International Journal of Otolaryngology and Head & Neck Surgery
Vol.2 No.3(2013), Article ID:31844,4 pages DOI:10.4236/ijohns.2013.23021
Cervico-Facial Soft Tissue Emphysema with Pneumo-Mediastinum Following Endoscopic Sinus Surgery: A Dilemma of Related or Unrelated Complication
1Department of ENT, NMC Specialty Hospital, Abu Dhabi, UAE 2Department of General Surgery, NMC Specialty Hospital, Abu Dhabi, UAE
3Department of Radiology, NMC Specialty Hospital, Abu Dhabi, UAE
Email: *produl_ent@rediffmail.com
Copyright © 2013 Produl Hazarika et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received February 3, 2013; revised April 3, 2013; accepted May 3, 2013
Keywords: Endoscopic sinus surgery; Cervico-facial emphysema; pneumo-mediastinum; ethical practice; medical audit; Extended indication of Endoscopic sinus surgery; CT Scan
ABSTRACT
We present a rare and unusual complication of cervico-facial soft tissue emphysema with pneumo-mediastinum which occurred in a 30-year-old female Jordanian patient in our hospital in October 2010 in Abu Dhabi following FESS. CT scan evaluation of aero-digestive tract in the immediate post-operative period was done to ascertain the cause pertaining to any surgical trauma or anaesthesia related complications. Such a case previously unreported has been included in this study. A simple close monitoring after establishing the cause is usually sufficient in management of such related or unrelated complications during FESS which in our case was likely to be anaesthesia related. Published data of such a complication assists in building up a good and effective medical audit based on ethical practice. This paper stresses the importance of immediate CT scan of aero-digestive tract in evaluating the cause.
1. Introduction
Functional endoscopic sinus surgeries like fronto-maxillo-ethmoido-sphenoidectomy or spheno-ethmoido-maxillo-frontosinusectomy are becoming a common surgical procedure in the treatment of chronic sinus diseases. This surgical technique initially developed by Stammberger and Messerklinger [1] in Austria and Wigand [2] in Germany is becoming very popular among the practicising otorhinolaryngologists of today. Various lethal and non lethal complications of FESS have been reported in the literature. Lethal complications are encountered mostly in extended indications of endoscopic sinus surgery. This paper deals with a very rare and unusual complication of cervico-facial soft tissue emphysema with pneumo-mediastinum which occurred three hours after the patient underwent minimally invasive endoscopic septoplasty, excision of right concha bullosa, left middle meatal antrostomy and anterior ethmoidectomy operation. Immediate evaluation of the cause of this complication became difficult because no such complication was previously reported in a patient after endoscopic sinus surgery. However, it has been reported in patient undergoing other non endoscopic sinus surgeries. Lack of published report of this complication in FESS surgery made it difficult to have an effective medical audit for both us operating surgeon and the anaesthetist to know whether it was a related or an unrelated complication of the primary surgery. Fortunately for us primary surgeons, an immediate CT scan evaluation of sinuses, neck and chest revealed a linear mucosal tear in the trachea at thoracic inlet level indicating the possible cause of this complication. A review of available medical literature failed to show any such documented evidence of this complication. In our opinion, this may be the first such case report of cervicofacial emphysema with pneumo-mediastinum after minimally invasive endoscopic sinus surgery with definite radiological evidence of tracheal tear.
