World Journal of Cardiovascular Diseases
Vol.05 No.04(2015), Article ID:55703,7 pages
10.4236/wjcd.2015.54012
Comparison of the Modified Eversion Carotid Endarterectomy Technique with the Conventional Carotid Endarterectomy Technique: Early Results
Burcin Abud1*, Süreyya Talay2, Celal Selcuk Ünal3, Emre Kubat3, Kemal Karaarslan1, Soysal Turhan1
1Cardiovascular Surgery Department, Izmir Tepecik Research and Teaching Hospital, Izmir, Turkey
2Cardiovascular Surgery Department, Canakkale State Hospital, Izmir, Turkey
3Cardiovascular Surgery Department, Karabük University Research and Teaching Hospital, Karabük, Turkey
Email: *burcinabud@hotmail.com
Copyright © 2015 by authors and Scientific Research Publishing Inc.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/



Received 22 March 2015; accepted 10 April 2015; published 15 April 2015
ABSTRACT
Objectives: In this study, we aimed to compare early results of the modified eversion carotid endarterectomy technique with the conventional carotid endarterectomy technique. The modified eversion carotid endarterectomy technique consisted of a longitudinal arteriotomy that was begun from the common carotid artery proximally to the origin of external carotid artery. We also avoided applying a carotid shunt during surgery in both techniques. Methods: Each patient was evaluated for coronary artery stenosis and valve replacement indications. Diagnosis of significant coronary artery stenosis or valve disease directed us to a combination of CEA and cardiac surgery (CABG/Valvular). We generally had a tendency to perform these two surgical procedures separately. Patients which had surgery for both at the same session were excluded in this study. As a result, our study included 120 patients and 137 carotid interventions. We performed the modified eversion carotid endarterectomy technique in 61 patients (68 carotid interventions) (Group A) and the conventional CEA technique in 59 patients (69 carotid interventions) (Group B). At follow-up, the patients were evaluated by physical examination and color Doppler USG. Results: There was no significant difference between the groups in terms of demographic data. Statistically significant difference was observed in one operative parameter between Group A and Group B; patchplasty requirements during surgery (12 carotid interventions in group B and 4 carotid interventions in group A, p = 0.036). We recorded temporary tongue deviation in five cases, facial asymmetry in eight cases, hoarseness in four cases, neurocognitive impairment in three cases and transient neurologic in two cases with no significant difference between the groups. There was in one case of permanent neurologic deficit (1 in group B). There were two postoperative deaths (1 in group A and 1 in group B). The death in group A occurred because of subarachnoid haemorrhage and the death in group B occurred because of myocardial infarction. After 6 month follow-up, no restenosis occurred in group A. Restenosis occurred in three patients of group B. Conclusion: The modified eversion technique for carotid endarterectomy decrease the incidence of patchplasty applications and postoperative restenosis by avoiding internal carotid artery manipulation and sewing. Besides, it is easy and possible to remove plaques completely from internal carotid artery via the modified arteriotomy line.
Keywords:
Conventional Carotid Endarterectomy, Modified Eversion Carotid Endarterectomy Technique, Avoiding Carotid Shunt

1. Introduction
Several modifications are presented for carotid endarterectomy procedure since the first describes surgical resection and anastomosis report in 1954 by Eastcott, Pickering and Rob [1] . A lot of studies have documented that surgical treatment is superior to medical treatment in patients with significant carotid stenosis. The North American Symptomatic Carotid Endarterectomy Trial (NASCET) has showed the superiority of the surgical treatment in symptomatic patients with carotid stenosis [2] . Likewise, the Asymptomatic Carotid Atherosclerosis Study (ACAS) and the Asymptomatic Carotid Surgery Trial (ACST) have showed the superiority of the surgical treatment in asymptomatic patients with significant carotid stenosis [3] [4] .
