Open Journal of Pediatrics
Vol.3 No.1(2013), Article ID:28623,3 pages DOI:10.4236/ojped.2013.31003
Immunadsorption therapy for end stage heart failure due to Duchenne muscular dystrophy*
![]()
1Department of Pediatrics, Caritas Krankenhaus, Bad Mergentheim, Germany
2Department of Internal Medicine III, Nephrology, Caritas Krankenhaus, Bad Mergentheim, Germany
3Department of Internal Medicine I, Cardiology, Universitaet Wuerzburg, Wuerzburg, Germany
Email: #reiner.buchhorn@ckbm.de
Received 11 December 2012; revised 13 January 2013; accepted 22 January 2013
Keywords: Duchenne Muscular Dystrophy; Immunoadsorption Therapy; Heart Failure; Betablocker; Cardiomyopathy
ABSTRACT
We report about a successful immunadsorption therapy of a boy with end stage heart failure due to Duchenne muscular dystrophy who has little chance to get cardiac transplantation. Prior to this therapy a medical therapy with an angiotensin converting enzyme inhibitor, a low dose betablocker, an aldosterone antagonist, and diuretics failed. In consent with the patient and his parents immunoadsorption therapy employing a protein A column was performed. Due to clinical improvement the betablocker carvedilol could be titrated from 6.25 mg up to 30 mg. In the following 4 month he improves from NYHA class IV to NYHA class II and NT-Pro-BNP levels fell from 5180 pg/ml to 402 pg/ml. The mean heart rate in Holter ECG decreases from 102/min to 68/min and ejection fraction improved from 25% to 30%. The boy began to walk without any support and was able to visit school. This clinical improvement now holds on for 2 years.
1. INTRODUCTION
Heart failure is one of the major causes of death in patients with Duchenne muscular dystrophy (DMD)! DMD is an X-linked myopathy-cardiac involvement was characterized by initial pathology descriptions of mycocyte hypertrophy and myocardial fibrosis. Diagnosis of heart failure based on reduced wall motion in echocardiogramphy, elevated heart rate in Holter ECG and neurohormonal activation with elevated NT-Pro BNP values. DMD patients with biopsy-proven acute or persistent myocardial inflammation had a rapid progression to heart failure and death in contrast to those without evidence of myocarditis [1].
To date, a guideline for the management of heart failure in pediatric patients have been published in 2004 by the International Society of Heart and Lung Transplantation. Because clinical data are scarce, the use of betablockers is not recommended in children with stage D heart failure [2].
Immunoadsorption therapy has been shown to reduce cardio-noxious antibodies, such as cardiostimulatory antibodies targeting the beta1-adrenergic receptor [3]). A first series of clinical pilot studies suggests indeed that immunoadsorption therapy might have beneficial effects in selected patients with idiopathic dilated cardiomyopathy [4]. Recently published data show that removal of β(1)-adrenoceptor-autoantibodies by immunadsorption can improve cardiac function allowing long-term stability in end-stage dilated cardiomayopathy, which can spare many patients from heart transplantation [5].
2. CASE REPORT
A 15 years old boy with Duchenne muscular dystrophy (DMD) presented in our hospital with dyspnea and loss of mobility within the last 4 weeks. Physical examination showed orthopnea, tachypnea, hepatomegaly and peripheral edema. Electrocardiography (ECG) showed sinus rhythm and normal time intervals without intraventricular conduction delay. Holter-ECG displayed an elevated mean heart rate of 102 bpm and 2900 ventricular premature beats within 24 hours. Echocardiography displayed enlargement of the left ventricle, moderate insufficiency of the mitral valve, and severely impaired left ventricular systolic function. Laboratory parameters showed normal troponin T (0.083 ng/ml) and highly elevated NT-Pro brain natriuretic peptide (NT-proBNP) levels (5180 pg/ml). Infection with cardiotropic viruses including Coxsackie, Epstein Barr, Parvovirus, Influenca A and B were not detected. However, highly elevated cyto-
Table 1. Clinical, hemodynamic and biochemical measurements during the therapeutic interventions.
