Open Journal of Medical Imaging
Vol.2 No.3(2012), Article ID:22675,4 pages DOI:10.4236/ojmi.2012.23017
Relationship between 18F-FDG PET SUV with Partial Volume Correction and Histology in Gastric and Gastro-Oesophageal Cancer
1Institute of Molecular Bioimaging and Physiology (IBFM)-CNR, Milan, Italy
2Nuclear Medicine Department, Hospital San Raffaele, Milan, Italy
3University of Milano-Bicocca, Milan, Italy
4Tecnomed Foundation, University of Milano-Bicocca, Milan, Italy
Email: gallivanone.francesca@hsr.it
Received July 16, 2012; revised August 15, 2012; accepted August 27, 2012
Keywords: 18F-FDG PET; SUV; Gastric Cancer
ABSTRACT
In vivo molecular imaging techniques is increasingly used in the management of oncological patients, allowing different aspects of oncological pathologies to be assessed (e.g. metabolism, hypoxia) non invasively. The possibility to extract indexes of disease from in vivo biomedical images and to associate them with their biological drivers opens new prospective on the role of in vivo molecular imaging and expedites the translation of novel biomarkers from the bench to the clinical environment. In this work we investigate the relationship between 18F-FDG uptake measured by BodyWeight Standardized Uptake Value (SUVBW) as index of cell glucose metabolism, and histological indices for gastric and gastro-oesophageal cancer. For this purpose, Partial Volume Effect Correction (PVC) has been properly compensated prior to the measurement of the PET index (PVC-SUVBW). The correlation of 18F-FDG PVC-SUVBW with histology data was evaluated by bivariate and multivariate statistical analysis. Although obtained in a limited number of patients, our results suggest that correlations can be found when PVC is applied to SUVBW and that 18F-FDG PET can provide information on biological characteristics of gastric and gastro-oesophageal cancer lesions.
1. Introduction
In vivo disease biomarkers are increasingly demanded by clinicians in order to characterize a disease, to make prognosis and to predict response to treatment non invasively.
Body-Weight Standardized Uptake Value (SUVBW), measured by Fluorodeoxyglucose and Positron Emission Tomography (18F-FDG PET), has been extensively used as semi-quantitative index accounting for altered glucose metabolism of an oncological lesion. In order to obtain an accurate measurement of 18F-FDG SUVBW, a Correction for Partial Volume Effect (PVC) has been proved mandatory, since this effect causes severe underestimation of SUVBW (up to 80% - 90% for small lesions) [1,2].
Aim of this work was to evaluate the metabolic impact of PVC on SUVBW as potential in vivo prognostic biomarker of gastric and gastro-oesophageal cancer, reflecting ex vivo histo-pathological characteristics.
2. Materials and Methods
Fourty-nine patients (31 men, 18 women; mean age 63 ± 13 years; age range: 33 - 83 years) with biopsy-proven gastric and gastro-oesophageal cancer underwent a basal 18F-FDG PET-CT study. 18F-FDG PET/CT sensitivity was assessed. Patient weight, and injected/residual dose were measured in order to calculate PVC-SUVBW on primitive gastric and gastro-oesophageal lesions detected on 18F-FDG PET images.
Patients fasted for twelve hours before the exams and were intravenous injected with 18F-FDG (1 mCi/10 kg). The PET-CT protocol began 60 minutes after the injection. All PET-CT studies were performed according to the oncological clinical protocol implemented on the discovery STE scanner, including a SCOUT scan at 40 mA, a CT scan at 140 keV and 150 mA (10 s) and 3D PET scans (2.5 min/scan) for adjacent bed positions. PET images were reconstructed by a 3D ordered subset expectation maximization algorithm (OSEM, 28 subsets, 2 iterations, 5.14 mm Gaussian post-smoothing) with corrections for random, scatter and attenuation incorporated into the iterative process.
An Operator Independent technique using an automatic threshold was used to define Regions of Interest (ROIs) on PET images [2] and quantitative analysis was performed by calculating mean SUVBW for each primitive gastric and gastro-oesophageal lesions. The RC-based correction methods developed in [2] was used to correct in order to account for Partial Volume Effect.
Both SUVBW and PVC-SUVBW were obtained by TouchSUV software [3,4].
Correlation tests (Mann-Whitney and Kruskal Wallis tests for univariate analysis and hierarchical clustering combined with a pre-processing k-means analysis for multivariate analysis) were performed in order to evaluate the relationships between 18F-FDG PVC-SUVBW and biopsy-evaluated histotype (signet ring cell carcinoma (SR), squamous cell carcinoma (S) and other adenocarcinoma (ADK) subtype) and grade (G1, G2, G3) (according to WHO and Lauren classifications).
