Health
Vol. 4 No. 5 (2012) , Article ID: 19318 , 3 pages DOI:10.4236/health.2012.45043
Sexually transmitted infections (STIs) in gynae-outpatients: Experience from a tertiary health centre
![]()
1Department of Obstertrics & Gynaecology, Government Medical College and Rajindra Hospital, Patiala, India;
*Corresponding Author: drharpreet_sidhu@hotmail.com, husanmeet@yahoo.co.in
2Department of Obstertrics & Microbiology, Government Medical College and Rajindra Hospital, Patiala, India
3Department of Obstertrics & Pathology, Government Medical College and Rajindra Hospital, Patiala, India
Received 26 June 2011; revised 1 July 2011; accepted 15 July 2011
Keywords: STIs; Vaginal Discharge; HIV; Pap Smear
ABSTRACT
Background: Prospective analysis of 500 cases of vaginal discharge in tertiary health centre of Punjab. Objective: To study the prevalence of Sexually transmitted infections (STIs) in 500 outpatient of 15 - 49 years age group with vaginal discharge and to evaluate the various factors influencing pattern of STIs. Method: All cases were subjected to cervical cytology, HIV ELISA, rapid plasma reagen (RPR) test for syphilis and Gram’s staining, Giemsa staining and wet mount study of vaginal discharge. Results: Prevalence of STIs was found to be 58% and majority of infection was caused by G. vaginalis, Candida and Trichomonas. Pap smear showed koilocytosis in 5.6%, mild dysplasia in 1.8% and carcinoma cervix in 1.2% cases. Conclusion: Vaginal discharge is a common gynaecological complaint and STIs are significant cause of vaginal discharge.
1. INTRODUCTION
Sexually transmitted infections (STIs) are a group of communicable diseases that are transmitted predominantly by sexual contact and in addition, a number of other diseases which are generally acquired by other means, may also be acquired during coitus and produce genital lesions [1]. List of pathogens which are sexually transmissible has expanded from five “classical” venereal disease agents to include more than twenty agents. STIs form a major public health problem in the world. They rank among the five most important causes of loss of years of productive life in developing countries. True incidence of STIs is difficult to estimate not because of inadequate reporting but because of secrecy and taboos that surround them and their epidemiology depends upon interaction between sexually transmitted disease (STD) pathogens, behaviors that transmit them and effectiveness of preventive and control measures [1].
STIs compromise women’s health much more than that of men as many of them are transmitted more efficiently from men to women than from women to men and once infection occurs they produce complications more often in women. Early in the disease course, women are more likely to have asymptomatic infection which can result in delayed diagnosis. They are responsible for significant amount of female morbidity including infertility, infant illness, increased susceptibility to HIV infection, ectopic pregnancy, preterm labor, fetal death, low birth weight and malignancy. In the era of AIDS, there is resurgence of interest in STDs because of their role in facilitating HIV infection. Some of STDs agents like human papilloma virus (HPV) are known to have definite etiological role in causation of carcinoma cervix. Women attending STD clinic share two major risk factors for cervical carcinoma—early onset of coitus & multiple sex partners. Cervical cytology study has an important role in detecting changes due to STIs and neoplasia & preinvasive lesions at an early stage.
Present Study was undertaken to determine the prevalence of STIs in women with vaginal discharge presenting to gynaecology OPD.
2. MATERIAL AND METHODS
The present study was undertaken on 500 cases of vaginal discharge in the age group of 15 - 49 years attending gynaecology OPD of Government Medical College and Rajindra Hospital, Patiala (Punjab), India to determine the prevalence of STIs in women with vaginal discharge and to evaluate various factors influencing the pattern of STIs. All the women were subjected to cervical cytology by Pap smear examination so as to detect any inflammatory or dysplastic changes. Women were enquired regarding their knowledge about STIs. In each case detailed history, thorough physical and local pelvic examination along with various laboratory investigations were carried out. Gram staining, Giemsa staining and wet mount study of vaginal discharge was carried out to detect causative agents. All the women were subjected to HIV ELISA and RPR test for syphilis.
2.1. Statistical Methods
Descriptive statistical analysis has been carried out in the present study. Results on continuous measurements are presented on Mean ± SD (Min-Max) and results on categorical measurements are presented in Number (%). Significance is assessed at 5% level of significance. Student t test (two tailed, independent) has been used to find the significance of study parameters on continuous scale between two groups (Inter group analysis) on metric parameters, Chi-square/Fisher Exact test has been used to find the significance of study parameters on categorical scale between two or more groups. p-value of <0.05 has been taken as significant.