2. Case Report
H. S. Miss, a 30-year-old young Jordanian, female patient, Hosp No. A12810/1 attended the ENT Clinic of NMC Specialty Hospital, Abu Dhabi on 14th October 2010 for complaints of frontal headache, nasal obstruction and recurrent nasal discharge. Xray PNS done revealed mucosal thickening of bilateral maxillary sinus with right septal deflection. Xray chest done was within normal limits. Prior to her ENT visit she was given a 4- month treatment for migraine by the neurologist who resulted in no significant improvement in her symptoms. She was further treated conservatively in our clinic for septal and allergic sinus disease for another 12 months with limited success. CT PNS was done on 18th September 2011 which revealed left sided maxillary sinus polyp, right sided concha bullosa with contact point and right sided septal deflection. On 26th September 2011, in view of present CT scan findings with inadequate response to conservative treatment; another neurological opinion was sought to review the status of migraine and sinus disease and change in treatment plan, if required. Therefore, it was decided that endoscopic limited FESS and septoplasty would relieve the headache and nasal block. Patient was counselled and on 2nd November 2011 she underwent excision of right concha bullosa, left middle meatal antrostomy, anterior ethmoidectomy and endoscopic septoplasty under general anaesthesia. The surgery commenced at 0928H and ended at 1058H. Patient was shifted to the ward after recovery from general anaesthesia. At 1230H, she developed an episode of severe retching, coughing and vomiting with swelling of face, neck and chest. Immediately, nasal pack was removed and CT Neck, thorax and Abdomen was done. To control the vomiting, a nasogastric tube was passed under fluoroscopic guidance and patient was kept nil per mouth and shifted to the Medical ICU (MICU). CT scan findings revealed extensive emphysema involving the soft tissue of face, neck and chest wall with significant pneumomediastinum. The air in the retropharyngeal soft tissue was causing narrowing of oropharyngeal air passage (Figures 1 and 2). A thin rim of left pneumomediastinum and extrapleural air along the posterior aspect of both lung lobes was noted (Figure 3). Focal area of thickening with linear defect in the posterior tracheal wall was found at the thoracic inlet level (Figure 4). No oesophageal leak of orally administered contrast could be seen and oesophageal tear was ruled out. Postoperative changes were noted in the sinus with intact lamina papyracea.
Patient was monitored for vital functions in MICU till 3rd November 2011 and excepting mild tachycardia and fever she was stable and doing well. She never experienced any respiratory difficulty. Patient showed remarkable improvement of swelling and was shifted to the ward the following day (4th November 2011). Patient was discharged on 7th November 2011 after an Endoscopic
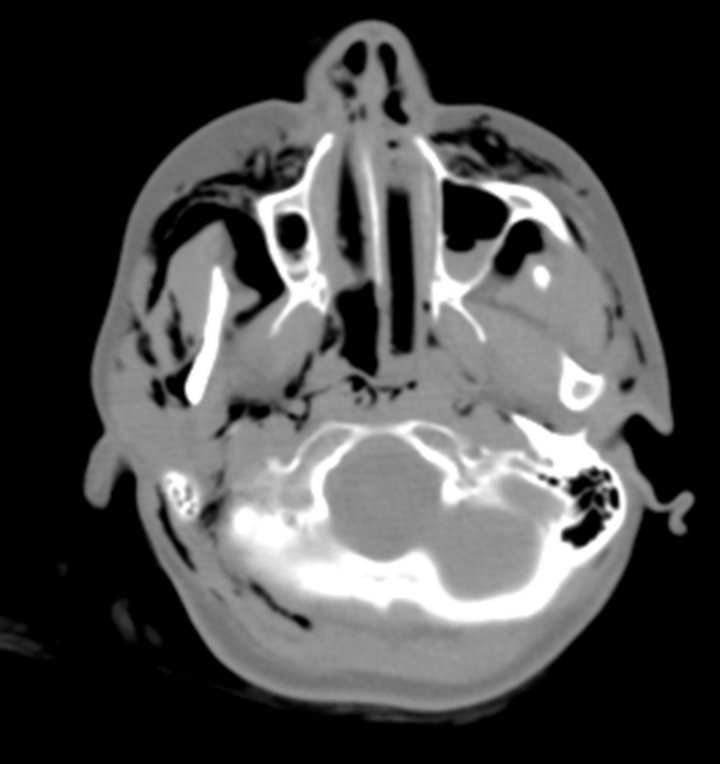

Figure 1. axial CT section of the neck showing extensive emphysema in the subcutaneous soft tissue and in the parapharyngeal and retropharyngeal spaces.
nasal cleaning and was advised to come for regular follow up on out patient basis.
3. Discussion
Functional endoscopic sinus surgery encompasses various surgical procedures ranging from simple uncinectomy and fronto-maxillo-ethmoido-sphenoidectomy to extended indication of skull base surgery. Complications arising in certain surgical procedures are related to the type of surgeries performed and the type of anaesthetic technique used. In sinus surgeries like uncinectomy,

Figure 2. Coronal reformatted CT image showing extensive emphysema in neck and axilla with significant pneumomediastinum.