There are two main surgical techniques in carotid endarterectomy (CEA): the eversion technique and the conventional technique. We prefer to use a modified eversion technique, which consists of a longitudinal arteriotomy from the common carotid artery to the origin of external carotid artery. Besides, we also avoid applying a carotid shunt. In this study, we evaluate early results of this modified eversion carotid endarterectomy technique and compare this result with results of the conventional carotid endarterectomy technique without shunt application.
2. Material and Methods
All cases were evaluated by color Doppler ultrasonography (USG) and formal angiography. Our surgical indications were mainly based on the NASCET and ACAS/ACST guidelines [2] -[4] . We operated cases for symptomatic clinical presentations in 50% or more luminal carotid stenosis. In asymptomatic patients angiographically more than 70% stenosed or 60% - 70% ulcerated common or internal carotid arteries were defined as operative indications. Each patient was evaluated for coronary artery stenosis and valve replacement indications. Diagnosis of significant coronary artery stenosis or valve disease directed us to a combination of CEA and concomitant cardiac valve operations and/or coronary artery bypass grafting (CABG). We generally had a tendency to perform these two surgical procedures separately. Patients which had surgery for both at the same session were excluded in this study.
As a result, our study included 120 patients and 137 carotid interventions. 62 of them had right, 41 had left CEA and 17 patients had bilateral CEA. The patients with bilateral CEA underwent contralateral intervention 10 to 30 days after the first intervention. 6 patients had complete occlusion of the contralateral carotid artery, 2 revealed not significant (<70%) unilateral vertebral artery stenosis. No intervention was performed on the patients with completely occluded carotid arteries or vertebral artery stenosis.
We performed the modified eversion carotid endarterectomy technique in 61 patients (68 carotid interventions) (Group A) and the conventional CEA technique in 59 patients (69 carotid interventions) (Group B). The choice of the procedure was made without criteria.
Significant coronary artery disease was present in 23 patients and significant valve disease was present in three patients. Additional cardiac surgery (CABG/Valvular) was performed in these patients 5 days after CEA.
Preoperative demographic data were recorded after obtaining the patient’s medical histories and performing physical examination. At follow-up the patients were evaluated by physical examination and color Doppler USG.
3. Surgical Procedures
All patients obtained the same premedication with Propofol 2 - 3 mg/kg, Fentanyl Citrate 10 - 15 microgr/kg and Pancuronium bromid 0.1 mg/kg. Following endotracheal intubation, anesthesia maintenance dose included Propofol 2 - 5 mg/kg/h and Fentanyl Citrate 5 - 10 microgr/kg/h intravenously. Inhaled anesthesia continued with Sevoflurane. Before the application and after the removal of the carotid cross clamp, we administered 8 mg dexamethasone.
Group A was consisted of the modified CEA cases without shunt applications in a total number of 61 patients. All operations were performed under general anesthesia. Classical incision medial to the sternocleidomastoid muscle was used for exposure of the carotid arteries. All dissections were performed by using low voltage electrocautery and surgical loops with 3.5 - 4.5 magnification. Carotid tree was completely dissected free. ICA dissection was extended to expose a segment of artery 0.5 cm distal to the end-point of the atherosclerotic plaque to allow a loop occlusion. Following this phase of our modified procedure, 15,000 IU of heparin was administered. Vascular clamp was applied only to the common carotid artery (CCA). For internal and external carotid artery occlusion, silastic loops, doubly passed around the vessels, were used. A longitudinal arteriotomy at the medial side of the CCA was made and extended to the external carotid artery (ECA) by means of medial or anterior aspect (Figure 1). After the creation of the endarterectomy plane on both sides, the plaque was freed from the ECA and its branches. Later, the plaque was cut free at its proximal end-point in the CCA and freed further with blunt dissection towards internal carotid artery (ICA). At this stage, only the ICA part of the plaque remained attached. While the first assistant gently everting the ICA by using two forceps, plaque was freed circumferentially until the end-point and removed (Figure 2). After irrigation and cleaning of the debris, arteriotomy was closed primarily by using 6/0 polypropylene suture.