2.2. Statistical Software
The Statistical software namely SAS 9.2, SPSS 15.0, Stata 10.1, MedCalc 9.0.1, Systat 12.0 and R environment ver.2.11.1 were used for the analysis of the data and Microsoft Word and Excel have been used to generate graphs, tables etc.
3. RESULTS
A total of 500 cases of vaginal discharge in the age group of 15 - 49 years were evaluated. Majority of women were in the age group of 25 - 34 years and were illiterate and unemployed. Majority of the women were married and staying with their husband and only two percent were married but separated and 2.2% were unmarried.
A total of 290 women were detected to have infection, thus the prevalence of STIs was 58%. In 25.6% of cases, cause of vaginal discharge was not determined. Various other etiological factors for vaginal discharge were cervical erosion (11.6%), mild dysplasia in 1.8%, carcinoma cervix in 1.2%, cervical polyp in one percent, senile vaginitis in 0.8% (Table 1).
Out of 290 patients with infection 54% of cases had mixed infection. G. vaginalis was the causative agent in majority of cases (57.58%), followed by Candida albicans in 45.86%, T. vaginalis in 35.17% and HIV in 4.13% of cases. Syphilis (2.06%), gonorrhoea (0.68%) and group B streptococcus (2.06%) infection was comparatively less common. No case of Chlamydia trachomatis was found in present study (Table 2).
Pap smear revealed non-specific inflammation in 76% cases, infection with G. vaginalis in 14.4% and T. vaginalis in 2.4%. Koilocytic changes suggestive of viral infection were seen in 4.2% cases. There was evidence of mild dysplasia in 1.8% and carcinoma cervix in 1.2% of cases (Table 3).
Majority of the subjects were ignorant about STIs (78%) and only 22% were having awareness about causes, treatment or modes of prevention of STIs.
Thirty six percent women were taking oral contraceptive pills. There was history of prolonged intake of anti-
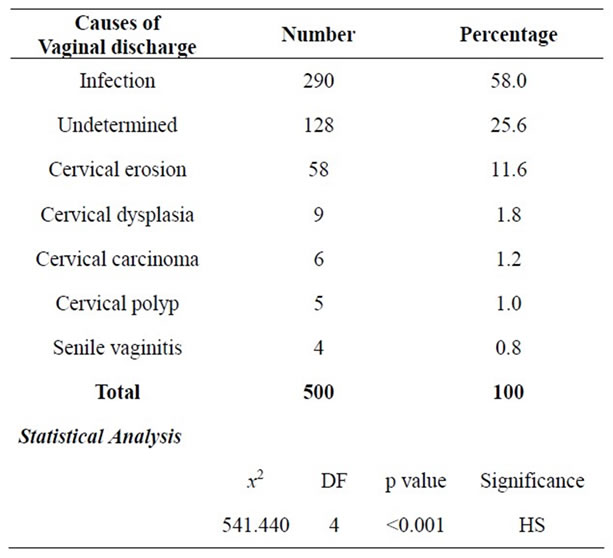
Table 1. Distribution of patients according to causes of vaginal discharge.
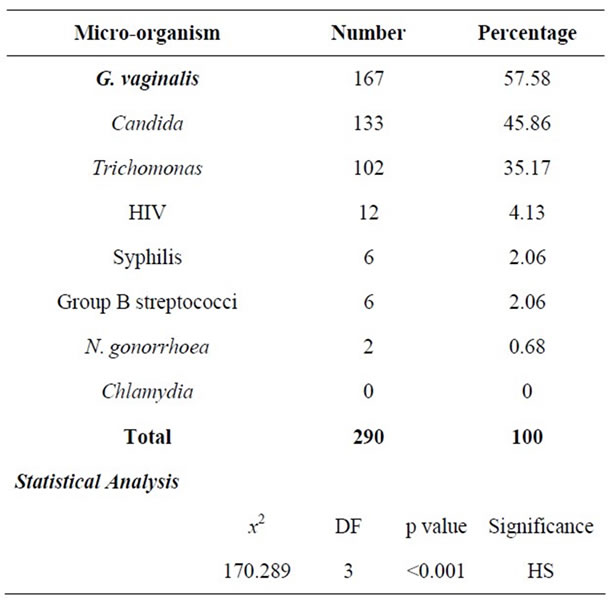
Table 2. Distribution of patients according to micro-organism causing vaginal discharge.