Figure 3. Axial CT Section at the level of upper thorax showing extensive emphysema in the bilateral mammary region and in the superior mediastinum.
middle meatal antrostomy and anterior ethmoidectomy in an uncomplicated patient, generally patient may encounter a minor complication like lid ecchymosis, subcutaneous emphysema of lid and cheek in the immediate post operative period whereas a synechiae or a septal perforation may appear as a delayed complication. Major complications like intracerebral hemorrhage, CSF leak, blindness, diplopia, orbital hematoma, pneumoencephalocoele are more commonly seen in procedures like fronto-maxillary-ethmoido-sphenoidectomy and in extended FESS. D. H. Rice (1989) [3] and Levine (1990) [4], Ramadan and Allen (1995) [5] recorded these complications as major and minor but none have mentioned about the complication of subcutaneous emphysema of face, neck, and chest wall with pneumo-mediastinum after FESS.
Neuhaus (1990) [6], Bellamy and Berridge et al. (1993) [7] previously reported cases of subcutaneous emphy-
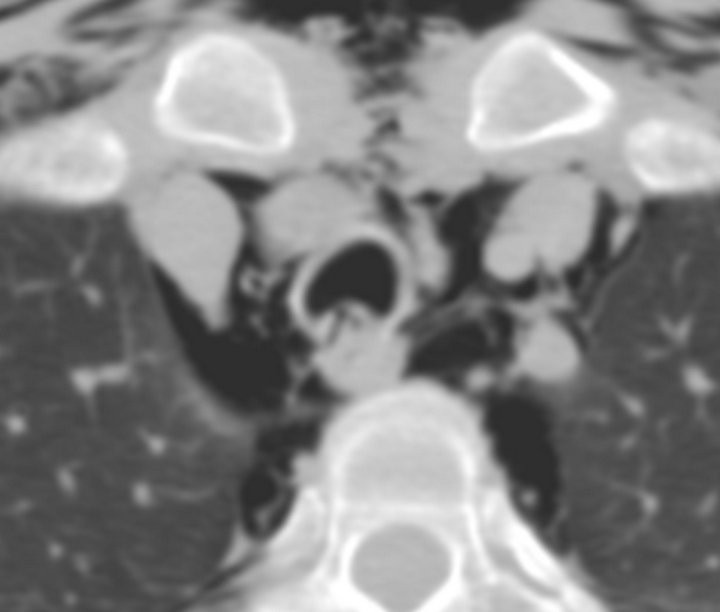
Figure 4. Axial CT Section showing a defect in the posterior tracheal wall (arrow) with extensive pneumo-mediastinum and chest wall emphysema.
sema of the face, neck and periorbital area after FESS. Various interventions have been blamed for this complication but the exact cause remains elusive. Sanu and Jayanthi et al. (2006) [8] reported another case of prevertebral surgical emphysema following FESS wherein the exact cause of it could not be established because of absence of any perforation in the aerodigestive tract. They referred to another case of Bellamy and Berridge et al. (1993) of cervico-facial emphysema which progressed rapidly to airway obstruction after stapedectomy operation under general anaesthesia where definitive pharyngeal tear and perforation was found. Since Sanu et al. could not clinically detect any aerodigestive tract injury or perforation in their case; they deduced it to be due to anatomical relations. They cited the specific anatomical relation of tubal elevation and its injury during surgery or nasal packing to be the probable cause of prevertebral emphysema in their case. However, there are no reports of such complications so far in tubal surgeries for patulous Eustachian tube. They also cited damage to another anatomical area where continuity of the lateral wall of the nose with the lateral wall of the nasopharynx lies at the posterior end of inferior and middle turbinate as being the cause of this emphysema. However, we feel that there should have been a definitive clinical or radiological evidence to support this view. Hence this view, in our opinion, is still a debatable one.
