Open Journal of Animal Sciences
Vol.3 No.3A(2013), Article ID:34750,5 pages DOI:10.4236/ojas.2013.33A003
In vivo evaluation of an experimental root-end filling material versus MTA
![]()
1Department of Endodontics, University of Alabama School of Dentistry, Birmingham, USA; *Corresponding Author: eleazer@uab.edu
2Department of Endodontics, Texas A&M, Baylor College of Dentistry, Dallas, USA
3Veterans Administration, Atlanta, USA
4Private Practice, Birmingham, USA
5Department of Anatomic Pathology, University of Alabama School of Medicine, Birmingham, USA
6Animal Resource Program, University of Alabama, Birmingham, USA
7Department of General Dentistry, University of Alabama School of Dentistry, Birmingham, USA
8Department of Behavioral and Population Sciences, University of Alabama School of Dentistry, Birmingham, USA
Copyright © 2013 Paul D. Eleazer et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received 15 May 2013; revised 16 June 2013; accepted 27 June 2013
Keywords: MTA; dog; Pulp; root
ABSTRACT
Mineral trioxide aggregate (MTA) has been found to be very biocompatible in a large number of studies. However, the handling properties can be challenging and research on modified materials to enhance placement are few. The purpose of this study is to compare a new faster setting, and more easily placed preparation with classic MTA in an animal model. Canine premolar teeth from two dogs were randomized and received quadrant surgery timed to allow 50 day and 98 day comparisons. Histologic and radiographic comparisons were made. Results were essentially equal in healing, even close to the materials.
1. INTRODUCTION
Torabinejad introduced mineral trioxide aggregate (MTA) as a highly biocompatible agent for pulp wounds and apical retrofills [1]. In a recent trio of review articles, he and Parirokh presented an excellent review of the literature on MTA [2-4]. They noted the lack of research regarding new forms of MTA [4].
MTA was originally described as a mixture of tricalcium silicate, tricalcium aluminate, tricalcium oxide, and silicate oxide. After hydration it becomes a colloidal gel that sets hard within 4 hours [1]. A recent prospective study of 339 retro filling surgeries by von Arx found MTA superior to a bonded composite by an 11% margin [5]. They used clinical outcomes in a case series as the outcome measure. They also cite three retrospective studies with a collective population size of nearly 400 in which MTA was superior, with 1 or 2 year success rates favoring MTA by 0% to 6%.
In spite of fulfilling almost all of the desired properties of a material for wound healing of pulps and periodontal tissues adjacent to teeth, handling properties of this material have been less than ideal. Dentsply Tulsa has developed a new form they describe as more finely powdered with a small amount of polymer that makes handling easier. The new material comes with a specific liquid that facilitates mixing and placement.
The purpose of this study is to compare in vivo healing of an experimental material versus conventional gray MTA.
2. MATERIALS AND METHODS
2.1. Preliminary actions Approval of the university animal care and use committee was obtained before the study was undertaken. All activities took place in the university animal care facility under direct supervision of their staff and veterinarians.
2.2. Preoperative Day
Two mongrel littermate male dogs were anesthetized and radiographed to confirm root end maturation. Their weights were 61 pounds and 61.5 pounds. The general anesthesia regimen used throughout the experiment was induction with ketamine and valium, followed by maintenance of anesthesia with isofluorane. In anticipation of post-surgical pain, premedication included the non-steroidal anti-inflammatory Carprofen and the narcotic buprenorphine. After each surgical procedure they received a bolus of penicillin G by IM injection.
2.3. Non-Surgical Root Canal Treatment Day
Endodontic procedures were performed on all mandibular premolar teeth. After the routine general anesthesia, each dog received an inferior alveolar nerve block with 1.8 mL of 2% lidocaine containing 1:100,000 epinephrine. With isolation using sterile gauze packs, access was achieved using #2 or #1157 high-speed carbide burs with saline irrigation. Canal contents were removed with stainless steel hand files and slow speed Gates-Glidden drills. Canals were irrigated during canal debridement with 5.25% sodium hypochlorite (Sno-White Bleach, Plover, WI). All canals were enlarged to size 40 and intentionally flared to allow access of a D-11T spreader to within 1 mm of working length. Canals were dried with paper cones and obturated with gutta percha and Roth’s zinc oxide root canal sealer. Access openings were closed with IRM, Intermediate Restorative Material (DentsplyCaulk, Milford, DE) The dogs recovered without signs of distress and received a soft diet.