Group B was consisted of conventional CEA without shunt application in a total number of 59 patients. An identical exposure was obtained in this group of patients. 15,000 IU of heparin was administered. Vascular clamp was applied only to the common carotid artery CCA. For internal and external carotid artery occlusion, silastic loops, doubly passed around the vessels, were used. Arteriotomy was extended from the CCA to the ICA. ECA was occluded by silastic vascular loops. After removal of plaque de-airing maneuvers, surgical closure was performed by the same technique as described above for Group A.
In both procedures, during cross clamping we kept the systolic blood pressure at 120 - 140 mmHg to provide adequate perfusion from the collateral circulation to maintain basal cerebral viability (collateral circulation from the contralateral carotid artery and vertebral arteries) [5] .
Antiplatelet therapy was given during preoperative and postoperative periods, and all of the patients were prescribed acetylsalicylic acid (150 mg oral/daily).
Statistical Analysis
All the data obtained in this study were analyzed using the Statistical Package for the Social Sciences for Windows (SPSS Inc., Chicago, Illinois, USA) version 16.0. Data were expressed as proportions or as the mean ± standard deviation. For comparisons between the two groups, Chi square test and Fisher’s exact test was used for the nominal data, while numerical data were compared using Mann-Whitney U test. A p value less than 0.05 (p < 0.05) was considered statistically significant.
4. Results
This study included 61 patients (26 female and 35 male) 68 carotid interventions in group A and 59 patients (27 female and 32 male) 69 carotid interventions in group B. There was no significant difference between the groups in terms of demographic characteristics, independent risk factors, concomitant surgery and significant (≥70%) contralateral carotid artery stenosis (Table 1).
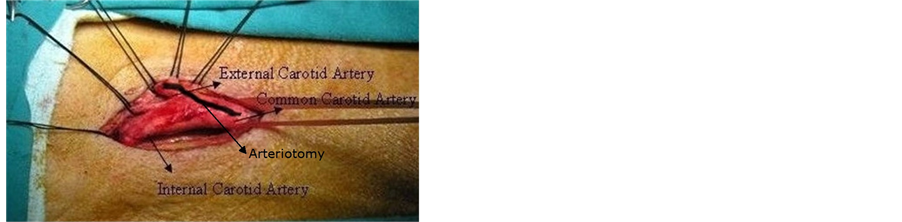
Figure 1. Dissection of carotid system branches and description of our modified arteriotomy line from CCA to ECA.
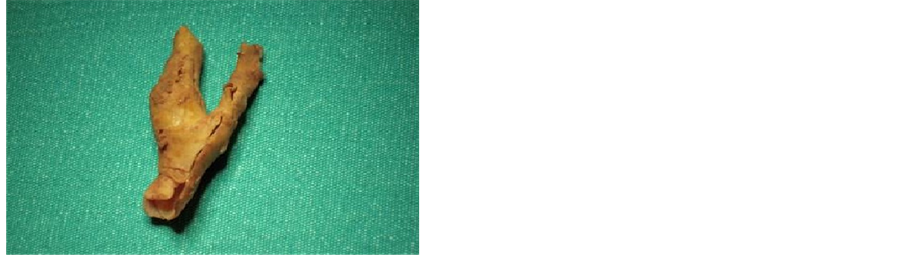
Figure 2. Removed atherosclerotic plaque in the modified eversion CEA technique.

Table 1. Preoperative patients data and demographics.
COPD: Chronic obstructive pulmonary disease, DM: Diabetes mellitus, HT: Hypertension, PAD: Peripheral artery disease, CABG: Coronary artery bypass graft, CAS: Carotid artery stenosis.
Table 2 depicts our perioperative data including intraoperative parameters. Statistically significance was observed in one different operative parameter between Group A and Group B; patchplasty requirements during surgery.