3. Results
18F-FDG PET/CT was able to detect gastric and gastrooesophageal cancer with a sensitivity of 82%: 18F-FDG PET/CT images of 9 (18%) biopsy-proven gastric cancers were classified as negative, showing no 18F-FDG uptake in the primitive lesions. Negative PET images were not quantified and were excluded by correlation analysis.
Mean primitive lesion diameter (sphere-equivalent diameter) was 2.15 ± 1.17 cm, ranging from 0.99 cm to 6.25 cm. Lesion size confirmed the need of PVC for accurate PET quantification for more than 75% of lesions [2].
Signet ring cell carcinomas showed a lower 18F-FDG PVC-SUVBW compared to squamous cell carcinomas and to other adenocarcinoma subtypes (PVC-SUVBW: 5.57 ± 3.22 g/cc vs 9.90 ± 1.91 g/cc vs 9.32 ± 4.26 g/cc; Mann-Whitney test, p < 0.05). No correlation was found when PVC was not applied to SUVBW.
No correlations were found between grade and 18FFDG PVC-SUVBW or 18F-FDG SUVBW (Kruskal Wallis test, p > 0.05).
Figure 1 shows the results for univariate analysis.
The pre-processing k-means cluster analysis allowed to stratify patients in three different groups on the basis of PVC-SUVBW (PVC-SUVBW ≤ 6.25 g/cc; 6.25g/cc < PVC-SUVBW < 11.60 g/cc; PVC-SUVBW ≥ 11.60 g/cc). Using these groups, the hierarchical cluster analysis performed on PVC-SUVBW, histotype and grade showed that poorly differentiated (G3) signet ring cell carcinomas were significantly associated with 18F-FDG PVCSUVBW ≤ 6.25 g/cc (p < 0.05), while moderately differentiated (G2, G1) squamous cell carcinoma were significantly associated with 18F-FDG PVC-SUVBW > 11.6 g/cc; (p < 0.05).
Figure 2 shows the results of the hierarchical cluster analysis.
4. Discussion
The role of 18F-FDG PET in staging gastric and gastroesophageal cancer is controversial. Some works showed a good sensitivity (94%) in the detection of primary gastric and gastro-oesophageal lesions [5], while other studies softened the impact of 18F-FDG PET [6] highlighting in particular its low sensitivity for signet-ring cells carcinomas [7].
In current clinical practice, the election modalities for gastric and gastro-oesophageal cancer remains Endoscopic Ultrasound (EUS) and Computerized Tomography (CT), even if 18F-FDG PET has been suggested in the work-up of patients with incomplete staging as obtained by EUS [5,6] and for detection of distant metastases.
Although obtained in limited population of patients with gastric and gastro-oesophageal cancer, our results show that PVC-SUVBW can have a prognostic role for those lesions detected by 18F-FDG PET.
In literature, few works have been devoted to investigate the relationship between 18F-FDG uptake, as detected
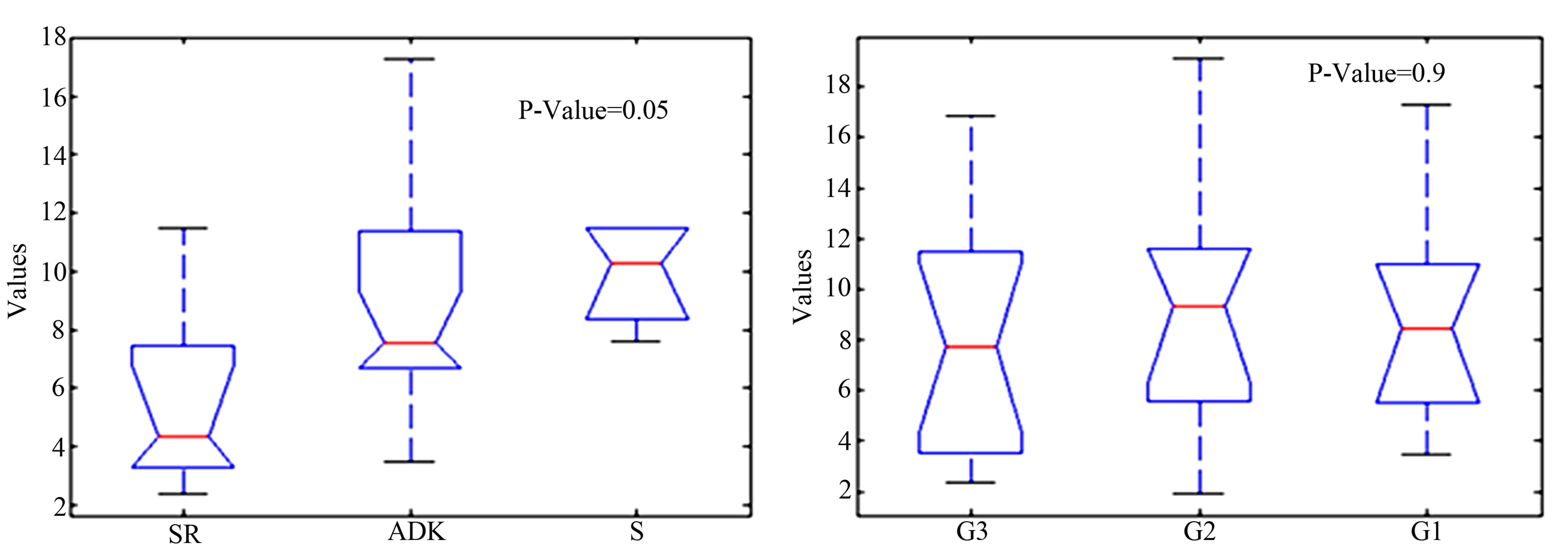
Figure 1. Results of bi-variate tests on histological type and grade.
