Journal of Biomedical Science and Engineering
Vol.6 No.6(2013), Article ID:33659,6 pages DOI:10.4236/jbise.2013.66077
Diagnostic accuracy of color Doppler in diagnosis of Hepatocellular carcinoma taking histopathology as gold standard
![]()
1Department of Radiology, Mayo Hospital/King Edward Medical University, Lahore, Pakistan
2Department of Gynecology and Obstetric, Lady Aitchison, Lahore, Pakistan
3Department of Pathology King Edward Medical University, Lahore, Pakistan
Email: drmhbukhari@yahoo.com, mulazim.hussain@gmail.com
Copyright © 2013 Wajid Ali et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received 1 April 2013; revised 7 May 2013; accepted 22 May 2013
Keywords: Hepatocellular Carcinoma; Doppler Sonography; Focal Liver Lesions
ABSTRACT
Hepatocellular carcinoma (HCC) is the fifth most common cancer in the world and the third most common cause of cancer mortality. Despite the high numbers of patients diagnosed worldwide, HCC continue to pose challenging clinical problems. Good-quality ultra sound with careful evaluation of the entire liver can be a screening examination for HCC in patients at risk. The aim of the study was to determine the diagnostic accuracy of the Doppler sonography for differentiation of hepatocellular carcinoma (HCC) from other focal liver lesions by taking histopathology as a gold standard. It was Cross-sectional survey, conducted in the Department of Diagnostic Radiology, King Edward Medical University/Mayo Hospital, Lahore in one year from 13-12-2010 to 12-12-2011. A total of 70 patients were included in this study with focal lesion on ultrasound are included while pregnant patient are excluded. After evaluating by Doppler sonography and doing core biopsy, the patients were sent to the department of pathology Mayo hospital for Histopathological examination. Histopathology was assessed for confirmation of positive and negative cases. Mean age of the patients was 60.9 ± 4.7 years. Out of 70 patients, 47 patients (67.1%) were male while remaining 23 patients (32.9%) were female. On Doppler sonography 37 cases were positive for hepatocellular carcinoma and 33 cases were negative while 36 cases were positive and 34 negative on histopathology. On Doppler sonography, sensitivity (94.4%), specificity (91.1%), diagnostic accuracy (92.8%), positive predictive value (91.8%) and negative predictive value was 93.9%. We concluded that Doppler sonography is a useful method for differen- tiation of Hepatocellular carcinoma from other focal liver lesions, detection and characterization of heaptocellular carcinoma.
1. INTRODUCTION
Hepatocellular carcinoma (HCC) is a malignancy of the hepatoyte, usually leading to death within 6 - 20 months. Its prevalence is 2% of all malignancies. Hepatocellular carcinoma often arises in the setting of cirrhosis, appearing 20 - 30 years following the initial insult to the liver. However, 25% of patients have no history of risk factor for the development cirrhosis [1].
HCC is the 8th most common cancer in women and 5th most frequent cancer in men world-wide. The incidence of HCC changes according to the occurrence of hepatitis B and C infections. In Asia and sub-Saharan Africa HCC have high rates of infectious hepatitis with incidences of 120 cases per 100,000 [2]. The most common malignancy of the liver is metastases from other organs: 25% - 50% patients with a known non-hematological malignancy have liver metastases at the time of diagnosis [3].
Moreover, differential diagnosis of these liver lesions is difficult, even with clinical, biochemical data, and imaging techniques [4-9]. Recently Doppler sonography has been used to characterize focal hepatic lesions with a higher diagnostic confidence [10]. The detection rate (sensitivity) of colour Doppler sonography to detect the malignant tumours has been reported 92% as compared its Histopathological findings [11,12]. Lin et al. done a study for differential diagnosis of hepatocellular carcinoma and metastasis in 54 patients with at least one lesion measuring diameter <3 cm and found the sensitivity and specificity of Doppler ultrasonography for hepatocellular carcinoma was 80.8% and 96.4%, respectively [13].
In our setup some invasive and costly techniques such as MRI, histopathology and CT scan are used to detect these lesions. Studies on colour Doppler sonography has not been established before, hence this study has been designed to see the diagnostic role of Doppler sonography in detection and differentiation of hepatocellular carcinoma (HCC) by taking histopathology as a gold standard.
