Open Journal of Nursing
Vol.05 No.04(2015), Article ID:55253,11 pages
10.4236/ojn.2015.54034
Effectiveness of ICU Diaries: Improving “Distorted Memories” Encountered during ICU Admission
Tomohide Fukuda1, Tomoko Inoue1, Yoshiko Kinoshita2, Tamiko Yukawa2
1Department of Critical and Invasive Palliative Care Nursing, Tokyo Medical and Dental University, Tokyo, Japan
2Department of Nursing, NTT East Japan Kanto Hospital, Tokyo, Japan
Email: fukuda.cc@tmd.ac.jp
Copyright © 2015 by authors and Scientific Research Publishing Inc.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/



Received 17 March 2015; accepted 28 March 2015; published 31 March 2015
ABSTRACT
Background: It is said that after ICU discharge, 40% of patients suffer from acute stress symptoms, such as anxiety and depression, caused by “distorted memories” (memory loss and delusions) due to various treatments in the ICU. This study focused on the quantitative and qualitative effects of ICU diaries on distorted memories that patients encountered during their time in the ICU. Aim: To assess improving distorted memories by providing information during ICU admission to patients to relieve the acute stress symptoms after ICU discharge. Design and Methods: This nonrandomized controlled trial included patients aged ≥20 years who had received treatment for ≥3 days in the ICU. Using ICU memory tool, the Hospital Anxiety and Depression Scale (HADS) and the Acute Stress Disorder Scale (ASDS) approximately 1 week after ICU discharge, then HADS and ASDS prior to hospital discharge, the change in mean values were compared between two groups (control and intervention) using a Wilcoxon signed-rank test. The intervention group was surveyed prior to hospital discharge using semi-structured interviews, and descriptions were analyzed by the content analysis method of Krippendorff. Results: Twenty-three participants were included in the control group, and 17 in the intervention group. When comparing subjects with distorted memories between the groups, we found reduced values for HADS anxiety (7.1 ± 3.8 to 5.7 ± 2.7, p = 0.011), HADS depression (8.6 ± 5.0 to 7.2 ± 4.3, p = 0.003), and ASDS (46.9 ± 13.8 to 43.8 ± 11.4, p = 0.012) in the intervention group. Based on the narrations, patients wanted to investigate facts in the ICU diary while having someone help them to remember these events. Conclusion: Improving distorted memories during ICU admissions may relieve acute stress symptoms. In addition, these patients needed someone to investigate facts from the ICU admission.
Keywords:
Aftercare, Acute Stress Symptoms, ICU Diary, Distorted Memories

1. Introduction
Receiving invasive treatments for a severe disease involves extreme physical and mental stress for intensive care unit (ICU) patients. Patients admitted to the ICU may suffer from memory loss and delusional memories associated with the events that occur in the ICU due to severe pain, deep sedation, or the acute onset of their condition. In addition, many patients clearly recall events that occurred in state of delirium after ICU discharge [1] . These so-called distorted memories remain intense within the patient and can subsequently lead to Acute Stress Disorder (ASD), i.e., anxiety and depression, and a higher risk of Post-Traumatic Stress Disorder (PTSD). Actually, the possibility that patients discharged from the ICU will suffer from PTSD is 21% - 35%, which is 10 times greater than that for persons who live normal lives [2] . Therefore, to understand the experiences of these patients, care following an ICU visit has become an important topic for ICU nurses.
As a part of the nursing care for patients admitted to the ICU, ICU nurses in Scandinavian medical institutions started using ICU diaries in the 1990s [3] , which has been established as a type of care mainly used in Europe. This can be a tool for patients after discharge from the ICU to provide information during the ICU admission, such as the course of treatment, the state of daily life in the ICU, and persons who came to ICU to meet the patient. ICU diaries were written by ICU nurses, other medical staff, and family members. The patients who read the ICU diary in the ward were often surprised at the facts from the ICU and delighted at the comments from one’s family. In addition, the patients were able to share the information from the ICU with family members and nursing staff in the general ward. These experiences helped to fill in the memory gap of the patients [4] - [6] and provided a sense of coherence to their memories [7] . In this way, ICU diaries are considered a “gift” from the patient’s family and ICU nurses [8] .