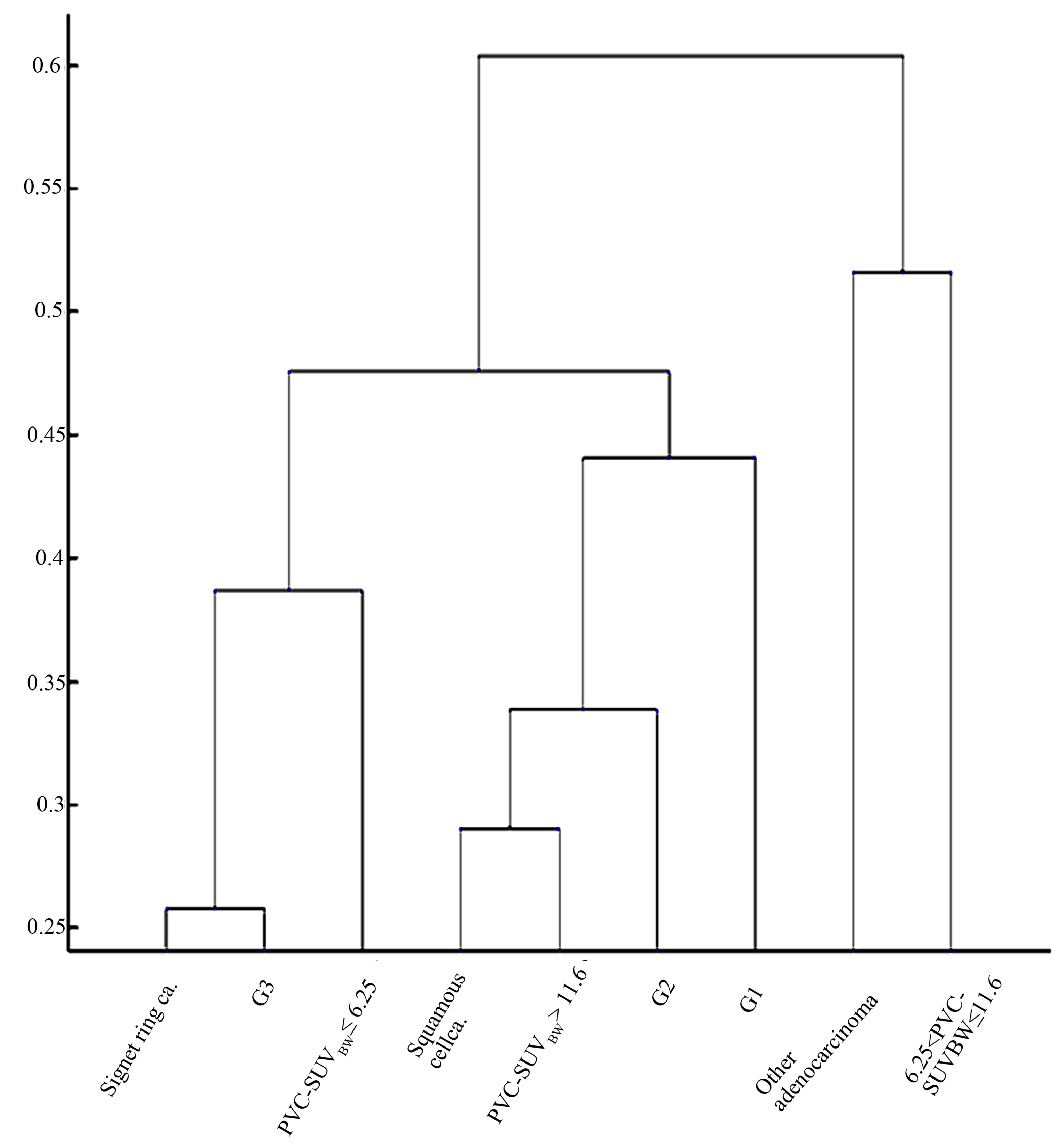
Figure 2. Results of hierarchical cluster analysis.