This study will help us to choose this non-invasive and cheep diagnostic tool if it will be high effective as reported in the previous literature.
The study was conducted to determine the diagnostic accuracy of the Doppler sonography for differentiation of hepatocellular carcinoma (HCC) from other focal liver lesions by taking histopathology as a gold standard.
2. MATERIAL AND METHODS
A cross sectional study was conducted in the Department of Radiology and Pathology on 70 patients presented with intra hepatic lesions, coming from the indoor and outdoor patents of Mayo Hospital, Lahore.
After meeting inclusion and exclusion criteria about 70 patients, referred from other departments of Mayo Hospital were enrolled in the study. All basic demographic information of each patient was obtained on proforma after informed consent. By using covex probes 2.5 - 3.5 MHz scanning was done at the department of Radiology, Mayo Hospital, Lahore by a single radiologist. The colour Doppler scan was optimized for each patients using low PRF (to obtained accurate results), high gain and filter setting. At first morphological characteristics of lesions including echogenicity, posterior enhancement, echogenic rim and target appearance was seen by Bmode sonography. This presence and or absence of heaptocellular carcinoma (as per operational definition) were assessed. After evaluating by Doppler sonography and doing CORE biopsy, the patients were sent to Department of Pathology Mayo hospital for Histopathological examination. Then the report of histopathology was assessed for confirmation of positive and negative cases.
2.1. Study Design
Cross sectional.
2.2. Study Settings
Department of Diagnostic Radiology, King Edward Medical University/Mayo Hospital, Lahore.
2.3. Duration of Study
Study was carried out over a period of one year from 13-12-2010 to 12-12-2011.
2.4. Sample Size
A total of 70 patients with 95% confidence level, 5% margin of error and expected percentage of HC i.e 48.78% and taking sensitivity and specificity of Doppler USG i.e. 80.8% and 96.4%, respectively taking histopathology as gold standard.
2.5. Sampling Technique
A Non-probability purposive sampling was suggested for this study.
2.6. Sample Selection
The patients were selected according to following criteria.
2.7. Inclusion Criteria
1) Confirmed patients of focal liver lesions diagnosed on ultrasonography (USG) having age 20 - 70 years with either sex with the positive history of hepatitis B hepatictis C and cirrhosis.
2) Lesions of <3 cm of size detected on USG.
2.8. Exclusion Criteria
Pregnant females.
2.9. Hepatocellular Carcinoma
Labeled on Doppler sonography if resistive index value was <0.4.
2.10. Resistive Index (RI)
Measured by formula = (systolic peak frequency – enddiastolic frequency/peak systolic frequency.
2.11. True Positive
Diagnosed as HCC on Doppler sonography and confirmed on histopathology.
2.12. True Negative
Diagnosed as non-HCC on Doppler sonography and also confirmed as non-HCC on histopathology.
2.13. False Negative
Diagnosed non-HCC on Doppler sonography but confirmed as HCC on histopathology.
3. DATA ANALYSIS PROCEDURE
The collected data were analyzed statistically by sing SPSS version 12.0. Quantitative data like age was presented in form of mean ± SD. Qualitative data gender was presented in form of frequency and percentage. A 2 × 2 table was used to calculate sensitivity, specificity, negative predicted value (NPV), positive predicted value (PPV) and accuracy of Doppler sonography taking histopathology as a fold standard.
Fine needle aspiration biopsy was taken and sent to Department of Pathology for cytology and Histopathological evaluation. The slides were stained with hematoxylin and eosin methods.
4. RESULTS
A total of 70 confirmed patients of focal liver lesions diagnosed on ultrasonography (USG) having age 20 - 70 years with either sex with the positive history of hepatitis B hepatitis C and cirrhosis during the study period of six months from 13-12-2010 to 12-12-2011. Majority of the patients i.e., 33 (47.2%) were between 41 - 60 years of age and minimum 11 patients (15.7%) were between 61 - 70 years with mean age of 60.9 ± 4.7 years (Table 1).
Out of 70 patients, 47 patients (67.1%) were male while remaining 23 patients (32.9%) were female (Table 1).