As for the psychometric outcomes from a long-term perspective, it has been reported that anxiety and depression following hospital discharge improved in patients who were given an ICU diary [9] . As a secondary effect, the ICU diary helped to ease the psychological stress of the family members of the patients who received the diary [10] . ICU diaries can reduce the chances of the onset of PTSD [11] and improve the patient’s quality of life (QOL) [12] . Therefore, providing patients with factual memories through the use of the ICU diary may improve the patient’s QOL. Previous studies have emphasized the benefits of using ICU diaries, as stated above.
However, the evidence for using ICU diaries has not been clarified. It is not clear why ICU diaries may be effective for patients [13] . In this study, we focused on improving distorted memories using the ICU diaries as soon as possible to relieve the patient’s acute stress symptoms over the short term (while he/she was still admitted to the hospital).
2. Aim
The aim of this study was to assess the extent of overcoming distorted memories by providing information during the ICU admission (using ICU diary) to patients to relieve acute stress symptoms after ICU discharge in the short term.
3. Methods
3.1. Design
A nonrandomized controlled trial was conducted. There had been no reports about the use of the ICU diary in Japan. Therefore, these data were collected during two periods: the first period consisted of a collection of data for the control group and the second was for the data from the intervention group. In this study, the participants in the control group were provided normal care in the ICU, and the intervention group was provided an ICU diary and normal care in the ICU.
3.2. Settings and Participants
This study was conducted from July 2014 to December 2014, with the control group comprising patients admitted from July to September and the intervention group comprising patients admitted from October to December. This study was conducted at a general hospital in Japan with approximately 600 beds and an eight-bed ICU. The subject sample included patients aged ≥20 years who had been treated in ICU for ≥3 days. The patients with mental illness or for whom the recovery of cognitive function was thought to be difficult because of higher brain dysfunction were excluded.
3.3. ICU Diary
To start the ICU diaries, guidelines were created in reference to previously conducted studies [14] and were distributed to the ICU nurses. Because the participating hospital was implementing the ICU diary for the first time, the following points were given particular attention when making diary entries:
(1) Diary entries should be primarily handwritten by the nurse looking after the patient each day.
(2) Diary entries should convey facts that focus on daily activities and the process of recovery for the patient.
(3) The interaction with and care received from health care providers and family members should be mentioned.
(4) The patient’s condition when interacting with health care providers and family members and the response to care should be mentioned.
(5) Any supporting comments should be mentioned, and
(6) In accordance with the policies of the participating facilities, no photos should be attached.
Furthermore, the diary entries were checked by a researcher and two nurse administrators from the ward to verify that the content was not unpleasant to the patient. The handwritten diary was typed by a researcher using Microsoft Word, and then bound into a file for the exclusive use of the patient. The prepared ICU diary was handed to the patient by a researcher during the patient’s visit to the hospital room approximately 1 week after discharge from the ICU. The diary content was read together by the patient and the researcher to reflect on the events that occurred during the ICU admission. Furthermore, as instructed by the institutional review board (IRB) of the participating institution, the researchers explained to the patients and their family members that the ICU diary would be collected for examination prior to the hospital discharge, and it would be sent by post to participants who wanted it after the effectiveness of the evaluation had been confirmed by the present study.
3.4. Data Collection
Researchers visited the hospital rooms to survey the patient approximately 1 week after ICU discharge (post- ICU) using the ICU memory tool (ICUM tool; [15] ), HADS [16] , and ASDS [17] . The researchers also used the HADS and ASDS approximately 10 days after the post-ICU survey and prior to the discharge from the hospital. The flow of this study is shown in Figure 1.
3.4.1. Demographic Data
The basic characteristics regarding ICU patients included age, gender, reason for ICU admission, duration of ICU stay, duration of artificial ventilation, length of sedation, and Simplified Acute Physiology Score 3 (SAPS3; [18] [19] ) to assess severity of patients’ conditions.
