Open Journal of Therapy and Rehabilitation
Vol.02 No.02(2014), Article ID:46392,9 pages
10.4236/ojtr.2014.22012
Auditory P300 as an Indicator in Effectiveness of Robot-Assisted Lower Limb Rehabilitation Training among Hemiplegic Patients after Ischemic Stroke
Yaning Zhao1*, Zhengwei Hao1,2, Jianmin Li3
1College of Nursing and Rehabilitation, Hebei United University, Tangshan, China
2People’s Hospital of Tangshan, Tangshan, China
3Affiliated Hospital of Hebei United University, Tangshan, China
Email: *zyning789@126.com
Copyright © 2014 by authors and Scientific Research Publishing Inc.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/



Received 19 February 2014; revised 27 March 2014; accepted 5 April 2014
ABSTRACT
Background: Robot-assisted lower limb rehabilitation training in early stage could improve the limb function among hemiplegic patients caused by ischemic stroke. P300 potential changes have importantly clinical value for evaluating the improvement in nerve function during the training as one of the objective targets. Methods: Sixty hemiplegic patients after stroke were randomly divided into a Lokomat group (30 cases) and a control group (30 cases). The Lokomat group received Lokomat rehabilitation while the control group only received traditional rehabilitation. The gait parameters and the balance ability were evaluated by the K421GAITRite analysis system and the Berg Balance Scale (BBS); ERP components including N100, N200, P200 and P300 potential were evaluated by a muscle electric inducing potentiometer. Results: There were no significant differences in BBS and gait parameters (P > 0.05), as well as in amplitude and incubation periods (IP) (P > 0.05) between the two groups before training. After 8 weeks treatment, the total (48.88 ± 3.68), static (26.40 ± 3.14) and dynamic (22.64 ± 3.68) balance scores improved significantly; the pace (59.22 ± 4.67), stride length (19.04 ± 2.24), feet wide (98.02 ± 7.97) and walking velocity (84.86 ± 9.88) and IP of N200 and P300 shortened obviously and P300 amplitude increased significantly in robot group (P < 0.05). Conclusion: This demonstrated that robot-assisted lower limb rehabilitation training in early stage could improve the limb function among hemiplegic patients caused by ischemic stroke. P300 may be considered as an indicator of neurological function improvement and effective robot-assisted lower limb rehabilitation training.
Keywords:
Lokomat Lower Limb Gait Training Rehabilitation Robot, Cerebral Infarction, Hemiplegic, P300

1. Introduction
Walking ability, though important for quality of life and participation in social and economic life, can be adversely affected by neurological disorders such as spinal cord injury, stroke or traumatic brain injury. It is well documented that individuals with chronic stroke often exhibit considerable gait impairments that significantly impact their quality of life [1] [2] . Previous studies showed that the balance and motor functions could be improved by early rehabilitation. Kelly P. et al., assessing the balance function using Berg balance scale, indicated that the robot hip-knee joint liner driver working as integrated external skeletons, could control the hip-knee joint movement and improve the balance functions by stimulating the coordination between muscle groups to effectively control the body movements and the integration ability [3] [4] . Since asymmetric patterns are often equated to poor stability during gait which increases the risk for falls, restoring gait symmetry is often the goal of rehabilitative gait training [5] [6] . Conventional training methods based on this approach, are proved to be effective, e.g. treadmill training, but they require great physical effort from the physiotherapists to assist the patient.