M. A. Sohail and Kishore et al. (1995) [9] first reported a case of mediastinal emphysema after endoscopic sinus surgery in a 40 year old patient having a 10-year history of recurrent bronchitis, persistent nasal discharge, headache and post nasal drip. In both of these 2 cases of emphysema (Sanu and Jyanthi et al. and M. A. Sohail and Kishore et al.), there was no evidence of injury to lamina papyracea or orbital periosteum during the surgery. Both the patients were operated under general anaesthesia. Emphysema did not occur in the immediate postoperative period but was seen 3 to several hours after the primary surgery. In our case too, facial, neck and chest emphysema developed 3 hours after the surgery initiated by severe bouts of coughing. Sanu and Jayanthi (2006) found no surgical violation of lamina papyracea or orbital periosteum and so in their case injury due to the nasal packing had been cited as the cause. In such a situation where there is no documented evidence of injury, it is difficult to build an effective medical audit based on ethical practice. In our case, an immediate CT scan of face, neck, chest and abdomen showed posterior tracheal wall injury near the thoracic inlet providing the probable cause of such extensive emphysema. Injury in the posterior tracheal wall became symptomatic after severe bouts of coughing and vice versa. All the above three cases of prevertebral and mediastinal emphysema and pneumo-mediastinum resolved after 3 to 4 days of close monitoring and management. Since these complications were reported only in a patient who underwent FESS under general anaesthesia and not local anaesthesia; violation of laryngotracheal mucosa during the anaesthetic technique should be considered as one of the causes. However, an immediate CT scan in their cases would have been ideal to confirm the trauma if present. We are also of the same opinion with Sohail and Kishore et al that the likely explanation of severe post operative emphysema in these cases is a complication of general anaesthesia procedure like intubation injury of laryngotracheal complex. Our case is backed up by definite radiological evidence to confirm our view point. The need for radiological evaluation in such scenarios cannot be overstressed for prompt diagnosis and management.
4. Acknowledgements
We, the authors acknowledge the immense help and support that we received from our NMC group medical director Dr. B. R. Shetty and Medical Director of NMC Specialty Hospital, Abu Dhabi Dr. C. R. Shetty. Dr. Sanjay Arora’s efforts have also been highly appreciated in helping of compilation of the data.
REFERENCES
- H. R. Stammberger, D. W. Kennedy and W. E. Bolger, “Paranasal Sinuses: Anatomic Terminology and Nomenclature,” Annals of Otology, Rhinology, and Laryngology, Vol. 104, 1995, pp. 7-17.
- W. Hosemann, U. Gode and M. E. Wigand, “Indications, Technique and Results of Endoscopic Ethmoidectomy,” Acta Otorhinolaryngol Belg, Vol. 47, No. 1, 1993, pp. 73- 83.
- D. H. Rice, “Endoscopic Sinus Surgery Results at 2-Year Followup,” Otolaryngology—Head and Neck Surgery, Vol. 101, No. 4, 1989, pp. 476-479.
- H. L. Levine, “Functional Endoscopic Sinus Surgery: Evaluation, Surgery and Follow-Up of 250 Patients,” Laryngoscope, Vol. 100, No. 1, 1990, pp. 79-84. doi10.1288/00005537-199001000-00016
- H. H. Ramadan and G. C. Allen, “Complication of Endoscopic Sinus Surgery in a Residency Training Program,” Laryngoscope, Vol. 105, No. 4, 1995, pp. 376-379. doi10.1288/00005537-199504000-00007
- R. W. Neuhaus, “Orbital Complications Secondary to Endoscopic Sinus Surgery,” Ophthalmology, Vol. 97, No. 11, 1990, pp. 1512-1518.
- M. C. Bellamy, J. C. Berridge and S. S. M. Hussain, “Surgical Emphysema and Upper Airways Obstruction Complicating Recovery from Anesthesia,” British Journal of Anaesthesia, Vol. 71, No. 4, 1993, pp. 592-593. doi10.1093/bja/71.4.592
- A. Sanu, N. V. G. Jayanthi and A. R. C. Mohan, “Pre- Vertebral Surgical Emphysema Following Functional Sinus Surgery,” The Journal of Laryngology & Otology, Vol. 120, No. 11, 2006, p. e38.
- M. A. Sohail, K. Kishore, H. Stammberger, J. A. Jebeles and W. Luxenberger, “Mediastinal Emphysema Associated with Functional Endoscopic Sinus Surgery,” Rhinology, Vol. 33, No. 2, 1995, pp. 111-112.
NOTES
*Corresponding author.