Table 1 also shows distribution of cases by presentation by number of nodules. On Doppler sonography 37 cases were positive for hepatocellular carcinoma and 33 cases were negative while 36 cases were positive and 34 negative on histopathology (Table 2).
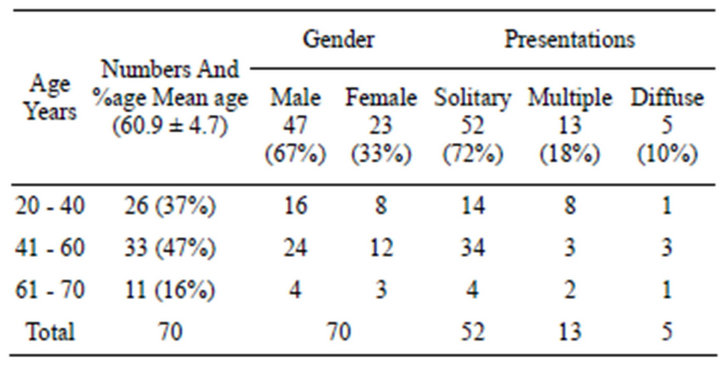
Table 1. Distribution of cases by Age.
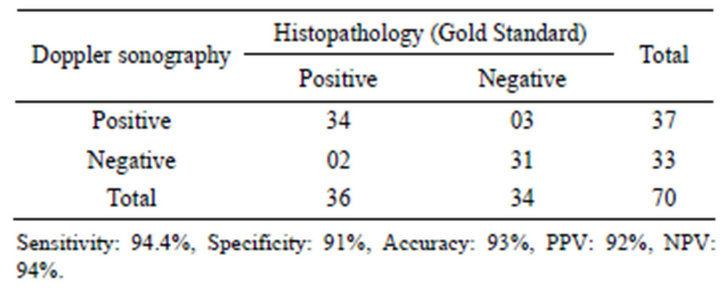
Table 2. Comparison of Doppler sonography vs histopathology’ for differentiation of hepatocellular carcinoma (HCC) from other focal liver lesions n = 70.
Out of 36 malignant lesions,one patient was of cholangiocarcinona and 4 patients were of metastatic carcinoma. (Figure 1).
Doppler sonography findings were compared with histopathology and cytopathology and the sensitivity (94.5%), specificity (91%), diagnostic accuracy (93%), positive predictive value (92%) and negative predictive value was observed 93.9% (Tables 2 and 3).
On histopathological examinations, Cholangiocarcinoma cells showed glandular pattern and tubular architecture of cuboidal to columnar epithelium. The architecture of hepatocellular carcinoma was arranged in sheets of pleomorphic cells of hepatic origin (sheets of large cells with abundant and granular cytoplasm). Eosinophilic cytoplasm, hyperchromatic nuclei with prominent nucleoli, large number of mitoses and increased nuclear to cytoplasmic ratio (Figure 2).
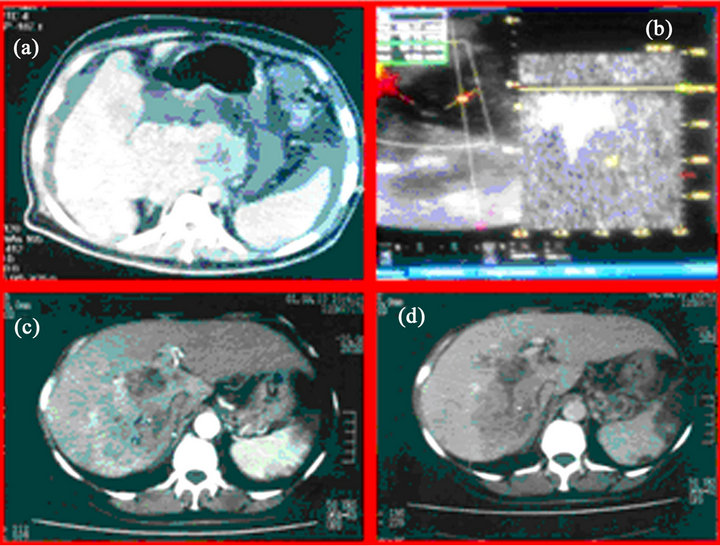
Figure 1. (a) CT scans of a 50 year old male patientof cirrhotic liver with heterogeneously mass lesion in caudate lobe (segment I) with another hypedense lesion in segment V of right lobe. Ascites and peritoneal metastasis as well splenomegaly. IVC expanded with thrombus. (b) color doppler image of Hepatic mass low resistance flow pattern. (c) Case ii, 56-year-old male patient. Venous phase hepatomegaly with multicentric mass lesion in right lobe (segment V and VI) peripheral enhancement, thrombus in IVC, cavernous transformation and splenic infarcts. (d) Case ii, 56-year-old male patient. Venous phase hepatomegaly with multicentric mass lesions in the right lobe(Segment V and CI) wash out of contrast, hrombus in IVC, cavernous transformation and splenic infarcts.