The robot-driven gait orthosis, Lokomat (Hocoma Medial Engineering Inc., Zurich) is the first driven gait orthosis that assists walking movements of gait-impaired patients on the treadmill. Lokomat rehabilitation system is the first lower limb rehabilitation training robot developed by Switzerland Hocoma company, and the Lokomat is adjustable in force, body weight support, and speed so that even severely handicapped patients can exercise in an environment delivering as much challenge as can be handled [7] [8] . In addition to movement disorders, most patients with cerebral infarction had cognition dysfunction, manifesting as perception, attention, learning and memory and judgment ability disorder, and in turn, cognition dysfunction affected physical disability rehabilitation [9] . Recently, increasing evidences suggest that rehabilitation focusing on motor function could impact the individual’s cognitive function and vice versa [10] . Event related potentials (ERP) P300 was discovered by Sutton in 1965, and it can reflect the changes of brain electrical physiological individual cognitive process. For safety, noninvasive and with good time resolution, ERP P300 has gradually been applied in diagnosing cognitive dysfunction after nerve injury and evaluating the prognosis [11] [12] . The data from Liu Ling-yu showed that if the patients received the early rehabilitation in 2 month, the latency of P300 marked shortened and the amplitude of P300 increased in the robot group was better than that in control group [13] . Given the significance ERP P300 and rehabilitation training characteristics of Lokomat rehabilitation system, we explore therapeutic effect of robot-assisted lower limb rehabilitation training on hemiplegic patients and evaluate P300 changes in this training process, so as to provide cerebral function basis for clinical application of robot-assisted lower limb rehabilitation training.
This study was designed to evaluate the changes and significance of auditory P300 in the training of rehabilitation robot in hemiplegic patients with cerebral infarction.
2. Materials and Methods
2.1. Participants
A total of 60 inpatients with ischemic stroke in the early recovery stage in Neurology Department Affiliated Hospital of Hebei United University during 5.2011-11.2012 were randomly divided into control group (n = 30) and Lokomat group (n = 30) (Table 1). All participants received medical approval before enrolment into the study, and no participant had Lokomat undertaken training, or any other structured exercise training, in the 8weeks prior to the study. Individuals were excluded from the study if they had with nerve, muscle, joint diseases or severe heart diseases and with significant cognitive, hearing and understanding impairment. Participants were not required to discontinue their medications during the testing or training sessions, and no participants made any change in their medications during the course of training.

Table 1. Clinical data of subjects.
DC: disease course.
2.2. Intervention
2.2.1. Method in Control Group
Regular trainings in this group, 30 min per day lasting 8 weeks, including functional electrical stimulation, bobath technology, neuromuscular ontology technology, sports and learning.
2.2.2. Method in Lokomat Training
Subjects were led into the Lokomat and with the help of a physical therapist the device was adjusted so that the Lokomat hip and knee centers lined up with those of the subject. After being correctly aligned, the marker clusters were applied to the subject’s feet, shanks, and thighs. Patients walked on a treadmill under the help of a robotic-driven gait orthosis and measured the leg length and bandage size and adjust the robot before training. The walking sessions in the Lokomat group were kept at: 1) the torque of the knee and hip drives can be adjusted from 100% to 0% for one or both legs; 2) the speed of the treadmill can be adjusted from 0 km/h to approximately 3 km/h and body weight support from 0% to 100%; 3) at the beginning of the treatment period, 30% of the body weight of each subject was supported; 4) guidance force provided by the Lokomat on the hemiparetic leg was gradually reduced from 100% to 15% [14] . The training lasted two treatment periods in total with 30 min every time, 3 times per week, 4 weeks as a treatment period (two sessions).
2.3. Outcome Measures
2.3.1. Berg Balance Scale [15]
The Berg Balance Scale (BBS) is comprised of 6 static and 8 dynamic balance tasks with a maximum score of 56. The 14 task ranges from standing up from a sitting position, including Sitting to standing, Standing unsupported, Sitting unsupported, Standing to sitting, Transfers, Standing with eyes closed, Standing with feet together, Reaching forward with outstretched arm, Retrieving object from floor, Turning to look behind, Placing alternate foot on stool, Turning 360 degrees, Standing with one foot in front and Standing on one foot.
2.3.2. Measurements of Pace, Stride Length, Feet Wide and Stride Turnover
Gait parameters were calculated by K421 GAITRite USB (USA). The pace, stride length, feet wide, stride turnover were measured when the participants walked 3 times continuously at a comfortable speed on a 3.8 m × 0.6 m pressure sensor mat connected with a computer, which could reflect the actual gait function changes in daily life.