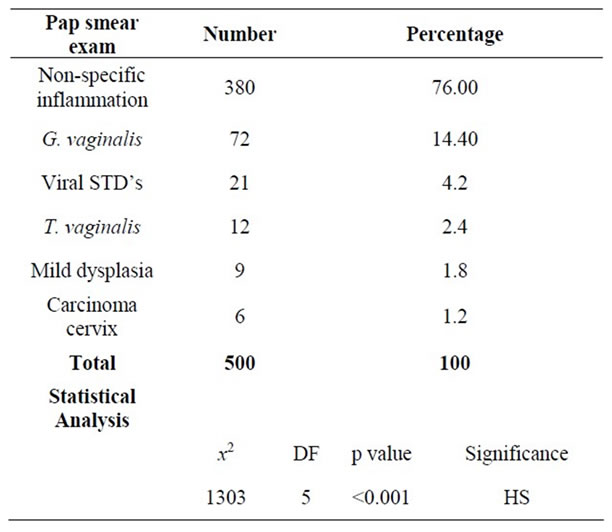
Table 3. Distribution of patients according to Pap smear examination.
biotics in 9.6% cases and diabetes mellitus was present in 6.8% cases. However, no predisposing factors were detected in 17.6% cases.
4. DISCUSSION
Vaginal discharge is the most common symptom of STIs. Although vaginitis is not a serious condition, it may have repercussions on women’s life. In the present study infection was the cause of vaginal discharge in 290 cases thus giving prevalence rate of STIs to be 58% [2,3].
Among these 290 cases of STIs—G. vaginalis was the causative agent in majority of cases followed by candida and Trichomonas [2,4,5]. HIV, syphilis, gonorrhoea and group B streptococcus were found in small number of cases. No case of chlamydia was detected in present study which may be because of very non-specific and insensitive method employed for its detection i.e. Giemsa stain to detect inclusion bodies [6] as facilities for immunoflourescent studies are not available in our institution [4,6].
A total of 46.20% of subjects were having polymicrobial infection, among these most common association was of G. vaginalis with Trichomonas and candida. HIV was associated mainly with Trichomonas, syphilis and gonorrhoea which is explained by the fact that there is loss of integrity of mucosal barrier in these infections [4].
Pap smear examination showed the presence of dysplastic cells in 1.8% cases and frank malignancy in 1.2%. High percentage of non-specific inflammation suggests the need for repeat smear after a course of antibiotics. Trends in mortality from carcinoma cervix closely follow trends in incidence of STIs as the women attending STD clinic share two major risk factors for carcinoma cervix i.e. early onset of coitus and multiple sex partners. So, carcinoma cervix can be considered as one of 3rd generation STDs [7]. Majority of women were ignorant regarding causes treatment and prevention of STIs [8]. Lifestyle and behavior are important factors affecting spread of STIs and these can be modified by proper knowledge through appropriate health education.
Among the predisposing factors—OCP use, prolonged use of antibiotics and diabetes mellitus were found to be important factors. This is because of alteration of normal vaginal ecosystem produced by these conditions [9].
5. CONCLUSION
Vaginal discharge is a common gynaecological complaint and STIs are important cause of vaginal discharge thus leading to significant proportion of female morbidity. G. vaginalis, Candida and Trichomonas are three important causes of vaginal discharge. Presence of STIs indicates high risk sexual behaviour for HIV and carcinoma cervix. Early diagnosis and management of STIs at an early stage will go a long way in improving women’s health, economy and society.
![]()
![]()
REFERENCES
- Wilcox, R.R. (1950) STDs: Definition. A Textbook of STDs, 11.
- Al Quaiz, J. M. (2000) Patients with vaginal discharge: A survey in a university primary care clinic in Riyadh City. Annals of Saudi Medicine, 20, 302-306.
- Catterall, R.D. (1970) Diagnosis of vaginal discharge. The British Journal of Venereal Diseases, 46, 122-124.
- Jain, N., Koranne, R.V., Sharma, R.C. and Malhotra, V.L. (1996) Clinico microbiological study of vaginal discharge in STD patients. Indian Journal of Sexually Transmitted Diseases, 17, 4-7.
- Driscoll, A.M., McCoy, D.R., Nicol, C.S. and Barrow, J. (1970) Sexually transmitted disease in gynaecological outpatients with vaginal discharge. The British Journal of Venereal Diseases, 46, 125-128.
- Gillbert, G.L. (1999) Chlamydia. In: Mackie and McCartney Practical Medical Microbiology, 14 Edition, Churchill Livingstone, London, 624.
- Farrer, C.J. and Tatham, P.H. (1962) Screening for carcinoma of the uterine cervix in a V.D. clinic. The British Journal of Venereal Diseases, 38, 230-231.
- Bhargava, N.C., Tewari, V.K. and Pandey, V.K. (1988) STD patients: A profile. Indian Journal of Sexually Transmitted Diseases, 9, 68-70.
- Sapre, S., Yadav, S. and Sharma, K. (2002) Vaginal and cervical cytology as a tool for surveillance of sexually transmitted diseases in cases attending OPD. The Indian Practitioner, 55, 567-570.