3.4.2. Survey of Distorted Memories during ICU Admission
The ICUM tool consisted of a total of 14 items including items that questioned the presence or absence of mem-

Figure 1. Flow of this study.
ories prior to and during ICU admission, items to select the content for experiences during ICU admission, and items to question the patient’s mental state after ICU discharge. The tool enabled a survey of whether patients had memories from their ICU admission and whether they had delusional memories. Responses to the items about the memories prior to and during ICU admission were given in a “yes/no” format, whereas for the responses regarding experiences in the ICU, the patients were asked to select the item or items that they had personally experienced (21 items including nasal tube, being almost injured by someone, darkness, and hallucinations). The items regarding the patient’s mental state, following ICU discharge, were in short answer form; for patients for whom it was difficult to write, a researcher acted as a scribe. The participating patient immediately checked the written content.
3.4.3. HADS and ASDS
HADS was developed to assess depression and anxiety. It consisted of simple questions including the anxiety scale (HADS-anxiety) with seven items and the depression scale (HADS-depression) with seven items. Each response was scored from 0 - 3 points, with an overall score of 0 - 7 points considered “normal,” 8 - 10 points considered “borderline abnormal,” and 11 points or more considered “abnormal.”
ASDS was a tool to screen for acute stress disorder consisting of a 19-item questionnaire that was answered by the individual. The questionnaire items included emotional flatness, sleeplessness, and reduced ability to concentrate, which were scored on a 5-point scale from “1. Not at all” to “5. Very much,” with a cutoff score of 56.
3.4.4. Interviews
The interview guide was created to survey the participants in the intervention group to assess how they used the ICU diary and how they felt about it. The survey was conducted prior to the hospital discharge using semi- structured interviews (Table 1). After the patients consented, the interview was recorded and verbatim reports were created.
3.5. Ethical Approval
Approval was obtained from the ethics committee of the Medical Research Institution of Tokyo Medical and Dental University (No. 1817) and the ethics committees of the participating medical institutions (No.14-128). Participants were provided a written explanation of study objectives and determinations of study participation, and written consent was obtained from the participants. The interviews of the participants in the intervention group were conducted in interview rooms in the wards to avoid any psychological stress to the participants. For the participants who were scheduled for ICU admission, the researchers explained the objectives of the study in writing, and written consent was obtained at the “ICU admission orientation” that was conducted on the day prior to the ICU admission.
For patients who underwent emergency ICU admission, the patient’s family members first received an expla- nation of the study objectives in writing. After the patient was discharged from the ICU in stable condition, a

Table 1. Interview guide.
researcher visited the patient, explained the study objectives, and obtained consent.
3.6. Data Analysis
3.6.1. Characteristic of Participants
The basic patient characteristics (age, gender, hospital department, reason for ICU admission, SAPS3 to assess severity, duration of intubation, and length of sedation) were analyzed by descriptive statistics. The mean values and range for each characteristic were obtained, and the statistical differences between the two groups were found using Fisher’s exact test and Welch’s t-test.
3.6.2. ICUM Tool, HADS and ASDS
The ICUM tool was used to perform a simple tabulation of memory loss and the presence or absence of delusional memories. Patients with memory loss or delusional memories as determined by the ICUM tool were included in our study as patients with distorted memories. Furthermore, changes in HADS-anxiety, HASDS-de- pression, and ASDS scores of patients with distorted memories underwent intergroup and intragroup comparison using the Wilcoxon signed-rank test. Statistical analyses were conducted using PASW Statistics 18, and a p value of <0.05 was considered statistically significant.
3.6.3. Interviews
To clarify how the patients used the ICU diaries, and to determine whether the diary helped to clarify memories and experiences, data obtained from the interviews were analyzed using the content analysis method of Krippendorff [20] . First, the verbatim reports and the content of notes were repeatedly read, and the narrations pertaining to the ICU diary, as well as the clarification of memories and experiences, were selected. The meaning of the selected narration was extracted, and a description of the participant’s narration was used as a label. Similar labels were summarized into codes, and codes with similar meanings were summarized into subcategories. The subcategories were further summarized and integrated into categories. The entire data analysis process was supervised by an expert in nursing research to ensure the reliability and validity of the analyses.