We recorded temporary tongue deviation in five cases (2 from group A and 3 from group B) and facial asymmetry in eight cases (3 from group A and 5 from group B) which we believe to be related with N. Hypoglossus injuries. These postoperative complications were treated with intravenous and perorally steroids. Hoarseness was observed in four cases (2 from group A and 2 from group B). This may have been due to recurrent laryngeal nerve injury or endotracheal intubation. We observed psychotic symptoms with delirium (neurocognitive impairment) in three cases (1 from group A and 2 from group B). Transient neurologic attack was observed in two cases (1 from group A and 1 from group B). There was in one case of permanent neurologic deficit (1 in group B) (Table 3).
There were two postoperative deaths (1 in group A and 1 in group B). The death in group A occurred because of subarachnoid haemorrhage and the death in group B occurred because of myocardial infarction. The latter patient was a candidate for CABG after CEA. After 6 month follow-up, no restenosis occurred in group A. Restenosis occurred in three patients of group B (Table 3).
5. Discussion
Cerebrovascular disease and associated stroke are the third most frequent reason of deaths. These conditions are also the main source of neurological deaths. Cerebrovascular events (CVE) are related with ischemia in 80% of cases and haemorrhage in 20%. Elaboration of this latter data shows that ischemia related CVE patients also have severe carotid system stenosis in 50%. Furthermore, 90% of this carotid system stenosis is resulted by extracranial atherosclerosis. Rest of the carotid stenosis in 10% percentage is associated with aneurysms, arteritis, carotid dissection, radiation, vasospasm and infective diseases. Yearly stroke incidence is reported to be approximately 160 cases in a 100,000 population [2] -[4] .
Table 2. Patients operative data.
CCT: Cross clamp time.
Table 3. Postoperative complications (6 month follow-up).
Extracranial carotid artery is recognized and named by ancient Greeks with the term of “Karoo” which means “to stupefy”. First medical literature for carotid occlusion was also defined in 1875 by Growers for a patient with right hemiplegia. Hunt pointed out the relationship between carotid disease and stroke by his original term of “cerebral intermittent claudication” [6] . Operative considerations especially took place with a higher accuracy by DeBakey in 1975 [7] . He reported his experience on this subject in a 19 year follow-up via his series of CEA.
Our surgical indications were mainly based on the NASCET and ACAS/ACST guidelines [2] -[4] . We operated cases for symptomatic clinical presentations in 50% or more luminal carotid stenosis. In asymptomatic patients angiographically more than 70% stenosed or 60% - 70% ulcerated common or internal carotid arteries were defined as operative indications. Patients mostly presented their symptoms by transient visual losses, transient ischemic attacks, minor strokes and strokes with several degrees of muscle strength losses from mild paresthesia to hemiplegia. We also preferred medical therapy over surgery in cases with concurrent life threatening general diseases, occluded carotid system with recent severe neurologic deficit and cerebral infarction. We did not accepted carotid doppler USG alone for surgical decision, we preferred to continue with carotid magnetic resonance angiography or conventional angiography before surgery in every case.
Conventional technique of endarterectomy is carried out in the media of CCA with a partial end-point on ICA [8] . In the majority of cases, this arteriotomy is sutured either primarily or with a Dacron patch. Perioperative mortality rate, stroke, cranial nerve injury with symptoms of hypoglossal and recurrent laryngeal nerve injuries are the most frequently reported complications after surgery [9] [10] . Re-stenosis may occur in 1% - 20% of cases which is believed to be in correlation with the cumulative risk of a serious ipsilateral stroke risk in 9% [11] . As a general aspect, surgical results are favorable when compared to medical treatment and/or angioplasty- stenting in this group of patients.
The modified eversion techique is a modification over conventional CEA procedure by avoiding intraluminal carotid shunt and with an arteriotomy which stands over the proximal portion of ECA rather than ICA. In our study, in the “modified eversion” group, there were statistically significant differences on behalf of Group A by one operative parameter such as less need for patchplasty closure.
Operation length was 49.5 ± 21.8 minutes for Group A 45.3 ± 11.2 minutes for group B. Cranial nerve injury was observed in 17 cases postoperatively. 10 of these cases were from group B with a rate of 14.5% which was a little bit higher than the rate of Group A with 10.3%.