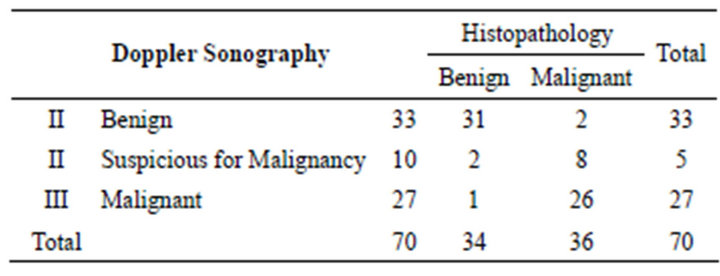
Tables 3. Distribution of different Hepatic lesions diagnosed Doppler Sonography as compared to Histopathology.
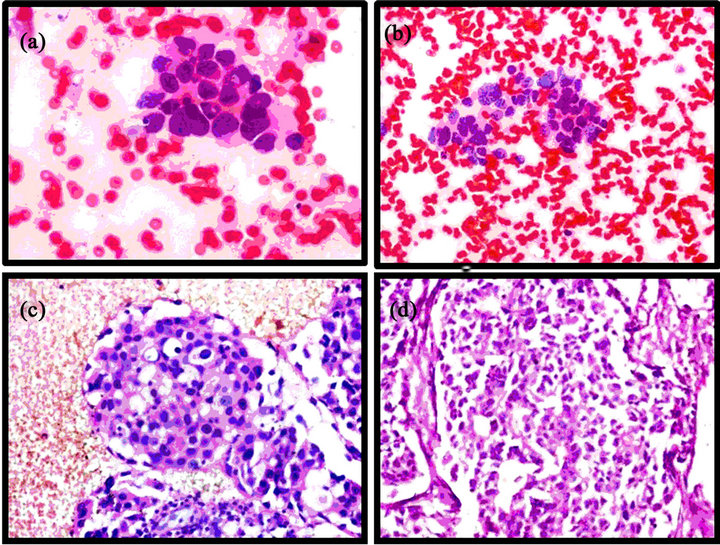
Figure 2. Photomicrograph of (H&E 20×), (a) Cells arranged in glandular pattern on Histopathology (d), showing tubular architecture of cuboidal to columnar epithelium (H&E 40×). Photomicrograph of (H&E 20×), (a) Cells arranged in sheets on cytology (sheets of large cells with abundant and granular cytoplasm) while on Histopathology (d), showing (H&E 40×) pleomorphic large cells of hepatocellular origin (Eosinophilic cytoplasm, hyperchromatic nuclei with prominent nucleoli, large number of mitoses and increased nuclear to cytoplasmic ratio).
5. DISCUSSION
Hepatocellular carcinoma (HCC) was believed to be a rare disease in the early 1900s. In Germany, Eggel found only 163 cases of HCC autopsies when he surveyed the world literature for HCC. He proposed an anatomical classification that HCC was classified as nodular, massive and diffuse [14].
Hepatocellular carcinoma (HCC) accounts for more than 90% of all primary liver cancers [15]. It ranks fifth in frequency worldwide among all malignancies and causes one million deaths annually [16]. Over 500,000 new cases are currently diagnosed every year [16] and HCC affects about three folds more males than females [17-19]. The incidence of HCC in Northern Europe, Australia and Caucasian populations in North America is less than 3 cases per 100,000 men, while the number of cases in Eastern Asia, Middle and Western Africa is much higher, and ranges from 20.8 to 48 per 100,000 individuals, since hepatitis B is endemic to those regions [20].