2.4. First Surgery, Day 0
One week later, designated as day 0, the pre-operative medications and general anesthesia were repeated. 3.6 mL of the same local anesthetic was used for each dog, for inferior alveolar nerve block and for buccal infiltration. The left buccal soft tissues were elevated using a sulcular incision and sharp and blunt dissection. The mental foramina were identified and avoided during the procedure. A 4 mm cut was made in the bone with high speed carbide 1157 bur so as to create a long bony crypt exposing all seven premolar root ends (Figure 1). About two mm of the root end was resected, exposing the gutta percha root canal filling. A straight ultrasonic tip was used to create a retropreparation in each root canal. Removal of gutta percha was confirmed with a micro-mirror. Retrofilling materials were placed according to a randomization schedule. ProRoot MTA (Dentsply-Tulsa, Tulsa, OK) was thoroughly hydrated with fluid provided by the manufacturer. Then the fluid mix was dried by absorbing excess liquid with a gauze sponge, to a rather dry consistency to aid in packing the material. The experimental material was mixed according to the manufacturer’s instructions and placed in the assigned sites. The slightly sticky nature of this material called for pressure from a saline-moistened cotton pellet over the apex
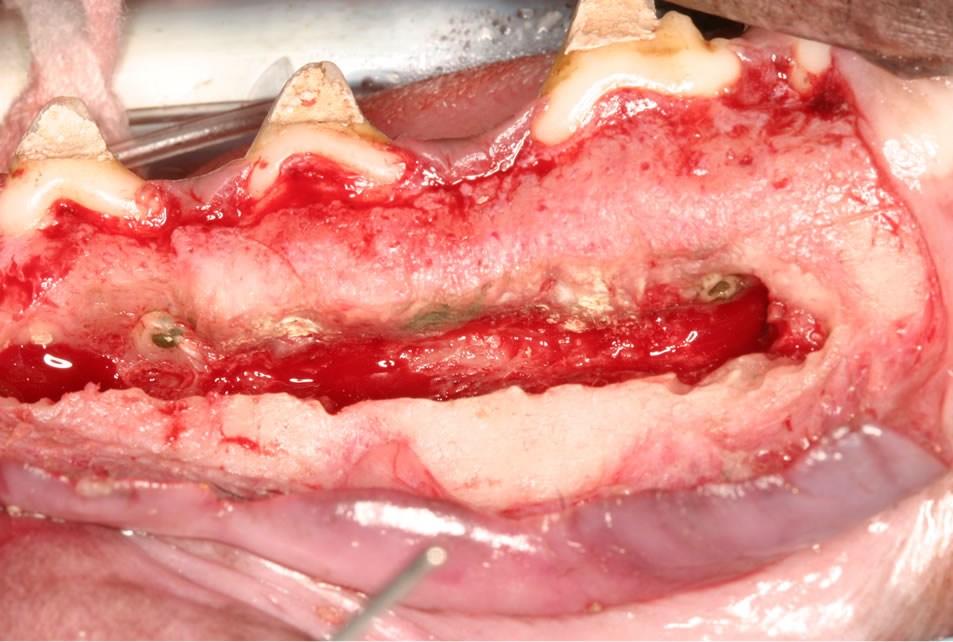
Figure 1. Photograph taken during surgery. Note uniform dimensions of bone trough created.
to ensure good marginal adaptation during setting.
Total irrigant used for the mandibular procedure was estimated at 300 mL. Total blood loss was estimated at 10 mL. The mandibular incisions were closed with 7 to 11 5 - 0 chromic gut interrupted sutures. The dogs recovered without apparent difficulty. They were monitored daily.