4. Results
During the length of this study, 23 patients were included in the control group and 17 in the intervention group. The control and intervention groups and the levels of attrition during the study are shown in Figure 2. The two groups are summarized in Table 2. Some ICU diary entries written by the ICU nurse required corrections; however, these corrections were only for misspelled or missing words and there was no rephrasing required.

Figure 2. Participants of control and intervention group with levels of attrition.
Table 2. Characteristics of participants.
4.1. Distorted Memories of Patients during ICU Admission
As a result of our survey of patients with distorted memories using the ICUM tool, there were 14 patients in the control group with “distorted memories” including five patients with memory loss, six patients with delusional memories, and three patients who experienced both simultaneously. The intervention group consisted of 13 patients with distorted memories, including six patients with memory loss, five patients with delusional memories, and two patients who experienced both simultaneously (Table 3).
4.2. Change in HADS and ASDS
The changes in HADS and ASDS scores from after ICU discharge to prior to hospital discharge for both groups are shown in Table 4. Patients in the intervention group with distorted memories, the HADS-anxiety score changed from 7.1 ± 3.8 after ICU discharge to 5.7 ± 2.7 (p = 0.011) prior to hospital discharge, while the HADS-depression score changed from 8.6 ± 5.0 after ICU discharge to 7.2 ± 4.3 (p = 0.003) prior to hospital discharge. ASDS changed from 46.9 ± 13.8 after hospital discharge to 43.8 ± 11.4 (p = 0.012). Both HADS and ASDS scores decreased in the intervention group (Figure 3).
4.3. The Experience of Accepting the ICU Diary
Seventeen patients in the intervention group were interviewed, and four patients withdrew their participation for health reasons; therefore, the narrations of 13 patients were analyzed. The mean duration of the interviews was 19 min. From the participant narrations, 36 codes were obtained with the extraction of 11 subcategories and five categories (Table 5). The results of the analysis are explained below using each category and patient quotes.
Reflecting upon the severe phase with the help of the individual’s own memories and the ICU diary
Patients who were admitted to the ICU were given an ICU diary for the first time during this study, which enabled the patient’s subjective reality and the objective reality to be compared. The diary described the conditions in which the patients gradually recovered, and the patients reflected on the recovery process of their illness.
“…I remembered something was put into my mouth and I could not close my mouth. It was so painful and difficult to breathe. I was in a panic. Then, I was told to calm down and many people gathered. After this, I seemed to be unconscious. In the general ward, I have read my diary, and I had received treatment for severe pulmonary failure and medication to remove the pain. That distress, it was so hard for me. But I could know factual things what occurred in the ICU and connect my memories to them.” (Participant D)
Table 3. Participants with distorted memories in the ICU.
P/E: Planned/Emergency.
Table 4. Descriptive statistics for HADS and ASDS scores.
Finding reality through one’s own memories with the help of surrounding information
Some patients said that the provision of information dealing with various topics was very beneficial to them for learning about the events that occurred in the ICU, and that they were able to reflect upon their difficult phase with the help of their own memories and the ICU diary. When the patients read the ICU diary, some found discrepancies between their own memories and the contents of the ICU diary; however, any discrepancies between one’s own memories and the ICU diary were resolved by asking friends and family.