Hepatocellular carcinoma (HCC) is the most common primary hepatic malignancy worldwide, with an increasing incidence in western countries [21]. The prognosis for patients with HCC has marginally improved over the last 2 decades. The outcome of patients with HCC is generally very poor without treatment [22]. The diagnosis is often made at an advanced tumour stage, precluding curative options such as surgical resection, transplantation or local ablation therapy. Small HCCs are clinically mostly asymptomatic and are the main topic in screening of risk groups. However, identification of HCC at an early stage is crucial for prompt surgical resection or transplantation [23].
Ultrasound has found its place in screening, guiding interventional therapy and post-therapeutic monitoring. The introduction of advanced techniques such as harmonic imaging, and power and Doppler modes, as well as contrast-enhanced techniques, have proved more effective than grey-scale imaging alone. In a suspicious hepatic lesion, CT and MRI are used for tumour assessment and staging. Especially the use of dynamic contrast-enhanced procedures has improved radiological diagnostic reliability. CT and MRI are better than US in detecting diffuse-type HCCs, bile duct and portal venous invasion. The characterization of lesions is the forte of MRI, because of the intrinsic tissue contrast as well as the availability of hepatospecific CM. Ongoing advances in MR-techniques are very promising both in improvements of sensitivity and in specificity of disease. Still, MRI is more time consuming than CT and needs a compliant patient because of the required breathhold imaging [23].
Patients with focal liver lesions (hemangioma, focal nodular hyperplasia, adenoma, hepatocellular carcinoma, metastatic lesions, focal fatty lesion) received the ultrasound contrast agent Levovist (300 mg/mL and 400 mg/mL) intravenously. This ultrasound contrast agent (a suspension of micrometer-sized microparticles of galactose and microscopic gaseous bubbles) can pass through the lungs without impairment. Ernst et al demonstrated that after the administration of Levovist, increased color flow signals were detected in the liver. Of 5/6 patients with metastatic liver lesions showed previously undetected blood flow in the rim of the tumor. In 4 patients with hepatocellular carcinoma, enhanced signal intensity was observed in the vessels of the rim and in 3 of those patients in the center of the tumor.
One patient with adenoma and one patient with focal nodular hyperplasia showed signal enhancement in the central area of the tumor. No signal enhancement was observed in hemangiomas, a focal fatty lesion, or in a carcinoid metastatic lesion. Levovist increased the echointensity of normal and tumor vessels in liver lesions. This new ultrasound contrast agent led to the detection of tumor vessels previously not detectable by conventional color flow imaging [24].
Color Doppler imaging has become a valuable method for the evaluation of the vascular supply of abdominal and pelvic organs and for obtaining clinically useful information related to organ perfusion and tumor vascularity [25].
In 1987, Taylor et al. described the presence of high velocity Doppler signals in HCC, which correlated with the angiographic findings of arteriovenous shunting frequently found in HCC while not in other liver lesions such as hemangiomas and metastases. Similar findings have been reported in subsequent studies, presented at the Radiological Society of North America meeting (December 1991) on the use of Doppler imaging in the differential diagnosis of focal hepatic lesions [26].
Tanaka et al. [26] used color flow Doppler imaging to differentiate HCC from other focal hepatic lesions. In their study, the sensitivity of basket and vessels-withinthe-tumor patterns as shown by color flow Doppler imaging for the diagnosis of HCC was 80%. The specificity for the diagnosis of HCC vs other focal hepatic lesions was 100%. In our study, although most HCCs had the basket and vessels within-the-tumor patterns, these patterns were also seen in the metastases [27].
In a study by Lin et al. [27] the clinical utility of color Doppler sonography in the differentiation of hepatocellular carcinoma from metastases and hemangioma was investigated in 72 hepatocellular carcinomas (80 lesions), 30 metastases (82 lesions), and 39 hemangiomas (54 lesions). Overlaps of color patterns were found among hepatocellular carcinoma, metastases and hemangioma. Pulsatile waves from lesions with the basket, vessels within tumor, or spot patterns, or lesions measuring less than 3 cm with detectable signals, did not favor the diagnosis of hemangioma [28].