and measured by PET, and tumour biological characteristics of gastro-oesophageal lesions [8,9]. In published studies no correction for PVC has been used prior to the measurement of 18F-FDG uptake. No correlation was found between 18F-FDG uptake and the differentiation grade [9], neither between 18F-FDG uptake and histological type [8], as obtained in our work when PVC was not applied to SUVBW.
Results of our work suggest that correlations can be found when PVC is applied.
Our work gives added value to current evidences on the role of 18F-FDG in gastric and gastro-oesophageal cancer in adopting, for the first time at our knowledge, two strategies: 1) the application of PVC for the accurate measurement of 18F-FDG SUVBW of small lesions and 2) the use of a multivariate hierarchic cluster analysis combined to a k-means pre-clustering approach for multiple correlations.
Our results need to be validated on a larger cohort of patients.
5. Conclusion
18F-FDG PET can provide information on biological characteristics of gastric and gastro-oesophageal cancer by means of 18F-FDG SUV on condition that partial volume correction is properly applied prior to the measurement of PET quantification indexes.
REFERENCES
- M. Soret, S. L. Bacharach and I. Buvat, “Partial-Volume Effect in PET Tumor Imaging,” Journal of Nuclear Medicine, Vol. 48, No. 6, 2007, pp. 932-945. doi:10.2967/jnumed.106.035774
- F. Gallivanone, A. Stefano, C. Canevari, L. Gianolli, C. Messa, M. C. Gilardi and I. Castiglioni, “PVE Correction in PET-CT Whole-Body Oncological Studies from PVEAffected Images,” IEEE Transactions on Nuclear Science, Vol. 58, No. 3, 2011, pp. 736-747. doi:10.1109/TNS.2011.2108316
- I. Castiglioni, F. Gallivanone and A. Stefano, “TOUCH SUV, SIAE Registration No 007449-D006667,” 2009.
- A. Stefano, F. Gallivanone, E. Grosso, G. Russo, C. Messa, V. Tripoli, M. C. Gilardi and I. Castiglioni “TOUCHSUV: A Touchscreen-Assisted Tool for Quantitative, Reproducible, Clinically Feasible and Collaborative Diagnostic Reporting of Whole-Body PET-CT Studies,” Software Engineering, Vol. 1, No. 1, 2011, pp. 1-8.
- W. L. Wong and R. J. Chambers, “Role of PET/PET CT in the Staging and Restaging of Thoracic Oesophageal Cancer and Gastro-Oesophageal Cancer: A Literature Review,” Abdominal Imaging, Vol. 33, No. 2, 2008, pp. 183-190. doi:10.1007/s00261-007-9241-1
- G. Lucignani, “Oesophageal Cancer: Can Imaging Improve Its Assessment?” European Journal of Nuclear Medicine and Molecular Imaging, Vol. 35, No. 10, 2008, pp. 1921-1927. doi:10.1007/s00259-008-0884-0
- T. K. Ha, Y. Y. Choi, S. Y. Song and S. J. Kwon, “F18- Fluorodeoxyglucose-Positron Emission Tomography and Computed Tomography Is Not Accurate in Preoperative Staging of Gastric Cancer,” Journal of the Korean Surgical Society, Vol. 81, No. 2, 2011, pp. 104-110. doi:10.4174/jkss.2011.81.2.104
- H. Miyata, Y. Doki, T. Yasuda, M. Yamasaki, I. Higuchi and Y. Makari, “Evaluation of Clinical Significance of 18F-Fluorodeoxyglucose Positron Emission Tomography in Superficial Squamous Cell Carcinomas of the Thoracic Esophagus,” Diseases of the Esophagus, Vol. 21, No. 2, 2008, pp. 144-150. doi:10.1111/j.1442-2050.2007.00743.x
- M. Westerterp, G. W. Sloof, O. S. Hoekstra, F. J. T. Kate, G. A. Meijer and J. B. Reitsma, “18FDG Uptake in Oesophageal Adenocarcinoma: Linking Biology and Outcome,” Journal of Cancer Research and Clinical Oncology, Vol. 134, No. 2, 2008, pp. 227-236. doi:10.1007/s00432-007-0275-0