“I have few memories of when I was in the ICU. So the ICU diary was so helpful to know what occurred in the ICU and to create an opportunity to talk with my family and the medical staff. In the ICU diary, they wrote about my situation in the ICU, such as I was sleeping due to sedation and was on ventilation, receiving medication via the IV drip. My family saw that and they were worried. They wrote about that in ICU diary. I was so moved by that! I confirmed what had occurred with my family and the medical staff. The ICU diary connected with me and my family again.” (Participant B)
Perception of experience and nurse care through the ICU diary
Patients admitted to the ICU emergently were unable to recall the circumstances of the ICU through the ICU
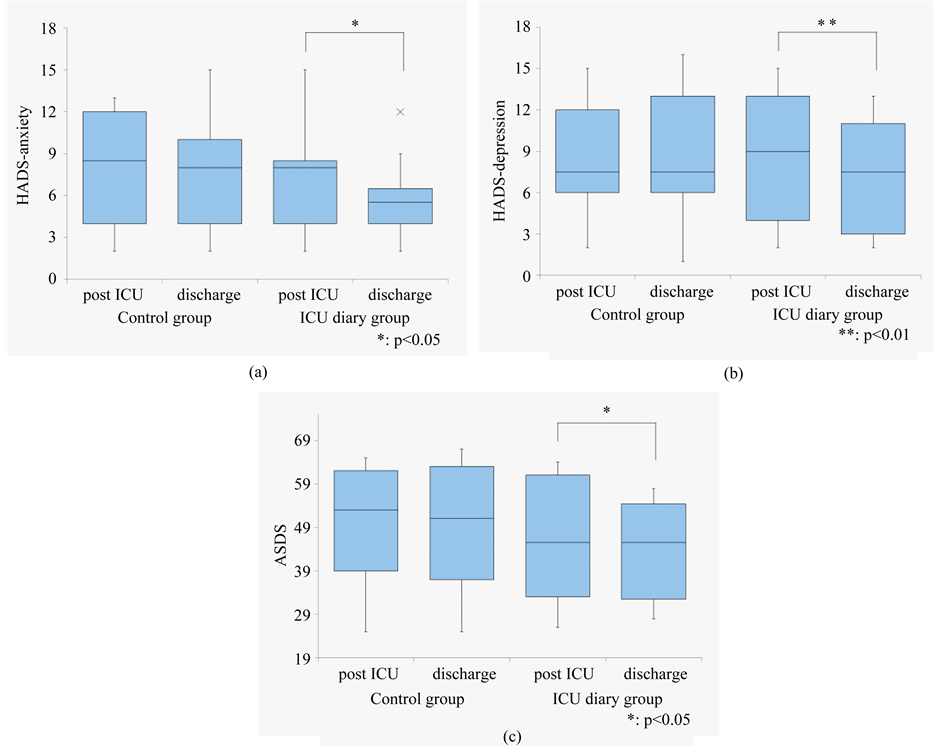
Figure 3. (a) Change in HADS anxiety scores from the participants with distorted memories in ICU; (b) Change in HADS depression scores in the participants with distorted memories in ICU; (c) Change in ASDS scores in the participants with distorted memories in ICU.
Table 5. Subjective effects of ICU diary as perceived by patients.
diary alone; however, the memories began to return with the help of others. The ICU diary also mentioned any accidents and nursing care that occurred in the ICU.
“My diary was written about my delirium time. When I was treated by mechanical ventilation, I seemed to be delusional. I don’t remember that or anything around that time, but that was not a negative thing for me. I understood that nurses cared for me. I think it was so difficult for the nurses to take proper care. However, the nurses wrote that ‘it would be getting better soon; we adjusted the amount of medicine and the environment around the bedside to help you feel comfortable.’ I thanked the ICU nurses so much. Now, I am able to laugh about the episode with my family.” (Participant J)
In addition to the ICU diary, patients required someone to give them courage for reflection
Patients who had strong memories of delusions said that they were burdened by the delusional memories and were unable to open the ICU diary. Patients with a complete loss of memory during their ICU admission were unable to accept their situation despite reading the ICU diary. For them, the ICU diary was simply a tool, in which information was written, and they needed someone to encourage them to reflect upon and assist them in interpreting the information given in the ICU diary.
“I have no memory about the time I was in the ICU. So I could not understand what occurred in the ICU despite reading the ICU diary. I could not imagine the environment of the ICU. To understand the comments from the ICU diary, I needed to greatly interact with someone who knew about the story of my ICU admission.” (Participant F)
Wanting to reconfirm the place where one received treatment
On reading through the ICU diary, the entries described the repeated improvement and deterioration of the patient’s condition. The patients became aware that the nurses provided intensive care when the patient was experiencing difficulties, and the patients said that the nurses’ comments not only informed them about their reality but provided encouragement. Therefore, the patients became aware of the nursing care through the ICU diary and looked forward to visiting the ICU to reconfirm the course of one’s medical treatment and care.