2.5. Second Surgery, Day 42
Forty-eight days later (50 days before sacrifice) the procedure was repeated on the opposite side. On the day following the surgery, one dog developed a respiratory infection and was treated with a cephalosporin by deep intramuscular injection daily for four days.
2.6. Final Surgery, Day 98
On day 98 the dogs were deeply sedated, heparinized and perfused with saline, then formo-saline for tissue fixation. Plain and cone beam radiographs were made of the grossly dissected jaws.
2.7. Histologic Preparation
Then small blocks containing one or two roots were cut with a band saw. The blocks were imaged from a proximal view by digital radiography (Kodak RVG 5100, PracticeWorks Systems, Atlanta, GA) and then densitometry measurements were taken of the new bone density in the surgical access cavity. The surgical access was essentially equal for all specimens.
These small blocks were then decalcified in DECAL (Decal Chemical, Tallman NY). This method uses hydrochloric acid with an ion exchange resin to more rapidly remove minerals. The root end filling materials were softened by this process. Sufficient decalcification was determined by cutting into a specimen with a scalpel blade. Transsection of the canal along the long axis was desired however orientation was difficult and some samples were inadequate for microscopic examination. Blocks were dehydrated in graded alcohols and xylenes and embedded in paraffin and cut into 5 micron sections with a diamond blade microtome. Slides were stained with hematoxylin and eosin (H&E), as well as examined in polarized light. In one root, an iatrogenic perforation was found and that specimen was not processed.
2.8. Grading of Histologic Slides
Two blinded investigators (PDE and PDeV) reviewed sections to find the section closest to the retrofilling. Recutting of the blocks was ordered when needed. Optimal sections were graded independently by a panel of three pathologists, including one who had helped select the specimens for final review (PDeV, SW, and LN). H&E sections were graded as follows: 1) distance (in mm) from root apical potion of canal to nearest new bone formation; 2) presence of new cement formation on the root apical portion (yes/no); presence of new cement over the opening of the root canal at the apical portion (yes/no); presence of inflammatory and fibrous infiltrate (yes/no); degree of inflammatory infiltrate (1 = mild, 2 = moderate and 3 = severe).
The shortest distance from the root apex adjacent to the retrofilling material to the bone was measured by a calibrated eyepiece micrometer graticule. Inasmuch as bone had been resected during the surgical procedure, this bone was obviously newly formed.
2.9. Statistical Analyses
Agreement among the three raters was evaluated by calculating differences in measurements of continuous variables for each pair of raters. One-sample t tests were used to test the hypothesis that the mean differences equal zero. For categorical ratings, percent agreement and Cohen’s kappa were calculated for each pair of raters. Statistical significance of disagreement was tested using McNemar’s test. For primary analysis, the mean of the three measurements was used for continuous variables, and consensus of at least two of the three raters was used for categorical measures. P < 0.05 was used to interpret statistically significant differences.
Means of nearest distance between retrofilling material and bone and radiodensity means were compared between the treatment groups using Mixed-model Analysis of Variance (ANOVA) in order to account for multiple observations made on the same dogs. Treatment group, time and their interaction were included as fixed effects in the model. Descriptive statistics are presented as leastsquares means and standard errors.
Presence of cementum over the resected dentin and over the retrofilling material was observed. These categories were graded as present or absent.
Categorical response variables were analyzed using Generalized Estimating Equations (GEE) to implement logistic regression analysis while accounting for multiple observations made on the same dogs.
3. RESULTS
3.1. Radiographic Analysis
Mean density of radiographs did not differ between the materials or the times groups. P was 0.5508 for differences between the experimental material versus classic MTA. P was 0.7865 for the 50 and 98 day data. Cone beam and plain film images confirmed the bone fill (Figure 2). Light microscope images demonstrated the exuberant bone regeneration, even directly adjacent to the root fillings (Figure 3). Raw data is shown in Table 1. Days are noted at time from procedure.