We strongly believe that the modified eversion technique present several advantages for reducing postoperative neurologic complications by lesser ICA manipulation.
Several studies have reported that carotid artery surgery could be performed safely without using a shunt despite the presence of contralateral carotid artery lesions and low stump pressure. This studies reported that during cross clamping the collateral circulation from the contralateral carotid artery and vertebral arteries would provide adequate perfusion of the brain [5] [12] [13] . In our study, we avoided applying a shunt in both groups. During carotid cross clamping we kept the systolic blood pressure at 120 - 140 mmHg to provide adequate perfusion from the collateral circulation. We believe that shorter cross clamp time may directly influence postoperative neurological conditions especially for cases with bilateral carotid stenosis in different degrees. Our average cross clamp time in Group A was 17.6 ± 7.2 minutes and in group B it was 15.2 ± 8.1 minutes, which we believe to be safe even in the absence of a carotid shunt to continue cerebral flow during surgery.
Patchplasty requirements were significantly higher in Group B (12 carotid interventions, 17.3%) when compared to Group A (4 carotid interventions, 5.9%, p = 0.036). From our point of view, modified eversion technique reduced patchplasty requirements after endarterectomy.
Debate on the use of patchplasy for CEA is controversial in the medical literature. Luminal diameter shorter than 4 mm is generally accepted as an indication for patchplasy in several studies [14] -[16] . For instance, Rock- man et al. [17] reported a significant elevation in stroke and mortality incidence by applications of primary closure of arteriotomy when compared to eversion and patchplasy, 6% to 2.5%, respectively. In their series of 1972 cases, they pointed out that these complication rates were identical by eversion and patchplasty techniques by 2.5%. On the contrary, Rizzo et al. [18] reported a serious infection risk for dacron patchplasty applications. He also stated by his study that a higher incidence of re-stenosis was a part of this infective complication. Our clinical preference was parallel to Rizzo et al. We advocated that closure of arteriotomy without patchplasty and avoiding possible complications as re-stenosis were atmost beneficial for the patients which could be achieved by eversion administrations [19] [20] . Katras and his co-workers [21] finalized their manuscript by a similar conclusion. He paraphrased that CEA technique of choice was to be eversion methods over patchplasty and primary closure for higher patency rates and lower complication incidence. With this eversion technique, their perioperative major stroke and mortality rates were 2.5%.
Carotid system atherosclerosis occurs in various localizations. Spread percentages are 9% for aortic arcus, 20% for vertebral artery, 33% at intracranial side and 38% on carotid bifurcation [22] [23] . Our clinical observation supports a higher frequency for carotid bifurcation incidence among these patients. Furthermore, we strongly believe that an arteriotomy incision from CCA to ECA allows a surgeon to remove atherosclerotic plaque completely from carotid bifurcation in both proximally and distally sides. A suture line towards the origin of ECA by avoiding ICA involvement clearly reduces the risk of postoperative incision line fibrosis and re-stenosis for ICA branch. Our postoperative evaluations by doppler USG proved these foresights to be correct over ICA patency. Another advantage of this modified technique is the possibility to achieve a complete removal of atherosclerotic plaques from ECA side. This presents a secondary benefit which is a certain elevation of the blood flow through the collateral connections from ECA to ICA. Besides, the modified eversion technique also reduces surgical manipulations to ICA.
6. Conclusion
The modified eversion technique for carotid endarterectomy which consists of a combination of “not to shunt” choice and arteriotomy incision from common carotid artery to external carotid artery may decrease the incidence of patchplasy applications and postoperative restenosis by avoiding internal carotid artery manipulation and sewing. Besides, we believe that it is almost always easy and possible to remove plaques completely from internal carotid artery via the modified arteriotomy line.