“I was treated with mechanical ventilation and sedation. I remember what occurred in the ICU, such as speaking with the ICU nurses and doctors. But I have read the ICU diary, and my memory is different from the comments from the ICU diary. I was so interested in this difference the treatment that was provided to me. I want an explanation about the treatment I received.” (Participant K)
5. Discussion
The purposes of this study were to examine the effect of an ICU diary as a tool to provide information about patients admitted to the ICU, to observe whether the diary helped to improve the distorted memories of the patients, and to relieve acute stress symptoms. In the early stages following ICU discharge, the patients who receive intensive care can have memories of their reality in the ICU with some loss of memory; they require a lot of effort to clarify their delusional memories [21] . If their efforts go well, the patient’s QOL will be improved; however, patients in which these efforts fail are at a high risk of developing Post Intensive Care Syndrome (PICS; [22] [23] ), which is a cognitive mental health disorder that follows ICU discharge. A previous study stated that the ICU diary improved the long-term QOL [12] . In this study, the patients in the intervention group had a decrease in HADS and ASDS scores prior to hospital discharge, and we found that giving patients an ICU diary soon after ICU discharge helped improve distorted memories. It has been indicated that receiving medical care while experiencing psychological stress during hospitalization can lead to the onset of PTSD following ICU discharge [24] . Starting early interventions for distorted memories can be very helpful for patients to understand their ICU care and encouragement, and it can smoothly and rapidly reduce mental distress. This means that early interventions for distorted memories will facilitate patients to return to society.
In terms of qualitative data, the ICU diary also served as a tool for the patients to check the entries and trace the progress of their recovery. We also found that the ICU diary served as a communication tool for patients to talk with their family and friends. Reading the ICU diary alone and reflecting on the events that occurred in the ICU with family and friends allowed the information from one’s own memories and from others’ memories to be consolidated, which could help to clarify memories and reduce the distorted memories.
Some patients felt lost when recalling about the events from the severe stage of their illness, including their condition and delusions during their treatment in the ICU. However, reading through not only the progress of inorganic conditions but also the encouraging comments and descriptions of daily care from the ICU nurses led patients to continue to read the ICU diary, which may have served as a tool to facilitate the uneventful recognition of the patient’s current situation. In addition to the original purpose of the ICU diary i.e., to “convey the facts,” knowing how the nurse-in-charge and other people felt about the patient provided encouragement for the patient [25] and may have led to an improvement in distorted memories, encouraged the patients to have a positive outlook regarding their medical treatments, and helped relieve their anxiety and depression.
Although there was no statistically significant difference observed between the groups in this study, there were more patients in the intervention group who were emergency ICU admissions. This may have attributed to a greater percentage of patients with distorted memories who said that they did not understand the situation very well despite reading the ICU diary. In emergency ICU admissions, unlike in scheduled admissions, the patients received invasive treatments without any psychological preparation. Thus, the patients who consequently underwent this great stress had memory loss, and despite reading the ICU diary, were unable to recall the events that had occurred in the ICU. In such instances, the patients attempted to construct the events in the ICU by talking with their family members; however, family members were not always in the ICU with the patient and lacked the information to help clarify the patient’s experience. Thus, the patient requested the assistance of someone who knew their situation well. A previous study stated that the diary alone provided incomplete information [26] . In this study, it was suggested that the patients with memory loss experienced difficulty completing the details of their memories during ICU admission. ICU nurses are typically focused on providing care for patients in the ICU and the patients that are scheduled to be admitted. In this study, we found that after ICU discharge, some patients sought contact with the ICU nurses. As a part of the care for post-ICU patients, the recording of an ICU diary together with post-ICU visits and increased contact with post-ICU patients may help patients to clarify information, and the patients would be able to reflect on the progress of the illness with the patient, and addressing the care needs of the patient may facilitate the smooth social rehabilitation of the patient following hospital discharge.
6. Limitations
In this study, we adapted the nonrandomized controlled trial, which is a limitation because we studied a small sample size to start ICU diaries. In Japan, no system has been established for the long-term, continuous care of patients after being admitted to the ICU. The development of a system to provide long-term support will enable the long-term follow-up of patients with an ICU diary and will help to clarify the areas where patients experienced difficulty during treatment.