3.2. Histologic Analysis
Inflammatory cells were judged to be present in 83.3% of specimens but the differences between materials was P
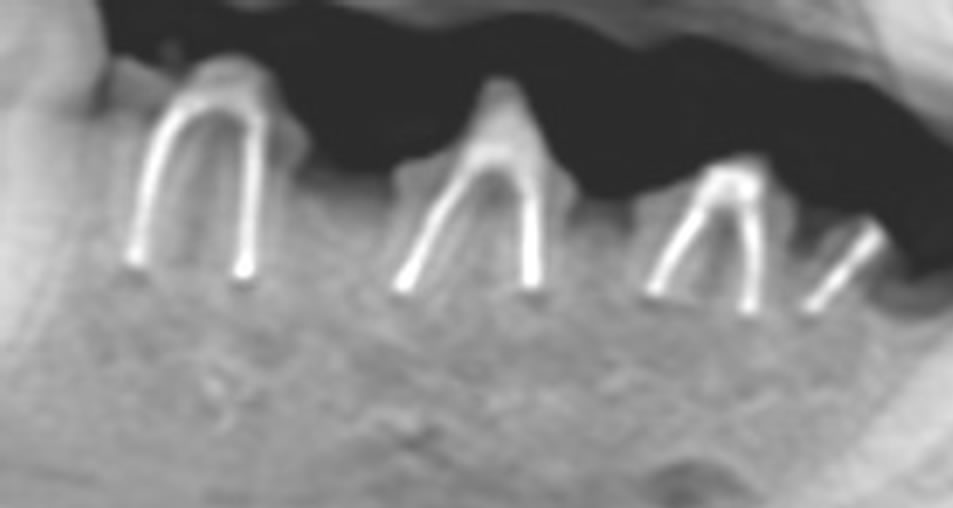
Figure 2. Plain film radiograph of 7 week result. Note excellent bone fill.
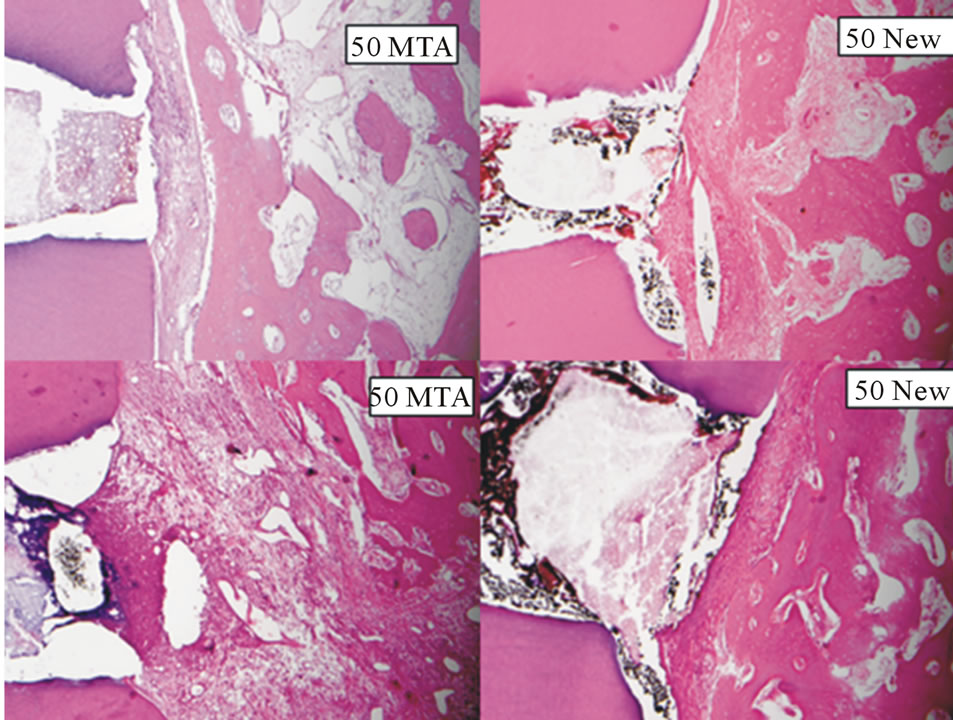
Figure 3. 50 day light microscope images (10× objective lens). Best and worst results for MTA shown in left panels. Best and worst results for new material shown in right panels. Retro preparations range from 1 to 2 mm.
