Buren, J. C. U. Coelco and Y. F. Li, “Effect of Biliary Obstruction on Pancreatic Exocrine Secretion in Conscious Opossums,” Surgery Forum, Vol. 35, 1984, pp. 226-228. [62] M. M. Lerch, A. K. Saluja, R. Dawra, P. Ramarao, M. Saluja and M. L. Steer, “Acute Necrotizing Pancreatitis in the Opossum: Earliest Morphological Changes Involve Acinar Cells,” Gastroenterology, Vol. 103, No. 1, 1992, pp. 205-213. [63] M. M. Lerch, A. K. Saluja, M. Rünzi, R. Dawra, M. Saluja and M. L. Steer, “Pancreatic Duct Obstruction Triggers Acute Necrotizing Pancreatitis in the Opossum,” Gastroenterology, Vol. 104, No. 5, 1993, pp. 853-861. [64] J. C. Austin, C. Roberts, M. J. Rosenhottz and H. A. Re- ber, “Effects of Partial Duct Obstruction and Drainage on Pancreatic Function,” Journal of Surgical Research, Vol. 28, No. 5, 1980, pp. 426-433. [65] P. Saharia, S. Margolis, G. D. Zuidema and J. L. Cam- eron, “Acute Pancreatitis with Hyperlipidemia: Studies with an Isolated Perfused Canine Pancreas,” Surgery, Vol. 82, No. 1, 1977, pp. 60-67. [66] M. G. San, G. B. Bulkley and J. L. Cameron, “The Role of Leukocytes in the Production of Oxygen Derived Free Radicals in Acute Experimental Pancreatitis,” Surgery, Vol. 101, No. 3, 1987, pp. 292-296. [67] H. Sanfey, G. B. Bulkley and J. L. Cameron, “The Source and Role of Oxygen-Derived Free Radicals in Three Dif- ferent Experimental Models,” Annals of Surgery, Vol. 201, No. 5, 1985, pp. 633-639. [68] P. Broe and J. Cameron, “Experimental Gallstone Pan- creatitis. Pathogenesis and Response to Different Treat- ment Modalities,” Annals of Surgery, Vol. 195, No. 5, 1982, pp. 566-573. [69] T. Kimura, G. Zuidema and J. L. Cameron, “Acute Pan- creatitis: Experimental Evaluation of Sreroid, Albumin and Trasyiol Therapy,” Annals of Surgery, Vol. 140, 1980, pp. 403-408. [70] H. Sanfey and J. L. Cameron, “Experimental Pancreatitis. Treatment with Osmotically Active Agents,” Surgery Forum, Vol. 33, 1982, pp. 216-217. [71] H. Sanfey, G. Bulkley and J. L. Cameron, “The Role of Oxygen-Derived Free Radicals in the Pathogenesis of Acute Pancreatitis,” Annals of Surgery, Vol. 200, No. 4, 1984, pp. 405-413. [72] M. G. Sarr, G. B. Bulkley and J. L. Cameron, “Temporal Efficacy of Allopurinol during the Induction of Pan- creatitis in the Ex Vivo Perfused Canine Pancreas,” Sur- gery, Vol. 101, No. 3, 1987, pp. 342-346. [73] I. H. Nordback, J. L. Olson, V. P. Chacko and J. L. Cam- eron, “Detailed Characterization of Experimental Acute Alcoholic Pancreatitis,” Surgery, Vol. l, 1995, pp. 41-49. [74] H. Sanfey, P. Broe and J. L. Cameron, “Experimental Ischemic Pancreatitis: Treatment with Albumin,” Ameri- can Journal of Surgery, Vol. 150, No. 3, 1985, pp. 297- 300. [75] J. A. Clemens, J. Olson and J. L. Cameron, “Cerulein- Infused Pancreatitis in the Ex Vivo Isolated Perfused Ca- nine Pancreas,” Surgery, Vol. 109, 1991, pp. 515-532. [76] E. Unal, H. Uzun, R. Kusaslan, et al., “Serum Parao- xonase (a High-Densitylipoprotein-Associated Lipophilic Antioxidant) Activity and Lipid Profile in Experimental Acute Pancreatitis,” Pancreas, Vol. 31, No. 1, 2005, pp. 84-87. [77] Z. Sledzinski, M. Wozniak, A. Brunelli, et al., “Experi- mental Pancreatitis Induced by Synthetic Prooxidant Tert-Butyl Hydroperoxide,” Pancreas, Vol. 20, No. 2, 2000, pp. 146-151. [78] K. Jankowski, J. Kubasik-Juraniec, Z. Sledzinski, et al., “The Morphology of Acinar Cells during Acute Pan- creatitis in Rats Induced by Intraductal Infusion of Per- acetate,” Folia Microbiologica, Vol. 63, 2004, pp. 179- 181. [79] J. Schmidt, K. Lewandrowsky and A. L. Warshaw, C. C. Compton and D. W. Rattner, “Morphometric Charachter- istics and Homogeneity of a New Model of Acute Pan- creatitis in the Rat,” International Journal of Pancrea- tology, Vol. 12, No. 1, 1992, pp. 41-51. [80] J. Shen, M. K. Huang and F. L. Wu, “Hemodynamic Changes during Acute Pancreatitis and the Dopamine  B. D. YILDIZ ET AL. Copyright © 2010 SciRes. SS 39 Therapy,” Chinese Medical