7. Conclusion and Implication for Clinical Practice
We found that using ICU diaries to improving distorted memories rapidly helped relieve acute stress symptoms. However, patients admitted to the ICU in an emergency were unable to picture the conditions in the ICU despite reading the ICU diary and sought the information directly from the ICU nurses. In contrast, patients with vivid delusional memories took some time until they were able to read the ICU diary. To further increase effects, ICU nurses should visit patients to investigate facts in the ICU together.
Acknowledgements
We would like to express our deepest gratitude to all of the patients who participated, the physicians, nursing department and ward nurses of the participating medical institution, and to all the ICU nurses who recorded entries in the ICU diaries.
References
- Kinoshita, Y. and Inoue, T. (2006) Impact of ICU Experience on Patients Discharged from the ICU and Their Nursing Care―The ICU Survivor Experience and Its Impact. Japanese Journal of Intensive Care Society, 2, 35-44. (In Japanese)
- Nunomiya, S. (2012) The Influence of Sedation and Analgesia on Long-Term Psychological Outcomes in Survivors of Intensive Care Treatment. Japanese Journal of Intensive Care Medicine, 36, 189-196. (In Japanese)
- Hale, M., Parfitt, L. and Rich, T. (2010) How Diaries Can Improve the Experience of Intensive Care Patients. Nursing Management, 17, 14-18. http://dx.doi.org/10.7748/nm2010.12.17.8.14.c8142
- Bergbom, I., Svensson, C., Berggren, E. and Kamsula, M. (1999) Patients’ and Relatives’ Opinions and Feelings about Diaries Kept by Nurses in an Intensive Care Unit: Pilot Study. Intensive & Critical Care Nursing, 15, 185-191. http://dx.doi.org/10.1016/S0964-3397(99)80069-X
- Bäckman, C.G. and Walther, S.M. (2001) Use of a Personal Diary Written on the ICU during Critical Illness. Intensive Care Medicine, 27, 426-429. http://dx.doi.org/10.1007/s001340000692
- Combe, D. (2005) The Use of Patient Diaries in an Intensive Care Unit. Nursing in Critical Care, 10, 31-34. http://dx.doi.org/10.1111/j.1362-1017.2005.00093.x
- Åkerman, E., Ersson, A., Fridlund, B. and Samuelson, K. (2012) Preferred Content and Usefulness of a Photodiary as Described by ICU-Patients―A Mixed Method Analysis. Australian Critical Care, 26, 29-35. http://dx.doi.org/10.1016/j.aucc.2012.04.002
- Egerod, I. and Christensen, D. (2009) Analysis of Patient Diaries in Danish ICUs: A Narrative Approach. Intensive & Critical Care Nursing, 25, 268-277. http://dx.doi.org/10.1016/j.iccn.2009.06.005
- Knowles, R.E. and Tarrier, N. (2009) Evaluation of the Effect of Prospective Patient Diaries on Emotional Well-Being in Intensive Care Unit Survivors: A Randomized Controlled Trial. Critical Care Medicine, 37, 184-191. http://dx.doi.org/10.1097/CCM.0b013e31819287f7
- Jones, C., Bäckman, C., Capuzzo, M., Egerod, I., Flaatten, H., Granja, C., Rylander, C. and Griffiths, R.D., The RACHEL Group (2010) Intensive Care Diaries Reduce New Onset Post Traumatic Stress Disorder Following Critical Illness: A Randomised, Controlled Trial. Critical Care, 14, R168. http://dx.doi.org/10.1186/cc9260
- Garrouste-Orgeas, M., Périer, A., Mouricou, P., Grégoire, C., Bruel, C., Brochon, S., Philippart, F., Max, A. and Misset, B. (2014) Writing in and Reading ICU Diaries: Qualitative Study of Families’ Experience in the ICU. PLoS ONE, 9, e110146. http://dx.doi.org/10.1371/journal.pone.0110146