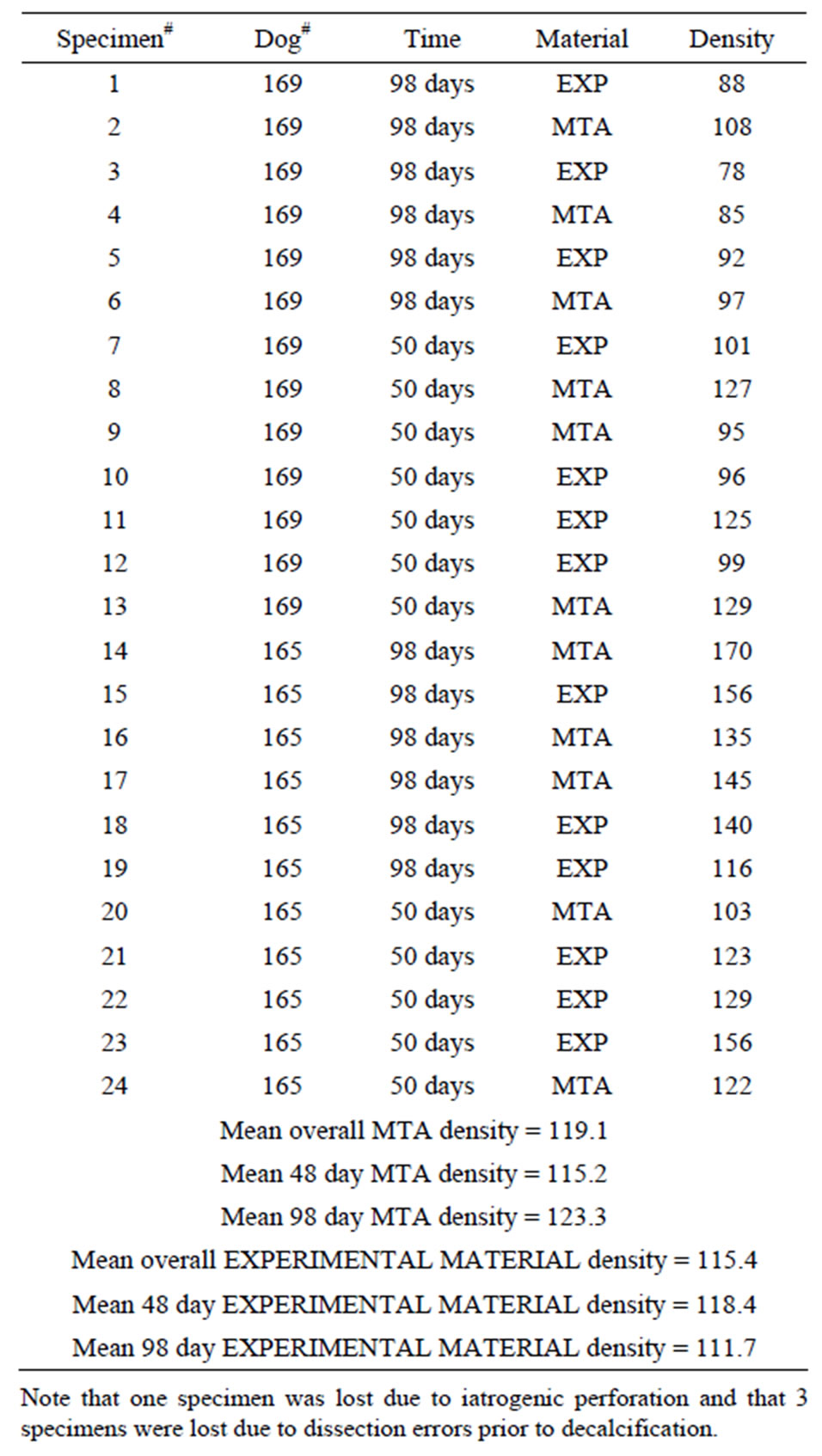
Table 1. Radiodensity data—post mortem data derived from digital radiographs from jaw halves before processing for histology.