2.3.3. ERP Measurement
The ERP measurement is done in the university EMG Laboratory with room temperature of 28˚C - 32˚C. Tell the purpose of the exam and give a pretest first to make sure the participants total understand the requirements. Medtronic Keypoin. Net electrical trigger potentiometer is adopted and, during the test, recording electrodes are placed at C1 and C2 according to 10 - 20 international EEG electrode system, and reference electrode are located at right earlobe (A2) and forehead (FPz) electrode impedance is less than 5 kΩ. Pure tone “auditory non-target stimulation sequence” with sound intensity of 110 dB, frequency of 0.3 - 1 Hz and waviness width of 50 ms, is used to stimulate their ears. Targeted stimulation is high frequency tone with an occurrence probability of 25%, while non-targeted stimulation is low frequency tone with an occurrence probability of 75%, and both of them were calculated for the superposition averaging. Targeted stimulation superposition is 200 times. Participants count the targeted stimulation in silence. Analysis time is 800 ms with a sensitivity of 50 μV/D. Analysis index include the IP of N100, N200, P200 and P300, as well as the amplitude of P300. The researchers used unified instructions and test parameters, and employed fixed operators.
2.4. Statistical Analysis
Statistical analyses were conducted using SPSSv17.0. Measurement data were expressed with  ± S, and comparing the results before and after the intervention using one way ANOVA. P < 0.05 is considered as having statistical significance and comparing the results before and after the intervention using the t-test.
± S, and comparing the results before and after the intervention using one way ANOVA. P < 0.05 is considered as having statistical significance and comparing the results before and after the intervention using the t-test.
3. Results
3.1. Quantitative Analysis of Included Subjects
A total of 60 inpatients with ischemic stroke in the early recovery stage were included in the fine analysis. The case group matched the control group in age, gender, Hemiplegia side, DC, MMSE and NHSS (P > 0.05). There were no significant differences between groups in general information (P > 0.05). See Table 1.
3.2. Results of BBC
There was no significant difference of total, static and dynamic balance scores before treatment between groups (P > 0.05). After 8 weeks treatment, total, static and dynamic balance scores improved significantly in Lokomat group (P < 0.05). See Table 2.
3.3. Results of Gait Analysis
There were no significant differences in scores of pace, stride length, feet wide (P > 0.05). The scores of pace, stride length and stride turnover were markedly higher in Lokomat group than control group (P < 0.05). See Table 3.
Table 2. Comparison of Berg balance score.
BT: before treatment; Comparison within control groups: Comparison before treatment, aP > 0.05; Comparison after 8 w, bP < 0.05.
Table 3. Comparison of gait analysis.
BT: before treatment; Comparison within control groups: Comparison before treatment, aP > 0.05; Comparison after 8 w, bP < 0.05.
3.4. Comparison of N100, N200, P200, P300 Incubation Period (IP) and P300 Amplitude
There was no significant difference of N100, N200, P200, P300 IPs and P300 amplitudes before treatment between groups (P > 0.05). After 8 weeks treatment, N200 and N200 IPs shortened significantly (P < 0.05), and P300 amplitude increased obviously (P < 0.05). See Table 4.
