Paper Menu >>
Journal Menu >>
 Psychology, 2010, 1, 229-232 doi:10.4236/psych.2010.14030 Published Online October 2010 (http://www.SciRP.org/journal/psych) Copyright © 2010 SciRes. PSYCH 229 The Impact of Sociodemographic Factors on Knowledge of Cardiac Procedures Samara Lipsky1, Michael Bohnen2, Janice Barnhart3 1Department of Psychology, Yeshiva University, Bronx, USA; 2Columbia University, New York, USA; 3Department of Epidemi- ology and Population Health, Albert Einstein College of Medicine, Bronx, USA. Email: SamaraLipsky@alum.emory.edu Received July 19th, 2010; revised July 26th, 2010; accepted August 3rd, 2010. ABSTRACT Background: This paper investigates the extent to which sociodemographic factors are associated with knowledge of cardiac procedures in a sample of study participants treated for coronary heart disease (CHD). Research indicates the importance of knowledge of CHD and its associated risks in order to prevent CHD. However, quantification of knowl- edge levels among individuals undergoing cardiac procedures to treat CHD has not been well documented. Method: Using a cross-sectional design, 156 participants, diverse in race/ethnicity, age, and sex, underwent elective cardiac catheterization for the evaluation of chest pain and/or angina. Participants completed surveys regarding medical his- tory, sociodemographic information, and knowledge of cardiac procedures. Ninety-five of these individuals, with clini- cally significant CHD, were recommended by their physician to undergo a coronary revascularization procedure [per- cutaneous transluminal coronary angioplasty (PTCA) or coronary artery bypass graft (CABG)]. These individuals completed additional knowledge assessment surveys. Results: The overall knowledge scores for those undergoing coronary angiography were suboptimal (M score = 4.6 out of 8). Older aged (> 65), male, married, white, col- lege-educated participants demonstrated greater knowledge of cardiac catheterization procedures (all p values < 0.05). Knowledge scores were greater among those revascularized than among participants undergoing coronary angiogra- phy. Conclusions: Health professionals should provide general information about CHD treatment and interventions, especially among women and ethnic minorities. Keywords: Coronary Heart Disease, Knowledge, Cardiac Procedure 1. Introduction Coronary heart disease (CHD) is the primary cause of death for adults in the United States [1,2]. Numerous reports outline disparities in knowledge of cardiovascular disease among different sociodemographic groups for individuals with CHD based on race/ethnicity and sex [3,4]. For example, Woodard and colleagues (2005) found that African Americans demonstrated less knowl- edge regarding risk factors for cardiovascular disease, compared to Caucasians. The lesser knowledge that Af- rican Americans demonstrated regarding risk factors of cardiovascular disease may directly correlate with the finding that African American women with multiple car- diac risk factors underestimated their risk for heart dis- ease [5]. Furthermore, Mosca and colleagues (2000) sur- veyed over 1,000 women and found that only 8% recog- nized CHD or stroke as their greatest health concern and less than one-third identified CHD as a leading cause of death. Thus, lack of knowledge regarding personal