Limitations of This Study
The small number of patients in the study may not prove that the modified eversion technique suggests a better longterm clinical outcome. We need to point out the postoperative differences between Group A and Group B in a more elaborate data and longer postoperative period. Restenosis ratios may increase in long-term follow-up in our cases.
Competing Interests
The authors declare that they have no competing interests.
Authors’ Contributions
BA, ST, CSÜ designed the study. BA, ST, KK and CSÜ carried out studies searching and performed the eligibility assessments. ST, EK evaluated the qualities of the included studies and carried out data extracting. BA, ST analyzed and interpreted the data. BA, ST, KK drafted the manuscript. BA, ST, EK made critical revision of the manuscript for important intellectual content. All authors read and approved the final manuscript.
References
- Eastcott, H.H., Pickering, G.W. and Rob, C.G. (1954) Reconstruction of Internal Carotid Artery in a Patient with Intermittent Attacks of Hemiplegia. Lancet, 264, 994-996. http://dx.doi.org/10.1016/S0140-6736(54)90544-9
- Barnett, H., Taylor, W., Eliasziw, M., Fox, A.J., Ferguson, G.G., Haynes, R.B., et al. (1998) Benefit of Carotid Endarterectomy in Patients with Symptomatic Moderate or Severe Stenosis. North American Symptomatic Carotid Endarterectomy Trial Collaborators. The New England Journal of Medicine, 339, 1415-1425. http://dx.doi.org/10.1056/NEJM199811123392002
- Walker, M.D., Marler, J.R., Goldstein, M., Grady, P.A., Toole, J.F., Baker, W.H., et al. (1995) Executive Committee for the Asymptomatic Carotid Atherosclerosis Study. Endarterectomy for Asymptomatic Carotid Stenosis. The Journal of the American Medical Association, 273, 1421-1428. http://dx.doi.org/10.1001/jama.1995.03520420037035
- Halliday, A., Mansfield, A., Marro, J., Peto, C., Peto, R., Potter, J., et al. (2004) MRC Asymptomatic Carotid Surgery Trial (ACST) Collaborative Group. Prevention of Disabling and Fatal Strokes by Successful Carotid Endarterectomy in Patients without Recent Neurological Symptoms; Randomized Controlled Trial. Lancet, 363, 1491-1502. http://dx.doi.org/10.1016/S0140-6736(04)16146-1
- Ott, D.A., Cooley, D.A., Chapa, L. and Coelho, A. (1980) Carotid Endarterectomy without Temporary Intraluminal Shunt. Study of 309 Consecutive Operations. Annals of Surgery, 191, 708-713. http://dx.doi.org/10.1097/00000658-198006000-00008
- James, A.L., Carl, E. and Jeffry, P.E. (1985) Vertebrobasilar İnsufficiency. Archives of Neurology, 42, 803-808. http://dx.doi.org/10.1001/archneur.1985.04210090071021
- DeBakey, M.E. (1975) Successful Carotid Endarterectomy for Cerebrovascular İnsufficiency. The Journal of the Ameri- can Medical Association, 233, 1083-1085. http://dx.doi.org/10.1001/jama.1975.03260100053020
- Khiatan, L., Sutter, F.P. and Goldman, S.M. (2000) Simultaneous Carotid Endarterectomy and Coronary Revasculari- zation. The Annals of Thoracic Surgery, 69, 421-424. http://dx.doi.org/10.1016/S0003-4975(99)01288-6
- Palombo, D., Lucertini, G., Mambrini, S. and Zettin, M. (2007) Subtle Cerebral Damage after Shunting vs Nonshunting during Carotid Endarterectomy. European Journal of Vascular and Endovascular Surgery, 34, 546-551. http://dx.doi.org/10.1016/j.ejvs.2007.05.028
- Stewart, G., Ross-Russell, R.W. and Browse, N.L. (1986) The Long-Term Results of Carotid Endarterectomy for Transient Ischemic Attacks. Journal of Vascular Surgery, 4, 600-605. http://dx.doi.org/10.1016/0741-5214(86)90176-X
- Rubin, J.R., Goldstone, J., McIntyre Jr., K.E., Malone, J.M. and Bernhard, V.M. (1986) The Value of Carotid Endarte- rectomy in Reducing the Morbidity and Mortality of Recurrent Stroke. Journal of Vascular Surgery, 4, 443-449. http://dx.doi.org/10.1016/0741-5214(86)90378-2
- Boontje, A.H. (1994) Carotid Endarterectomy without a Temporary Indwelling Shunt: Results and Analysis of Back Pressure Measurements. Cardiovascular Surgery, 2, 549-554.