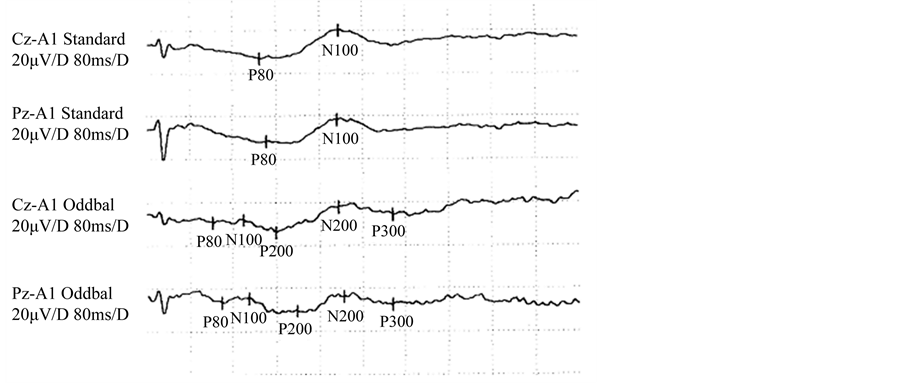
3.5. Comparison of N100, N200, P200, P300 Incubation Period (IP) and P300 Amplitude in the Figure between the Two Groups
From Figure 1, there was no significant difference of N100, N200, P200, P300IPs and P300 amplitudes before treatment between the two group (see Figure 1(a) and Figure 1 (b)); after treatment, there was significant difference between the two groups; compared to the control group, N100, N200 and N200 IPs shortened significantly and P300 amplitude increased obviously after treatment in the Lokomat group (P < 0.05) (see Figure 1(c) and Figure 1(d)).
4. Discussion
Our results indicate that the Lokomat robot has a positive promotion on balance, gait ability. Modern concepts of motor learning favor a task specific training, the patient should ideally train all walking movements, needed in daily life, repetitively in a physically correct manner [16] . Recently developed rehabilitation robots allow delivering continuous support for the legs in a physiological gait pattern, high repetition accuracy, and prolonged training duration compared to manual treadmill training. Lokomat, under the control of an intelligent system, can make sure the hip-knee joint exercise is taken in a normal physical state exercise model, which is helpful in stimulating under limb proprioceptors of the joint, muscle and tendon to facilitate the proprioception recovery [17] . The Lokomat training could maintain stability of knee joint, front and back body, and prevent hip buckling by hip-knee joints stretching and bending repeatedly and separately to make sure that lower limb hip-knee joint extend when pushing forward [18] . However, Results indicated that total, static and dynamic were improved after 8 w and is better than the control group. This illustrated that Lokomat was effective in improving patients’ balance function. The reason for that may be that the poor bearing load ability of the suffered side and limited transfer to the suffered side for scaring of falling.
ERP are brain potentials recorded from skull surface by average superposition when people try to proceed a cognitive processing towards certain objects (such as attention, memory and thinking, and its main ingredients includes exogenous compositions (N100, P200) and endogenous compositions (N200, P300)). P300 represents the classification, coding and discriminating speed of brain responding to external stimuli. Amplitude the resource utilization extent in brain information processing, which means that the higher the amplitude is, the more activated neurons are in the sense information processing [19] . P300 has been widely used in researches about dementia, mental illnesses, cerebral vascular diseases, brain injury and drug dependence [20] [21] . Results of the current study showed that P300 IP shortened and amplitude increased largely indicating that early rehabilitation training could improve P300 potential, in accordance with a previous study [22] . It has been proved that early rehabilitation can promote the activity of conceal passage and dormant synapse, the function recombine of non-injury region and the function rebuilt of injury region. It can also induce the plasticity change of synapse and form new synapse [23] , which could increase the synaptic potential summation and affect P300. In this study, the Lokomat bionic exoskeleton mechanical legs, drive on patients with complete exoskeleton structure in
Table 4. Comparison of N100, N200, P200, P300 IPs and P300 amplitude.
BT: before treatment; Comparison within control groups: Comparison before treatment, aP > 0.05; Comparison after 8 w, bP < 0.05.