risk of CHD may impact decision-making regarding risk prevention, and this impact may be heightened among sociodemographic groups under-educated on the risks and prevention of cardiovascular disease. Few studies have examined the origin of the dispari- ties in knowledge of CHD based on race/ ethnicity and sex among individuals with CHD [3,4]. The root cause might include the effect of a previously unmeasured non-clinical factor: knowledge of the risks and benefits of cardiac procedures, including coronary angiography and revascularization (i.e. percutaneous transluminal coronary angioplasty [PTCA] or coronary artery bypass graft [CABG]) [3]. Determining if knowledge affects individuals’ decision-making might aid in understand- ing disparities in the provisions of the use of coronary angiography or revascularization [6,7]. Moreover, if knowledge levels of these cardiac procedures vary along sociodemographic lines, the root of the disparity in know-  The Impact of Sociodemographic Factors on Knowledge of Cardiac Procedures Copyright © 2010 SciRes. PSYCH 230 ledge of individuals with cardiovascular disease may be targeted further. 2. Method 2.1. Participants Individuals who met the following criteria were invited to participate in the study: 1) ≥ 40 years of age; 2) un- dergoing angiography for chest pain/pressure and/or an- gina equivalents; and 3) able to give informed consent. Out of 217 individuals eligible for the study, 181 agreed to participate, and we obtained complete data from 156 participants. These 156 participants had their knowledge level of the catheterization they were about to undergo assessed. Ninety-five of these individuals had their knowledge level of their subsequent revascularization procedure assessed via bedside survey. 2.2. Procedure Knowledge of cardiac procedures was investigated among male and female participants scheduled for coronary an- giography at an academic medical center in the Bronx. These individuals were identified weekly using the logs at this medical center. Trained interviewers abstracted infor- mation from medical log books to locate eligible partici- pants. Once located, individuals were asked to be inter- viewed at bedside and permission was granted to access their health information. 2.3. Measures Following the baseline interview, medical record ab- stractors used standardized forms to collect detailed in- formation on medical history, angiography results, and angina severity as classified by the Canadian Cardiovas- cular Society [8]. These forms consisted of the following items: age, race/ethnicity, sex, marital and employment status, level of education, insurance, medical history, angiography results, and treatment received. In addition, all respondents completed eight true-false questions re- garding knowledge of coronary angiography. One point was assigned to each correct response (possible score 0 to 8). All individuals with clinically significant CHD that underwent a revascularization procedure (i.e. PTCA or CABG) also completed a survey pertaining to their re- spective procedures. These surveys contained a mix of true/false and multiple choice questions (possible scores for CABG = 0 to 10; for PTCA = 0 to11). A higher mean score indicated that the individual had greater knowledge of his or her corresponding procedure. 