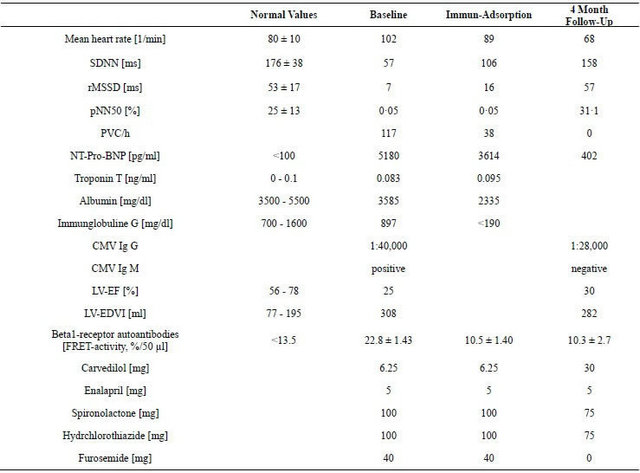
SDNN: Standard deviation of all NN intervals; rMSSD: Square root of the mean of the sum of the squares of differences between adjacent NN intervals; pNN50: Number of pairs of adjacent NN intervals differing by more than 50 ms divided by the total number of all NN intervals; PVC: Premature ventricular contraction; CMV: Cytomegaly virus; LV-EF: Left ventricular ejection fraction; LV-EDVI: Left ventricular enddiastolic volume index.
megaly (CMV) IgG and positive IgM antibody-titers were highly suggestive of CMV infection but CMV DNA was not detected by polymerase chain reaction. Magnetic resonance imaging of the heart revealed severe left ventricular dilatation and a markedly reduced ejection fraction of 25%.
A standard heart failure therapy was started immediately including an ACE inhibitor (enalapril 5 mg per day), a betablocker (carvedilol 6.25 mg per day), an aldosterone antagonist (spironolactone 100 mg per day), and diuretics (furosemide and hydrochlorothiazide). After a weight loss of 5 kg his clinical condition improved but he remained confined to bed. Due to hypotension and tachypnea betablocker therapy could not be up-titrated adequately and the boy decompensated again 4 weeks later. Because of DMD heart transplantation was not a realistic option.
In consent with the patient and his parents immunoadsorption therapy employing a protein A column (ImmunosorbaTM; Fresenius Medical Care, Germany) was performed as previously described (4). Vascular access was via an internal jugular double lumen catheter and a microprocessor controlled elution monitor pumped plasma between two Immunosorba columns. The daily treatment time was 3 - 5 h during which approximately two patient blood volumes were processed through 20 - 30 adsorption cycles per column. Total immunoglobulin G fractions were determined on treatment Days 1 - 5. Without immunoglobulin-substitution the total immungobulin G titers decreased from 897 mg/dl below 190 mg/dl.
In the following 4 months we observed an impressive clinical improvement from NYHA class IV to NYHA class II. The boy began to walk without any support and to visit school 6 weeks later. Due to this improvement the daily dose of carvedilol could be up-titrated from 6.25 - 30 mg, and finally, even furosemide therapy was stopped without any signs of recurrence of congestion. NT-proBNP levels decreased from 5180 to 402 pg/ml and right ventricular pressure as derived from the velocity of tricuspid valve regurgitation fell to normal. By cardiac magnetic resonance imaging left ventricular ejection fraction improved from 25% to 30%. Regarding the suspected CMV infection sero-conversion from CMV IgM positive to negative occured. The elevated levels of cardiostimulatory β(1)-adrenoceptor-autoantibodies fell to normal values after immunoadsorption therapy and remained stable over 4 months. Holter ECG 4 month after immunadsorption therapy under a daily dose of 30 mg carvedilol, 5 mg enalapril, 75 mg spironolactone and 25 mg hydrochlorothiazide revealed a mean heart rate of 68 bpm, only 11 premature ventricular beats and normal heart variability.