 (a)
(a)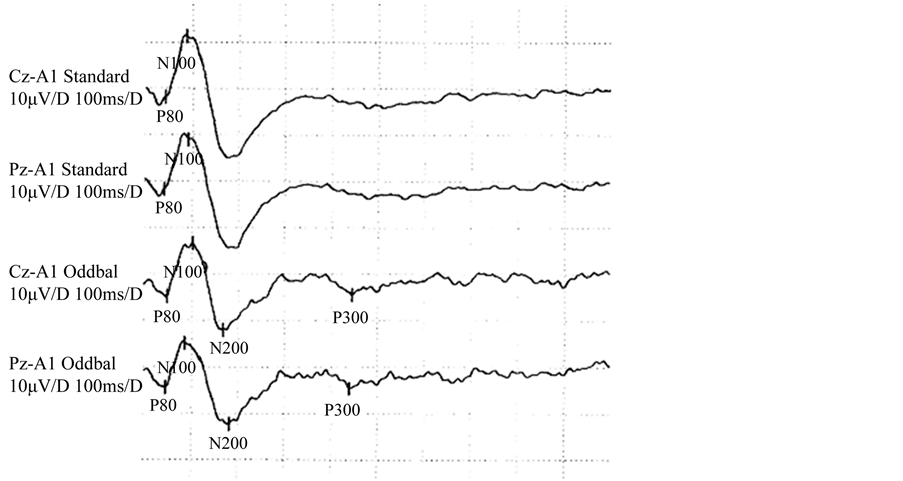 (b)
(b)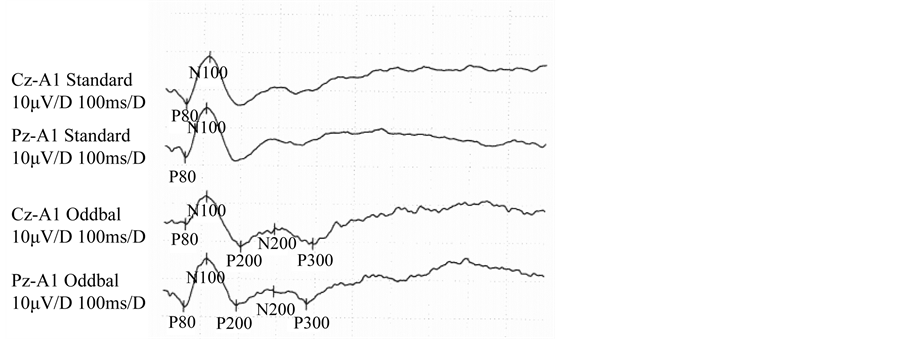 (c)
(c) (d)
(d)
Figure 1. (a), (b) represent before treatment. The P300 potential lengthen between the two groups; (c), (d) represent after 8weeks treatment. There was no significant difference of N100, N200, P200, P300 IPs and P300 amplitudes before treatment between groups (P > 0.05). After 8 weeks treatment, N200 and N200 IPs shortened significantly (P < 0.05), and P300 amplitude increased obviously (P > 0.05). And P300 IP and amplitude changed more obvious in Lokomat group than control group (P < 0.05).
a default movement model for training. The patient’s legs move repeatedly on the treadmill, making cortex signal continuously extend. Studies find that gait training takes part in strengthening the nerve regeneration environment and promoting the expression of BDNF and other nerve growth factors [24] [25] . This could explain why P300 changes in Lokomat group is more obvious than that control group. P300 is the comprehensive result of multiple cortical areas potential, and subject to the regulation of a variety of projection fibers, to a certain extent, reflects the overall level of brain function state [26] . This study found that after a month robot gait training, P300 IP shortened, amplitude increased, indicating the injured brain had rebuilt or recombination, and the brain integrative function and P300 changed. Lower limbs balance function also be found improved, although with no significant difference, which show P300 potential changes in early stage could reveal the effectiveness of the robot gait training. Balance of the human body depends on its normal muscle tone, appropriate sensory input, the integration function of brain and control of mutual nerves or skeletal muscle. After stroke, patients suffered from motor or sensory pathway disorders, abnormal muscle tone and strength, movement control barriers, eventually balance dysfunction [27] . This study applies Lokomat gait rehabilitation training robot, with a weight loss system and intelligent control system, to provide a weight loss condition to make sure the coordinated movements of hip, knee, ankle, and to prompt muscles to produce harmonious muscle contraction phase. Although patients’ motor or sensory conduction recovered quickly, which is helpful for the integration of the brain information, the P300 change was insignificant after a short period of Lokomat training because the poor bear load of affected side in early stage, slow recovery of muscle strength and tone, as well as psychological factors such as being afraid of falling down. The study result also showed that, 8 weeks after training could further shorten P300 IP and increase its amplitude largely than before training in Lokomat group, previous study shows that nerve has plasticity which is characterized by task dependent, relieving on the starting of training mode and maintaining the stimuli. Gregory Barriere, etc. [28] found increased limb coordination, shortened evoked potential latent short, and lower amplitude in incomplete spinal cord injury cats with strict systematic treadmill training than those with ought. Lokomat driven