2.4. Statistical Analysis We used descriptive statistics (e.g. percentages, means, standard deviations) to characterize the study population. Univariate analyses allowed us to calculate the crude rates for coronary angiography and revascularization (i.e. PTCA and CABG) according to the patients’ demo- graphic characteristics. We determined significant asso- ciations with chi-square tests for categorical variables (e.g. sex) and student’s t-tests for continuous variables (e.g. age, knowledge scores). Marital status was coded as married and not married (single, separated, divorced and widowed). Age was dichotomized to 65 years and > 65 years based on the study population. Race/ethnicity was coded as white and non-white (African American, His- panic, Native American, Asian, and other). Level of edu- cation was coded as college degree (college, graduate school) and no college degree (high school, high school diploma, some college experience but no degree obta- ined). We calculated knowledge of cardiac procedures by summing the number of correct responses to the an- giography, PTCA, and CABG questions. 3. Results 3.1. Sociodemographic Characteristics The study’s sample included 156 participants ranging in age from 42 to 96 (mean = 69.2; SD = 9.5 years) and the majority were women (93 females, 59.6% of partici- pants). The major racial/ethnic groups were white (56%), non-Hispanic black (18%), and Hispanic (16%). The majority of participants had private insurance (60%) or Medicare (20%). Most individuals had at least two risk factors for CHD, hypertension and hypercholesterolemia the most prevalent among them. Chronic stable angina (moderate-severe) was the most common presenting symptom. Fifty-eight percent of the participants had mild-moderate CHD (i.e. at least 50% blockage of a main heart artery) and PTCA was the more common revascu- larization procedure performed (54%). Demographic characteristics and clinical data of the study population are displayed in Table 1. 3.2. Knowledge of Angiography Knowledge levels of coronary angiography varied sig- nificantly according to an individual’s sociodemographic background. The overall mean score for the eight an- giography knowledge questions was 4.6 (SD = 1.7) as shown in Table 2. Scores ranged from 0 (n = 2) to 8 (n = 3). Participants who were over 65 years of age, male, married, college educated, and white had higher mean knowledge scores for cardiac catheterizations than their respective counterparts (p < 0.05 for all comparisons). Participants who were employed were more knowle- dgeable about their procedures as well. 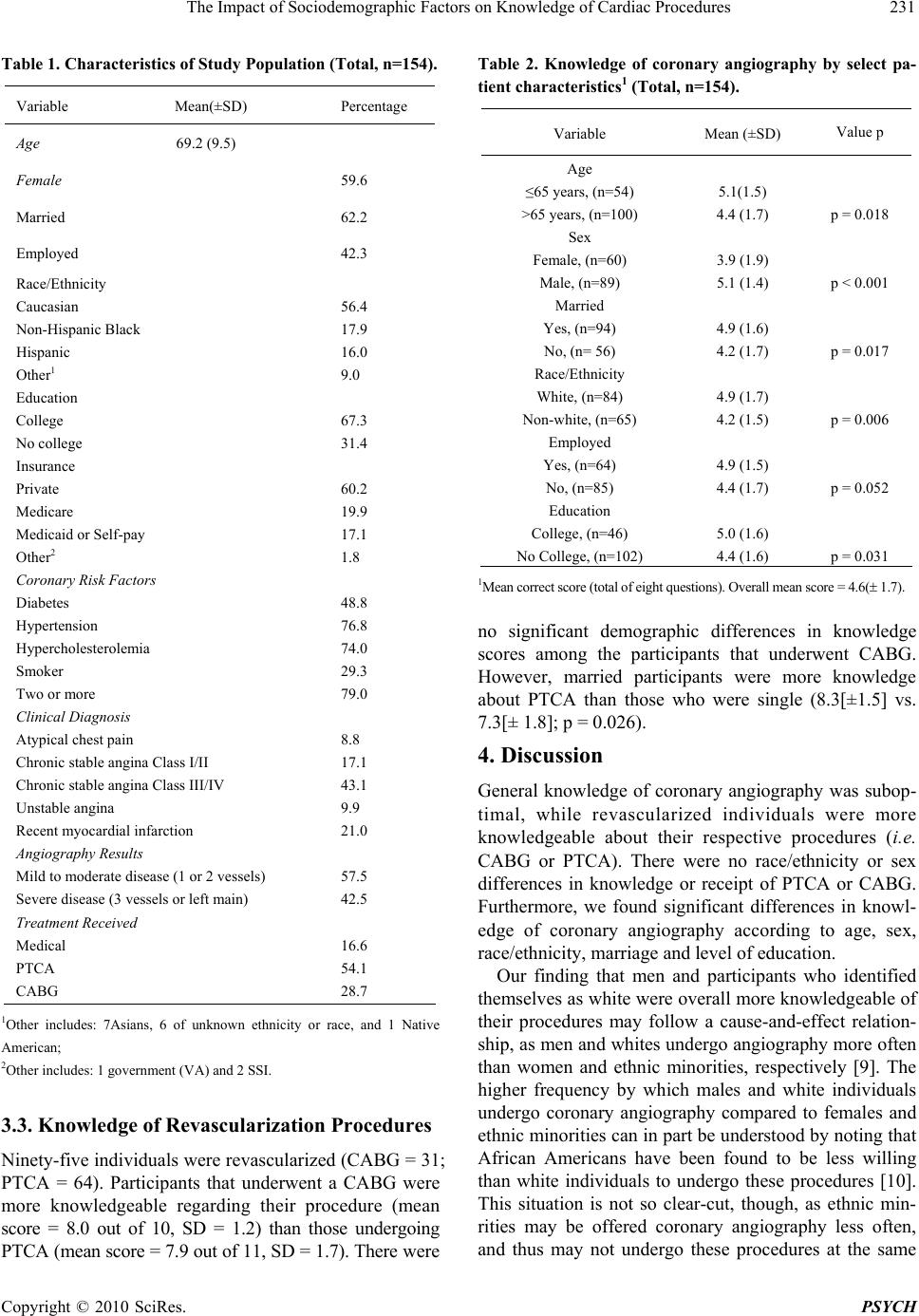 The Impact of Sociodemographic Factors on Knowledge of Cardiac Procedures Copyright © 2010 SciRes. PSYCH 231 Table 1. Characteristics of Study Population (Total, n=154). Variable Mean(±SD) Percentage Age 69.2 (9.5) Female 59.6 Married 62.2 Employed 42.3 Race/Ethnicity Caucasian Non-Hispanic Black Hispanic Other1 56.4 17.9 16.0 9.0 Education College No college 67.3 31.4 Insurance Private Medicare Medicaid or Self-pay Other2 60.2 19.9 17.1 1.8 Coronary Risk Factors Diabetes Hypertension Hypercholesterolemia Smoker Two or more 48.8 76.8 74.0 29.3 79.0 Clinical Diagnosis Atypical chest pain Chronic stable angina Class I/II Chronic stable angina Class III/IV Unstable angina Recent myocardial