In current study comparison of Doppler sonography with histopathology for differentiation of hepatocellular carcinoma (HCC) from other focal liver lesions was made and we observed sensitivity (94.5%), specificity (91.1%) diagnostic accuracy (93%), positive predictive value (92%) and negative predictive value (94%). Our findings are comparable with histopathology the results of Lin et al, they found the sensitivity and specificity of Doppler ultrasonography for hepatocellular carcinoma 80.8% and 96.4%, respectively [13].
6. CONCLUSION
Doppler sonography is a useful method for differentiation of Hepatocellular carcinoma from other focal liver lesions, detection and characterization of hepatocellular carcinoma.
7. FUTURE STRATEGIES
If a quantitative data could be drawn from the remote sensing, the data analysis could be more intuitionistic to indicate the results. We suggest that in future more and more research should be made because color Doppler sonography can aid in the differentiation of hepatocellular carcinoma from hemangioma but may be unreliable in the differentiation of hepatocellular carcinoma from hypervascular metastases.
REFERENCES
- Schottenfeld, D. and Fraumeni, J. (2006) Cancer epidemiology and prevention. 3rd Edition, University Press, New York. doi:10.1093/acprof:oso/9780195149616.001.0001
- Stuart, K. (2009) Primary hepatic carcinoma. http://emedicine.medscape.com/article/282814-overview
- Albreeht, T. (2005) Sonography of liver metastases. In: Lencioni, R. and Cioni, D., Eds., Focal Liver Lesions, Detection, Characterization, Ablation, Springer-Verlag, Heidelberg, Berlin, 261-274.
- Sherman, M. (2005) Diagnosis of small hepatocellular carcinoma. Hepatology, 42, 14-16. doi:10.1002/hep.20790
- Stojkovic, M.V., Artiko, V.M., Radoman, I.B., Knezevic, S.J., Lukic, S.M., Kerkez, M.D., et al. (2009) Color Doppler sonography and angioscintigraphy in hepatic Hodgkin’s lymphoma. World Journal of Gastroenterology, 15, 3269-3275. doi:10.3748/wjg.15.3269
- SK, B. (2007) Ultrasound differential diagnosis. Jaypee Brothers Medical Publishers Ltd, New Delhi.
- Dragoteanu, M., Balea, I.A., Dina, L.A., Piglesan, C.D., Grigorescu, I., Tamas, S., et al. (2008) Staging of portal hypertension and portosystemic shunts using dynamic nuclear medicine investigations. World Journal of Gastroenterology, 14, 3841-3848. doi:10.3748/wjg.14.3841
- Artiko, V.M., Sobic-Saranovic, D.P., Pavlovic, S.V., Perisic-Savic, M.S., Stojkovic, M.V., Radoman, I.B., et al. ( 2008) Estimation of the relative liver perfusion using two methods of radionuclide angiography in the patients with hemodynamic disorders in the portal system. Acta Chirurgica Iugoslavica, 55, 11-16. doi:10.2298/ACI0801011A
- Artiko, V., Obradovic, V., Petrovic, M., Perisic, M., Stojkovic, M., Sobic-Saranovic, D., et al. (2007). Hepatic radionuclide angiography and Doppler ultrasonography in the detection and assessment of vascular disturbances in the portal system. Hepatogastroenterology, 54, 892- 897.
- Kim, S.H., Lee, J.M., Lee, J.Y., Han, J.K., An, S.K., Han, C.J., et al. (2005) Value of contrast-enhanced sonography for the characterization of focal hepatic lesions in patients with diffuse liver disease: receiver operating characteristic analysis. American Journal of Roentgenology, 184, 1077-1084. doi:10.2214/ajr.184.4.01841077
- Wang, Y., Wang, W.P., Ding, H., Huang, B.J., Mao, F. and Xu, Z.Z. (2004) Resistance index in differential diagnosis of liver lesions by color doppler ultrasonography. World Journal of Gastroenterology, 10, 965-967.