robot gait training could adjust the loss weight according to patients condition, and provide a gait training model in physiological conditions. It introduces the bear load and joint motion information into cortical motor areas, which is stable and more conducive to the remodeling of the nervous system [29] . Besides, gait training can strengthen the release of acetylcholine, 5 serotonin and noradrenaline transmitter, which play an important role in regulation of P300 production, IP and amplitude [30] [31] . This partly explains why P300 changes after 8weeks training were more significant. In addition, this study found that N200 have changed dramatically in Lokomat group, which reflects the identify and processing of brain towards selected events [32] . Systematic technical rehabilitation needs patients’ active cooperation, and the training process itself requires the patient to keep certain attention in order to keep one or more rehabilitation activities. Lokomat training system has an information feedback function, which helps patients understanding their own training effect and shortcomings while training, improving the patients’ interest and motivation. In this process, patients will think and seek improvement measures actively, which is helpful in improving the patients’ thinking ability, and this is one reason P300 and N200 potential further changed in Lokomat group. Robot assisted rehabilitation has been accepted widely.
5. Conclusion
This study provides another evidence for its effectiveness in lower limb gait training. It also finds that P300 could be considered as an objective indicator of a better nerve function by observing the P300 changes in robot-assisted gait training. As with most pilot studies, the small sample size and resultant low statistical power limit interpretation of this study. A modest dose of Lokomat training is effective for improving over-ground walking speed and gait symmetry, and other lower extremity impairments and physical function in persons with chronic hemiparesis post-stroke. Consequently, larger, randomized controlled trials are needed.
Acknowledgements
We wish to thank the patients and their families as well as the involved Rehabilitation Department and Neurology Department.
Funding
This study was support by the Education Key supporting of Hebei province science and technology.
Author Contributions
Yaning ZHAO and Jianmin LI had full access to all data and participated in data collection and analysis. Hao Zheng-wei participated in data analysis, interpretation, designed and supervised this study then wrote the manuscript.
Conflict of Interest
None declared.
Ethical Approval
This study received permission from the Affiliated Hospital of Hebei United University.
References
- Jin, T.-J., Ye, J. and Lin, J. (2009) The Effect of Intensive Weight-Bearing Exercise Especially for Affected Lower Limb on Balance and Walking Function of Stroke Patients. Chinese Journal of Rehabilitation Medicine, 24, 995-998.
- Xu, G.Q., Lan, Y. and Huang, D.F. (2010) The Study on Effect of Motor Imagery on Gait and Walking Ability Rehabilitation in Patients with Stroke Hemiparesis. Chinese Journal of Rehabilitation Medicine, 25, 942-946.