= 0.1900. Similarly the grading of the inflammation was not significantly different between groups. One rating was 0, two ratings were 1 and three were given a grade of 2. Adjusting for individual animal and for time effects resulted in a P value of 0.7254. Raw data are shown in Table 2. Days are noted at time from procedure.
3.3. Statistical Analysis
Mean pairwise differences in measurement of nearest bone ranged from 0.0083 to 0.0233 mm, with standard deviations of 0.024 to 0.056 mm. None of the pairwise differences were significant as can be noted by the p values all being 0.15 or greater. Agreement between at least two raters was 100% for all categorical variables. Bone regeneration was exuberant in every case. No root
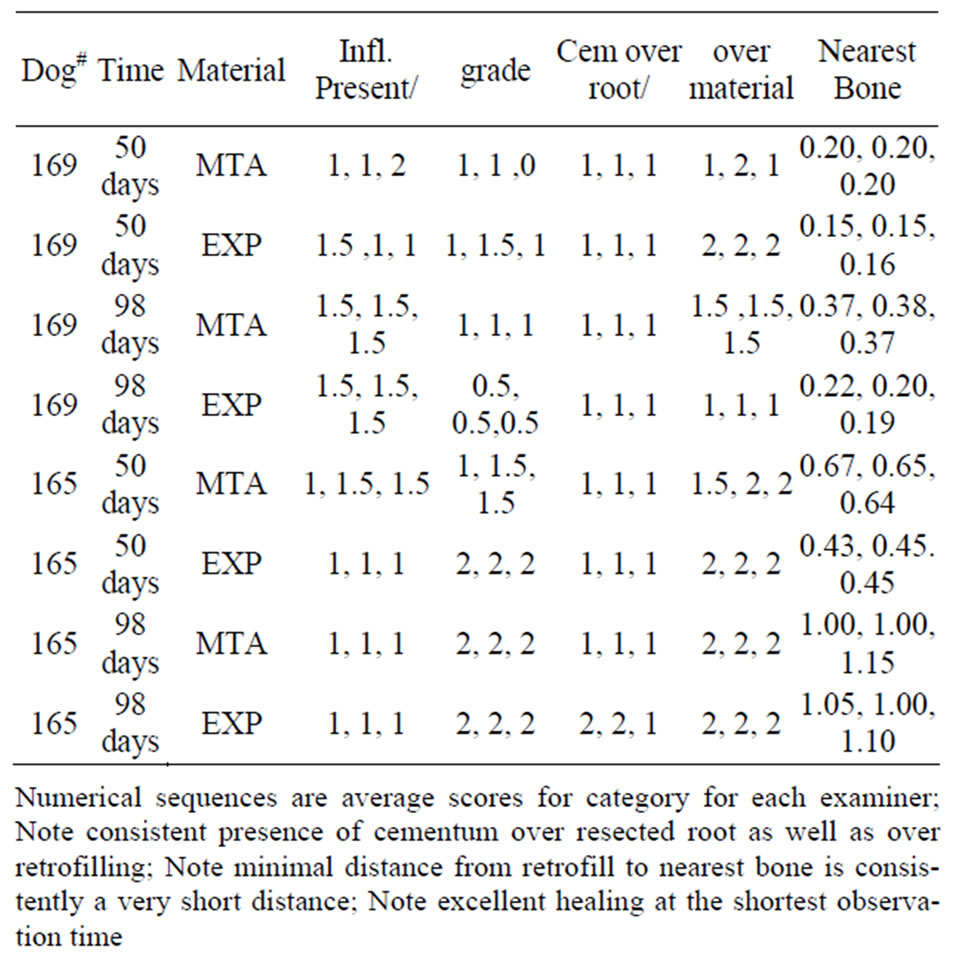
Table 2. Histology results.
resorption was seen. Raw data is shown in Table 3. Days are noted at time from procedure.