- Samson, R.H., Showalter, D.P. and Yunis, J.P. (1998) Routine Carotid Endarterectomy without a Shunt, Even in the Presence of a Contralateral Occlusion. Cardiovascular Surgery, 6, 475-484. http://dx.doi.org/10.1016/S0967-2109(98)00018-0
- Hertzer, N.R., Beven, E.G., O’Hara, P.J. and Krajewski, L.P. (1987) A Prospective Study of Vein Patch Angioplasty during Carotid Endarterectomy: Three-Year Results for 801 Patients and 917 Operations. Annals of Surgery, 208, 628- 635. http://dx.doi.org/10.1097/00000658-198711000-00013
- Mackey, W.C., Khabbaz, K. and Bojar, R. (1996) Simultaneous Carotid Endarterectomy and Coronary Artery Bypass: Perioperative Risk and Long Term Survival. Journal of Vascular Surgery, 24, 58-64. http://dx.doi.org/10.1016/S0741-5214(96)70145-3
- Loftus, C.M. (2007) Historical Perspective on Carotid Reconstruction. Carotid Endarterectomy Principles and Technique. 2nd Edition, Informa Healthcare, New York, 1-46.
- Rockman, C.B., Halm, E.A., Wang, J.J., Chassin, M.R., Tuhrim, S., Formisano, P. and Riles, T.S. (2005) Primary Clo- sure of the Carotid Artery İs Associated with Poorer Outcomes during Carotid Endarterectomy. Journal of Vascular Surgery, 42, 870-877. http://dx.doi.org/10.1016/j.jvs.2005.07.043
- Rizzo, A., Hertzer, N., O’Hara, P., Krajewski, L. and Beven, E. (2000) Dacron Carotid Patch İnfection: A Report of Eight Cases. Journal of Vascular Surgery, 32, 602-606. http://dx.doi.org/10.1067/mva.2000.107567
- Kieny, R., Hirsch, D., Seiller, C., Thiranos, J.C. and Petit, H. (1993) Does Carotid Eversion Endarterectomy and Reimplantation Reduce the Risk of Restenosis? Annals of Vascular Surgery, 7, 407-413. http://dx.doi.org/10.1007/BF02002123
- Bosse, A., Ansorg, P., Mayer, B. and Mulch, J. (1991) Eversion Endarteriectomy of the İnternal Carotid Artery. The Thoracic and Cardiovascular Surgeon, 39, 371-375. http://dx.doi.org/10.1055/s-2007-1020002
- Katras, T., Baltazar, U., Rush, D.S., Sutterfield, W.C., Harvill, L.M. and Stanton Jr., P.E. (2001) Durability of Eversion Carotid Endarterectomy: Comparison with Primary Closure and Carotid Patch Angioplasty. Journal of Vascular Surgery, 34, 453-458. http://dx.doi.org/10.1067/mva.2001.117885
- Bernhard, V.M., Johnson, W.D. and Peterson, J.J. (1972) Carotid Artery Stenosis. Archives of Surgery, 105, 837-840. http://dx.doi.org/10.1001/archsurg.1972.04180120018005
- Imparato, A.M., Riles, T.S. and Gorstein, F. (1979) The Carotid Bifurcation Plaque: Pathologic Findings Associated with Cerebral İschemia. Stroke, 10, 238-245. http://dx.doi.org/10.1161/01.STR.10.3.238
NOTES

*Corresponding author.