- Westlake, K.P. and Patten, C. (2009) Pilot Study of Lokomat versus Manual-Assisted Treadmill Training for Locomotor Recovery Post-Stroke. Journal of NeuroEngineering and Rehabilitation, 6, 18-20. http://dx.doi.org/10.1186/1743-0003-6-18
- McCain, K.J., Pollo, F.E., Baum, B.S., Coleman, S.C., Baker, S. and Smith, P.S. (2008) Locomotor Treadmill Training with Partial Body-Weight Support before Overground Gait in Adults with Acute Stroke: A Pilot Study. Archives of Physical Medicine and Rehabilitation, 89, 684-691. http://dx.doi.org/10.1016/j.apmr.2007.09.050
- Visintin, M., Barbeau, H., Korner-Bitensky, N. and Mayo, N.E. (1998) A New Approach to Retrain Gait in Stroke Patients through Body Weight Support and Treadmill Stimulation. Stroke, 29, 1122-1128. http://dx.doi.org/10.1161/01.STR.29.6.1122
- Sullivan, K.J., Knowlton, B.J. and Dobkin, B.H. (2002) Step Training with Body Weight Support: Effect of Treadmill Speed and Practice Paradigms on Poststroke Locomotor Recovery. Archives of Physical Medicine and Rehabilitation, 83, 683-691. http://dx.doi.org/10.1053/apmr.2002.32488
- Colombo, G., Matthias, J., Schreier, R. and Dietz, V. (2000) Treadmill Training of Paraplegic Patients Using a Robotic Orthosis. Journal of Rehabilitation Research and Development, 37, 693-700.
- Jezernik, S., Colombo, G., Kelly, T., Frueh, H. and Morari, M. (2003) Robotic Orthosis Lokomat: A Rehabilitation and Research Tool. Neuromodulation, 6, 108 -115. http://dx.doi.org/10.1046/j.1525-1403.2003.03017.x
- Magliaro, F.C.L., de Andrade Matas, S.L. and Matas, C.G. (2009) Cognitive Potential-P300 in Patients with Right Hemisphere Ischemic Lesion. Pró-Fono Revista de Atualização Científica, 21, 285-290.
- Dong, W., Yan, B. and Johnson, B.P. (2013) Ischemic Stroke: The Ocular Motor System as a Sensitive Marker for Motor and Cognitive Recovery. Journal of Neurology, Neurosurgery & Psychiatry, 84, 337-341. http://dx.doi.org/10.1136/jnnp-2012-303926
- Xie, Y. and Li, L.-X. (2006) The Clinical Study of Event Related Potential P300 for Poststroke Depression. Journal of Practical Medical Techniques, 13, 4122-4124.
- Ruchkin, D.S., Munson, R. and Sutton, S. (1982) P300 and Slow Wave in a Message Consisting of Two Events. Psychophysiology, 19, 629-642. http://dx.doi.org/10.1111/j.1469-8986.1982.tb02514.x
- Wu, S.-K., Liu, L.-Y. and Chen, B. (2013) Effects of Manipulation Treatment Cognitive Function and Visual P300 Potential of Patients after Strok. Journal of Rehabilitation Medicine, 28, 238-24l.
- Mayr, A., Kofler, M., Quirbach, E., Matzak, H., Fröhlich, K. and Saltuari, L. (2007) Prospective, Blinded, Randomized Crossover Study of Gait Rehabilitation in Stroke Patients Using the Lokomat Gait Orthosis. Neurorehabilitation and Neural Repair, 21, 307. http://dx.doi.org/10.1177/1545968307300697
- Straube, D., Moore, J., Leech, K. and Hornby, T.G. (2013) Item Analysis of the Berg Balance Scale in Individuals with Subacute and Chronic Stroke. Topics in Stroke Rehabilitation, 20, 241-249. http://dx.doi.org/10.1310/tsr2003-241
- Asanuma, H. and Pavlides, C. (1997) Neurobiological Basis of Motor Learning and Memory. Neuroreport, 3, 1-5.