Journal, Vol. 103, No. 3, 1990, pp. 20l-207. [81] N. Wang, R. Andersson, V. Soltesz, P. Leveau and I. Ihse, “Gut Origin Sepsis, Macrophage Functionand Oxygen Extraction Associated with Acute Pancreatitis in the Rat,” World Journal of Surgery, Vol. 20, No. 3, 1996, pp. 299- 308. [82] M. H. Schoenberg, M. Büchler, M. Younes, R. Kirchmayr, U. B. Brücker and H. B. Beger, “Effect of Antioxidant Treatment in Rats with Acute Hemorrhagic Pancreatitis,” Digestive Disease Sciences, Vol. 39, No. 5, 1994, pp. 1034-1040. [83] R. Chardavoyne, A. Asher, B. Simmy, T. A. Stein and L. Wise, “Role of Reactive Oxygen Metabolites in the Early Cardiopulmonary Changes of Acute Hemorrhagic Pan- creatitis,” Digestive Disease Sciences, Vol. 3, 1989, pp. 1581-1584. [84] M. L. Steer, “Workshop on Pancreatitis,” Digestive Dis- ease Sciences, Vol. 30, No. 6, 1985, pp. 575-581. [85] H. Paran, J. Klausner, A. Siegal, E. Graff, U. Freund and O. Kaplan, “Effect of the Somatostatin Analogue Octreo- tide on Experimental Pancreatitis in Rats,” Journal of Surgical Research, Vol. 62, 1996, pp. 201-206. [86] A. Lichtenstein, R. Milani, Jr., S. M. Fernezlian, et al., “Acute Lung Injury in Two Experimental Models of Acute Pancreatitis: Infusion of Saline or Sodium Tauro- cholate into the Pancreatic Duct,” Critical Care Medicine, Vol. 28, No. 5, 2000, pp. 1497-1502. [87] E. Vaquero, I. Gukovsky, V. Zaninovic, et al., “Localized Pancreatic NF-KappaB Activation and Inflammatory Response in Taurocholate-Induced Pancreatitis,” Ameri- can Journal of Physiology - Gastrointestinal and Liver Physiology, Vol. 280, No. 6, 2001, pp. 1197-1208. [88] R. Lightwood and H. A. Reber, “Micropuncture Study of Pancreatic Secretion in the Cat,” Gastroenterology, Vol. 72, No. 1, 1977, pp. 61-66. [89] H. A. Reber, C. Roberts and L. W. Way, “The Pancreatic Mucosal Duct Barrier,” American Journal of Surgery, Vol. 137, No. 1, 1979, pp. 128-134. [90] G. S. Haas, A. L. Warshaw, W. M. Dagget and H. T. Aretz, “Acute Pancreatitis after Cardiopulmonary By- pass,” American Journal of Surgery, Vol. 149, No. 4, 1985, pp. 508-515. [91] H. Friess, A. Weber and M. Buchler, “Standards in Moni- toring Acute Experimental Pancreatitis,” European Sur- gical Research, Vol. 24, No. (Suppl. 1), 1992, pp. 1-13. [92] H. Waldner, “Vascular Mechanisms to Induce Acute Pancreatitis,” European Surgical Research, Vol. 24, No. (Suppl. 1), 1992, pp. 62-67. [93] R. B. Pfeffer, A. Lazzarini-Robertson, D. Safadi, Jr., G. Mixter, C. F. Secoy, Jr. and J. W. Himon, “Gradation of Pancreatitis: Edermatous through Hemorrhagic, Experi- mentally Produced by Controlled Injection of Micro- spheres into Blood Vessels in Dogs,” Surgery, Vol. 51, 1962, pp. 564-569. [94] D. A. Dreiling, M. Koller and C. H. Su, “Vascular Pan- creatitis: A Neglected Disorder,” Mount Sinai Journal of Medicine, Vol. 53, No. 3, 1986, pp. 482-484. [95] S. Sjovall, T. Holmin, A. Evander, et al., “Splenic and Gastro-Duodenal Vein Occlusion Influence on the Pan- creatic Gland and on the Outcome of Experimental Pan- creatitis,” International Journal of Pancreatology, Vol. 3, 1988, pp. 143-149. [96] A. Barzilai, B. J. Ryback, J. A. Medina, et al., “The Mor- phological Changes of the Pancreas in Hypovolemic Shock and the Effect of Pretreatment with Steroids,” In- ternational Journal of Pancreatology, Vol. 2, No. 1, 1987, pp. 23-32. [97] H. Waldner, “Vascular Mechanisms to Induce Acute Pancreatitis,” European Surgical Research, Vol. 24, No. (Suppl. 1), 1992, pp. 62-67. [98] O. Kaplan, T. Kushnir, U. Sandbank and G. Navon, “Acute Pancreatitis in Rats: A 31P Nuclear Magnetic Resonance Study,” Journal of Surgical Research, Vol. 45, 1987, pp. 172-178. [99] H. Paran, A. Mayo, D. Kidron, G. Sivak, T. Reshef, T. Vider, O. Ziv and U. Freund, “Experimental Acute Ne- crotising Pancreatitis: Evaluation and Characterisation of a Model of Intraparenchymal Injection of Sodium Tau- rocholate in Rats,” European Surgical Research, Vol. 166, No. 11, 2000, pp. 894-898. |