3. DISCUSSION
To the best of our knowledge this case report is the first about immunoadsorption therapy in Duchenne cardiomyopathy. Some recently published retrospective studies [6] and currently one clinical trial in Japan [7] examine if low-dose carvedilol may prevent cardiac dysfunction in children with DMD, but unfortunately nothing is known how to treat severe heart failure in these children. Due to bad long-time prognosis and the lack of organ donors heart transplantation was no realistic option. Like other patients with DMD-associated left ventricular dysfunction our patient had a normal QRS duration and would probably not profit from cardiac resynchronization therapy (CRT) [8]. Recently published data show myocarditis as a precipitating factor for heart failure in DMD with a high impact on prognosis [1]. We found cardiostimulatory β(1)-adrenoceptor-autoantibodies that are known to be involved in the initiation and progression of idiopathic cardiomyopathy and may predict increased mortality [9]. Various studies with a limited number of patients indicate that the use of immunoadsorption to eliminate immunoglobulin G significantly improves cardiac performance and clinical status in heart failure patients [4]. Our concept to take advantage of this possible clinical improvement by immunoadsorption therapy to up titrate carvedilol therapy from 5 mg to 30 mg daily in our patients was very successful. Like shown in the Table 1 all prognostic important parameters like NT-proBNP, mean heart rate, ventricular arrhythmias and heart rate variability improve. This clinical improvement now holds on for 2 years.
4. CONCLUSION
Cardio-noxious antibodies, such as cardiostimulatory anti beta1-adrenoceptor autoantibodies, may contribute to progressive left ventricular dysfunction and ventricular arrhythmias in children with DMD. Immunoadsorption therapy together with carvedilol treatment may be beneficial in patients with DMD and end stage heart failure most of all if β(1)-adrenoceptor-autoantibodies are detectable.
REFERENCES
- Mavrogeni, S., Papavasiliou, A., Spargias, C., Constandouklakis, P., Papadopoulos, G., Karanasios, E., et al. (2010) Myocardial inflammation in Duchenne muscular dystrophy as a precipitating factor of heart failure: A prospective study. BMC Neurology, 10, 33-40. doi:10.1186/1471-2377-10-33
- Rosenthal, D., Chrisant, M.R., Edens, E., Mahony, L., Canter, C., Colan, S., et al. (2004) International society for heart and lung transplantation: Practice guidelines for management of heart failure in children. Journal of Heart Lung Transplant, 23, 1313-1333. doi:10.1016/j.healun.2004.03.018
- Nikolaev, V.O., Boivin, V., Störk, S., Angermann, C.E., Ertl, G. and Lohse, M.J. (2007) A novel fluorescence method for rapid detection of functional β1-adrenergic receptor autoantibodies in heart failure. Journal of the American College of Cardiology, 50, 423-431. doi:10.1016/j.jacc.2007.03.051
- Ikeda, U., Kasai, H., Izawa, A., Koyama, J., Yazaki, Y., Takahashi, M., et al. (2008) Immunoadsorption therapy for patients with dilated cardiomyopathy and heart failure. Current Cardiology Reviews, 4, 219-222. doi:10.2174/157340308785160534
- Dandel, M., Wallukat, G., Englert, A., Lehmkuhl, H.B., Knosalla, C. and Hetzer, R. (2012) Long-term benefits of immunadsorption in β(1)-adrenoceptor-autoantibody-positive transplant candidates with dilated cardiomyopathy. European Journal of Heart Failure, 14, 1374-1388. doi:10.1093/eurjhf/hfs123
- Kajimoto, H., Ishigaki, K., Okumura, K., Tomimatsu, H., Nakazawa, M, Saito, K., et al. (2006) Beta-blocker therapy for cardiac dysfunction in patients with muscular dystrophy. Circulation Journal, 70, 991-994. doi:10.1253/circj.70.991
- Nishizawa, T. and Yasuma, F. (2007-2012) The preventive efficacy of carvedilol on cardiac dysfunction in duchenne muscular dystrophy. Clinicaltrials.gov Indentifier. Current Study NCT00606775.
- Hor, K.N., Wansapura, J.P., Al Khalidi, H.R., Gottliebson, Taylor, M.D., Czosek, R., et al. (2011) Presence of mechanical dyssynchrony in Duchenne muscular dystrophy. Journal of Cardiovascular Magnetic Resonance, 13, 12. doi:10.1186/1532-429X-13-12
- Stork, S., Boivin, V., Horf, R., et al. (2006) Stimulating autoantibodies directed against the cardiac beta1-adrenergic receptor predict increased mortality in idiopathic cardiomyopathy. American Heart Journal, 152, 697-704. doi:10.1016/j.ahj.2006.05.004
NOTES
*Conflict of interest: There is no conflict of interest, no funding of this study ocurred. None of the authors has financial interest.
#Corresponding author.