- Fracanzani, A.L., Burdick, L., Borzio, M., Roncalli, M., Bonelli, N., Borzio, F., et al. (2001).Contrast-enhanced Doppler ultrasonography in the diagnosis of hepatocellular carcinoma and premalignant lesions in patients with cirrhosis. Hepatology, 34, 1109-1112. doi:10.1053/jhep.2001.29373
- Lin, Z.Y., Chang, W.Y., Wang, L.Y., Chen, S.C., Chuang, W.L., Hsieh, M.Y., et al. (1992). Duplex pulsed Doppler sonography in the differential diagnosis of hepatocellular carcinoma and other common hepatic tumours. British Journal of Radiology, 65, 202-206. doi:10.1259/0007-1285-65-771-202
- But, D.Y., Lai, C.L. and Yuen, M.F. (2008) Natural history of hepatitis-related hepatocellular carcinoma. World Journal of Gastroenterology, 14, 1652-1656. doi:10.3748/wjg.14.1652
- Yu, A.S. and Keeffe, E.B. (2003). Management of heaptocellular carcinoma. Reviews in Gastroenterological Disorders, 3, 8-24.
- Llovet, J.M., Burroughs, A. and Bruix, J. (2003) Hepatocellular carcinoma. Lancet, 362, 1907-1917. doi:10.1016/S0140-6736(03)14964-1
- Qian, J., Feng, G.S. and Vogl, T. (2003) Combined interventional therapies of hepatocellular carcinoma. World Journal of Gastroenterology, 9, 1885-1891.
- Qian, J., Vossoughi, D., Woitaschek, D., Oppermann, E., Bechstein, W.O., Li, W.Y., et al. (2003) Combined transarterial chemoembolization and arterial administration of Bletilla striata in treatment of liver tumor in rats. World Journal of Gastroenterology, 9, 2676-2680.
- Perry, J.F., Strasser, S.I., George, J., Farrell, G.C. and McCaughan, G.W. (2003). Pharmacotherapy of hepatocellular carcinoma. Expert Opinion on Pharmacotherapy, 4, 2175-2185. doi:10.1517/14656566.4.12.2175
- Kudo, M. (2011). Diagnostic imaging of hepatocellular carcinoma: Recent progress. Oncology, 81, 73-85. doi:10.1159/000333265
- Bosch, F.X., Ribes, J., Diaz, M. and Cleries, R. (2004) Primary liver cancer: Worldwide incidence and trends. Gastroenterology, 127, S5-S16. doi:10.1053/j.gastro.2004.09.011
- Perz, J.F., Armstrong, G.L., Farrington, L.A., Hutin, Y.J. and Bell, B.P. (2006). The contributions of hepatitis B virus and hepatitis C virus infections to cirrhosis and primary liver cancer worldwide. Journal of Hepatology, 45, 529-538. doi:10.1016/j.jhep.2006.05.013
- Llovet, J.M. (2005) Updated treatment approach to heaptocellular carcinoma. Journal of Gastroenterology, 40, 225-235. doi:10.1007/s00535-005-1566-3
- Ernst, H., Hahn, E.G., Balzer, T., Schlief, R. and Heyder, N. (1996). Color doppler ultrasound of liver lesions: Signal enhancement after intravenous injection of the ultrasound contrast agent Levovist. Journal of Clinical Ultrasound, 24, 31-35. doi:10.1002/(SICI)1097-0096(199601)24:1<31::AID-JCU5>3.0.CO;2-M
- Yasuhara, K., Kimura, K., Ohto, M., Matsutani, S., Ebara, M., Tsuchiya, Y., et al. (1988) Pulsed Doppler in the diagnosis of small liver tumours. British Journal of Radiology, 61, 898-902. doi:10.1259/0007-1285-61-730-898
- Taylor, K.J., Ramos, I., Carter, D., Morse, S.S., Snower, D. and Fortune, K. (1998) Correlation of Doppler US tumor signals with neovascular morphologic features. Radiology, 166, 57-62.
- Tanaka, S., Kitamura, T., Fujita, M., Nakanishi, K. and Okuda, S. (1990) Color Doppler flow imaging of liver tumors. American Journal of Roentgenology, 154, 509- 514. doi:10.2214/ajr.154.3.2154912
- Lin, Z.Y., Wang, L.Y., Wang, J.H., Lu, S.N., Chen, S.C., Chuang, W.L., et al. (1997) Clinical utility of color Doppler sonography in the differentiation of hepatocellular carcinoma from metastases and hemangioma. Journal of Ultrasound in Medicine, 16, 51-58.