Furthermore, there was not a significant difference in mean distance to nearest bone between the experimental material and the classic MTA. P was 0.4143 for this analysis. Measurements made for the 98 day post-op period versus the shorter period were actually statistically significantly at P = 0.0428, yet this is obviously insignificant clinically. The mean difference between groups was not significantly different by post-op time when analyzed by group-time interaction.
The analysis of cementum also revealed no statistically significant differences. Cementum was present on the resected root surfaces in 100% of specimens. Adjusting for dog and time effects, P was 0.3149 for MTA versus the experimental material. Cementum deposition directly on the retrofilling material was positive in one third of the specimens, but there was no statistically significant difference between materials (P = 0.3256).
4. DISCUSSION
These dogs were young and healthy and the teeth were uninfected, so rapid healing was expected. This rapid alveolar bone healing in healthy dogs was confirmed recently by Wang and co-workers who found essentially complete healing of the tooth-ligament-bone relationship 60 days after tooth transplantation [6]. Brasil et al. also noted very good 60 day healing in their study of orthograde overfillings in premolars of healthy young canines [7].
MTA has been shown to enhance bone morphogenic protein in vitro by Yasuda et al., as well as by Maeda et
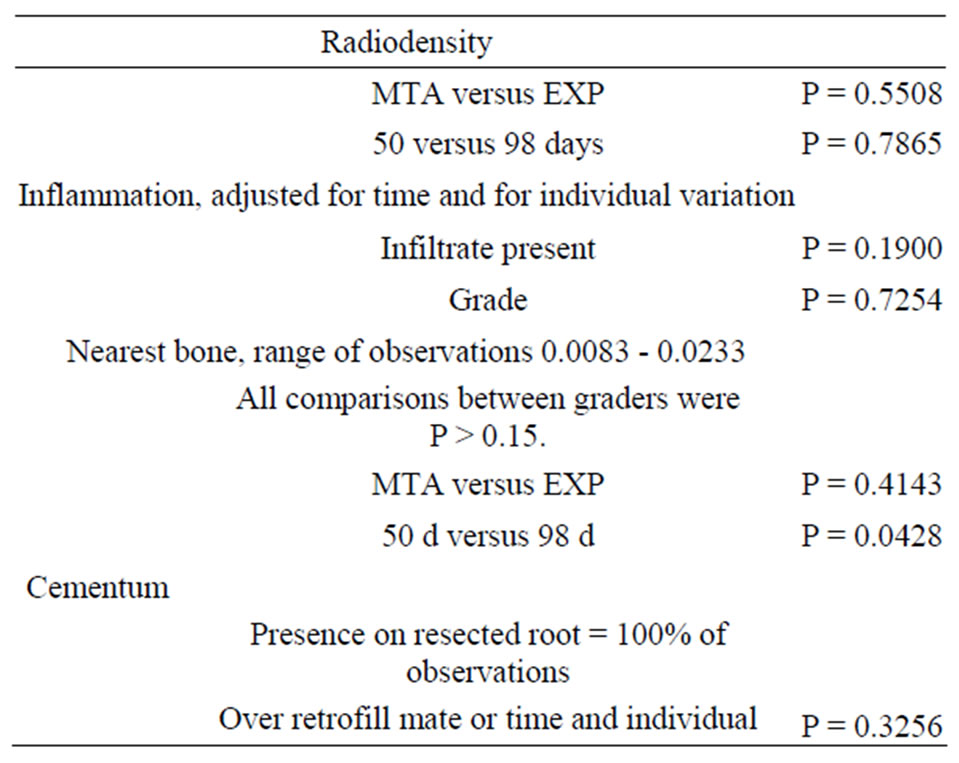
Table 3. Summary of statistical analyses.
al. [8,9]. Rapid bone regeneration at 50 days in this study was confirmed by digital radiography densitometry, cone beam radiography, and histology.
The minimal amount of inflammation, even at 50 days post op, was indicative of this excellent biocompatibility of both materials. Near total bone regeneration and the presence of cementum over some retrofillings is further evidence of the favorable in vivo tissue acceptance of both of these materials.