- Lo, A.C. and Triche, E.W. (2008) Improving Gait in Multiple Sclerosis Using Robot-Assisted, Body Weight Supported Treadmill Training. Neurorehabilitation and Neural Repair, 22, 661-671. http://dx.doi.org/10.1177/1545968308318473
- Morrison, S.A. and Backus, D. (2007) Locomotor Training: Is Translating Evidence into Practice Financially Feasible? Journal of Neurologic Physical Therapy, 31, 50-54. http://dx.doi.org/10.1097/NPT.0b013e3180690679
- Allison, B.Z. and Polieh, J. (2008) Workload Assessment of Computer Gaming Using a Single-Stimulus Event-Related Potential Paradigm. Biological Psychology, 77, 277-283. http://dx.doi.org/10.1016/j.biopsycho.2007.10.014
- Jiang, B., Chen, Y.-M. and Meng, X.-L. (2010) Research on Neuropsychology and Event-Related Potential in the Patients with Vascular Cognitive Impairment. Chinese Journal of Geriatric Heart Brain and Vessel Diseases, 12, 145- 147.
- Li, H.-L., Fang, J.-Y. and Xue, X.-P. (2010) The Application of P300 Potential on the Traumatic Brain Injury. Chinese Journal of Physical Medicine and Rehabilitation, 32, 551-553.
- Medvidovic, S., Titlic, M. and Maras-Simunic, M. (2013) P300 Evoked Potential in Patients with Mild Cognitive Impairment. Acta Informatica Medica, 21, 89-92. http://dx.doi.org/10.5455/aim.2013.21.89-92
- Scholz, J., Klein, M.C., Behrens, T.E. and Johansen-Berg, H. (2009) Training Induces Changes in White-Matter Architecture. Nature Neuroscience, 12, 1370-1371. http://dx.doi.org/10.1038/nn.2412
- Li, H.-L., Liu, L.-Q. and Lu, H.-Y. (2012) Effect of Body Weight Support Treadmill Training or Du Channel Electroacupuncture on Expressions of Nerve Growth Factor and Growth-associated Protein-43 in Rats with Spinal Cord Transection. Chinese Journal of Rehabilitation Theory and Practice, 18, 930-932.
- Van Hedel, H.J. and Dietz, V. (2010) Rehabilitation of Locomotion after Spinal Cord Injury. Restorative Neurology and Neuroscience, 28, 123-134.
- Li, Y., Wang, L.Q. and Hu, Y. (2009) Localizing P300 Generators in High-Density Event-Related Potential with fMRI. Medical Science Monitor, 15, 47-53.
- Ye, H., Yang, Q.-H. and Cai, H. (2012) The Effects of Balance Function Training with Visual Biofeedback on Functional Rehabilitation of Lower Extremity of Stroke Hemiplegic Patients. Chinese Journal of Physical Medicine and Rehabilitation, 34, 45-47.
- Barrière, G., Leblond, H., Provencher, J. and Rossignol, S. (2008) Prominent Role of the Spinal Central Pattern Generator in the Recovery of Locomotion after Partial Cord Injury. Neuronscience, 15, 3976-3987.
- Mayr, A., Kofler, M., Quirbach, E., Matzak, H., Fröhlich, K. and Saltuari, L. (2007) Prospective, Blinded, Randomized Crossover Study of Gait Rehabilitation in Stroke Patients Using the Lokomat Gait Orthosis. Neurorehabilitation and Neural Repair, 21, 307-314. http://dx.doi.org/10.1177/1545968307300697
- Song, J.-G., Zhang, N. and Mu, J.-L. (2009) A Study on Relation with Event-Rated Potential P300 and the Serum Levels of Monoamine Neurotransmitter with Senile Dementia Patients. Journal of Apoplexy and Nervous Diseases, 26, 444-446.
- Mochizuki, Y., Oishi, M. and Takasu, T. (1998) Correlations between P300 Components and Neurotransmitters in the Cerebrospinal Fluid. Electroencephalography and Clinical Neurophysiology, 29, 7-11. http://dx.doi.org/10.1177/155005949802900106
- Gu, L., Lv, Y.-B. and Su, L. (2008) Analysis Oil the Detection of MMSE and P300 in Ischemic Stroke Patients. Journal of Liaoning University of Traditional Chinese Medicine, 10, 63-65.
NOTES

*Corresponding author.