- Bäckman, C.G., Orwelius, L., Sjöberg, F., Fredrikson, M. and Walther, S.M. (2010) Long-Term Effect of the ICU- Diary Concept on Quality of Life after Critical Illness. Acta Anaesthesiologica Scandinavica, 54, 736-743. http://dx.doi.org/10.1111/j.1399-6576.2010.02230.x
- Ullman, A.J., Aitken, L.M., Rattray, J., Kenardy, J., Le Brocque, R., MacGillivray, S. and Hull, A.M. (2014) Diaries for Recovery from Critical Illness. Cochrane Database System Reviews. http://dx.doi.org/10.1002/14651858
- Jones, C. (2009) Introducing Photo Diaries for ICU Patients. Journal of the Intensive Care Society, 10, 183-185. http://dx.doi.org/10.1177/175114370901000306
- Jones, C., Humphris, G. and Griffith, R.D. (2000) Preliminary Validation of the ICUM Tool for Assessing Memory of the Intensive Care Experience. Clinical Intensive Care, 11, 251-253. http://dx.doi.org/10.3109/tcic.11.5.251.255
- Zigmond, A.S. and Snaith, R.P. (1983) The Hospital Anxiety and Depression Scale. Acta Psychiatrica Scandinavica, 67, 361-370. http://dx.doi.org/10.1111/j.1600-0447.1983.tb09716.x
- Bryant, R.A., Moulds, M.L. and Guthrie, R.M. (2000) Acute Stress Disorder Scale: A Self-Report Measure of Acute Stress Disorder. Psychological Assessment, 12, 61-68. http://dx.doi.org/10.1037/1040-3590.12.1.61
- Metnitz, P.G., Moreno, R.P., Almeida, E., Jordan, B., Bauer, P., Campos, R.A., Iapichino, G., Edbrooke, D., Capuzzo, M. and Le Gall, J.R., SAPS 3 Investigators (2005) SAPS 3―From Evaluation of the Patient to Evaluation of the Intensive Care Unit. Part 1: Objectives, Methods and Cohort Description. Intensive Care Medicine, 31, 1336-1344. http://dx.doi.org/10.1007/s00134-005-2762-6
- Moreno, R.P., Metnitz, P.G., Almeida, E., Jordan, B., Bauer, P., Campos, R.A., Iapichino, G., Edbrooke, D., Capuzzo, M. and Le Gall, J.R., SAPS 3 Investigators (2005) SAPS 3―From Evaluation of the Patient to Evaluation of the Intensive Care Unit. Part 2: Development of a Prognostic Model for Hospital Mortality at ICU Admission. Intensive Care Medicine, 31, 1345-1355. http://dx.doi.org/10.1007/s00134-005-2763-5
- Krippendorff, K. (1980) Content Analysis: An Introduction to its Methodology. Sage, Beverly Hills, CA. (Translated in Japanese, 1989)
- Fukuda, T., Inoue, T., Sasaki, Y. and Moro, E. (2013) Research on the Actual Condition of the Memories and Experiences of Patients Who Have Been in an Intensive Care Unit. Journal of Japan Academy of Critical Care Nursing, 9, 29-38. (In Japanese) http://dx.doi.org/10.11153/jaccn.9.29
- Davydow, D.S., Gifford, J.M., Desai, S.V., Needham, D.M. and Bienvenu, O.J. (2008) Posttraumatic Stress Disorder in General Intensive Care Unit Survivors: A Systematic Review. General Hospital Psychiatry, 30, 421-434. http://dx.doi.org/10.1016/j.genhosppsych.2008.05.006
- Davidson, J.E., Harvey, M.A., Schuller, J. and Black, G. (2013) Post-Intensive Care Syndrome: What It Is and How to Help Prevent It. American Nurse Today, 8, 32-38.
- Davydow, D.S., Zatzick, D., Hough, M.I. and Katon, W.J. (2013) A Longitudinal Investigation of Posttraumatic Stress and Depressive Symptoms over the Course of the Year Following Medical-Surgical Intensive Care Unit Admission. General Hospital Psychiatry, 35, 226-232. http://dx.doi.org/10.1016/j.genhosppsych.2012.12.005
- healthtalk. org. (2012) Intensive Care: Patient’s Experiences. healthtalk org. http://www.healthtalk.org/peoples-experiences/intensive-care/intensive-care-patients-experiences/impact-family
- Egerod, I. and Bagger, C. (2010) Patients’ Experience of Intensive Care Diaries―A Focus Group Study. Intensive & Critical Care Nursing, 26, 278-287. http://dx.doi.org/10.1016/j.iccn.2010.07.002