Asgary and co-workers found cementum covering 11 of 12 MTA retrofills in dogs at 2 months [10]. Individual variability between individual animals was noted in the fact that one dog did not grow any cementum directly over either retrofilling material. In an in vitro study, Hakku and others found cultured cementoblasts were killed by high concentration MTA, whereas lower concentrations were better tolerated. This finding represents a plausible explanation for individual variability, as one animal did not demonstrate cementum overgrowth of either material [11].
This study found no radiographic or histologic differences in classic MTA versus the experimental MTA. Typical, exuberant bone regeneration was demonstrated, as was presence of cementum on or near the classic MTA as well as the experimental retro fillings. The experimental material sets faster and is more easily placed.
REFERENCES
- Torabinejad, M., Watson, T.F. and Pitt-Ford, T.R. (1993) Sealing ability of a mineral trioxide aggregate used as a root end filling material. Journal of Endodontics, 19, 591- 595. doi:10.1016/S0099-2399(06)80271-2
- Parirokh, M. and Torabinejad, M. (2010) Mineral trioxide aggregate: A comprehensive literature review—Part I: Chemical, physical, and antibacterial properties. Journal of Endodontics, 36, 16-27. doi:10.1016/j.joen.2009.09.006
- Torabinejad, M. and Parirokh, M. (2010) Mineral trioxide aggregate: A comprehensive literature review—Part II: Leakage and biocompatibility investigations. Journal of Endodontics, 36, 190-202. doi:10.1016/j.joen.2009.09.010
- Parirokh, M. and Torabinejad, M. (2010) Mineral trioxide aggregate: A comprehensive literature review—Part III: Clinical applications, drawbacks and mechanism of action. Journal of Endodontics, 36, 400-413. doi:10.1016/j.joen.2009.09.009
- von Arx, T., Hanni, S. and Jensen, S.S. (2010) Clinical results with two different methods of root-end preparation and filling in apical surgery: Mineral trioxide aggregate and adhesive resin composite. Journal of Endodontics, 36, 1122-1129. doi:10.1016/j.joen.2010.03.040
- Wang, Y., Cheung, G.S., Xu, X., Zhao, S. and Zhang, C. (2010) The effect of cultured autologous periodontal ligament cells on the healing of delayed autotransplanted dog’s teeth. Journal of Endodontics, 36, 264-267. doi:10.1016/j.joen.2009.09.014
- Brasil, D.S., Soares, J.A., Horta, M.C.R., Ferreira, C.L., Nunes, E., Chaves, G.G. and Silvera, F.F. (2010) Periapical repair in dog teeth: Root canal adhesive filling by using the Resilon system. Journal of Endodontics, 36, 482- 488. doi:10.1016/j.joen.2009.11.020
- Yasuda, F., Ogawa, M., Arakawa, T., Kadowaki, T. and Saito, T. (2008) The effect of mineral trioxide aggregate on the mineralization ability of rat dental pulp cells: An in vitro study. Journal of Endodontics, 34, 1057-1060. doi:10.1016/j.joen.2008.06.007
- Meade, H., Nakano, T., Tomokiyo, A., Fujii, S., Wada, N., Monnouchi, S., Hori, K. and Akamine, A. (2010) Mineral trioxide aggregate induces bone morphogenetic protein-2 expression and calcification in human periodontal ligament cells. Journal of Endodontics, 36, 647-652. doi:10.1016/j.joen.2009.12.024
- Asgary, S., Eghbal, M.J. and Ehsani, S. (2010) Periradicular regeneration after endodontic surgery with calciumenriched mixture cement in dogs. Journal of Endodontics, 36, 837-841. doi:10.1016/j.joen.2010.03.005
- Hakki, S.S., Bozkurt, S.B., Hakki, E.E. and Belli, S. (2009) Effects of mineral trioxide aggregate on cell survival, gene expression associated with mineralized tissues, and biomineralization of cementoblasts. Journal of Endodontics, 35, 513-519. doi:10.1016/j.joen.2008.12.016