infarction 8.8 17.1 43.1 9.9 21.0 Angiography Results Mild to moderate disease (1 or 2 vessels) Severe disease (3 vessels or left main) 57.5 42.5 Treatment Received Medical PTCA CABG 16.6 54.1 28.7 1Other includes: 7Asians, 6 of unknown ethnicity or race, and 1 Native American; 2Other includes: 1 government (VA) and 2 SSI. 3.3. Knowledge of Revascularization Procedures Ninety-five individuals were revascularized (CABG = 31; PTCA = 64). Participants that underwent a CABG were more knowledgeable regarding their procedure (mean score = 8.0 out of 10, SD = 1.2) than those undergoing PTCA (mean score = 7.9 out of 11, SD = 1.7). There were Table 2. Knowledge of coronary angiography by select pa- tient characteristics1 (Total, n=154). Variable Mean (±SD) Value p Age ≤65 years, (n=54) >65 years, (n=100) 5.1(1.5) 4.4 (1.7) p = 0.018 Sex Female, (n=60) Male, (n=89) 3.9 (1.9) 5.1 (1.4) p < 0.001 Married Yes, (n=94) No, (n= 56) 4.9 (1.6) 4.2 (1.7) p = 0.017 Race/Ethnicity White, (n=84) Non-white, (n=65) 4.9 (1.7) 4.2 (1.5) p = 0.006 Employed Yes, (n=64) No, (n=85) 4.9 (1.5) 4.4 (1.7) p = 0.052 Education College, (n=46) No College, (n=102) 5.0 (1.6) 4.4 (1.6) p = 0.031 1Mean correct score (total of eight questions). Overall mean score = 4.6( 1.7). no significant demographic differences in knowledge scores among the participants that underwent CABG. However, married participants were more knowledge about PTCA than those who were single (8.3[±1.5] vs. 7.3[± 1.8]; p = 0.026). 4. Discussion General knowledge of coronary angiography was subop- timal, while revascularized individuals were more knowledgeable about their respective procedures (i.e. CABG or PTCA). There were no race/ethnicity or sex differences in knowledge or receipt of PTCA or CABG. Furthermore, we found significant differences in knowl- edge of coronary angiography according to age, sex, race/ethnicity, marriage and level of education. Our finding that men and participants who identified themselves as white were overall more knowledgeable of their procedures may follow a cause-and-effect relation- ship, as men and whites undergo angiography more often than women and ethnic minorities, respectively [9]. The higher frequency by which males and white individuals undergo coronary angiography compared to females and ethnic minorities can in part be understood by noting that African Americans have been found to be less willing than white individuals to undergo these procedures [10]. This situation is not so clear-cut, though, as ethnic min- rities may be offered coronary angiography less often, and thus may not undergo these procedures at the same  The Impact of Sociodemographic Factors on Knowledge of Cardiac Procedures Copyright © 2010 SciRes. PSYCH 232 high frequency. Nevertheless, a possible greater unwill- ingness of African Americans to undergo coronary an- giography compared to white individuals corresponds with findings that African Americans are less likely than white individuals to feel that their physicians have a par- ticipatory style of decision making [11]. Whether African Americans demonstrate low knowledge of coronary an- giography due to a lack of trust in their physician is an important consideration. Most of our respondents were older individuals and had multiple cardiovascular risk factors. Therefore, they might have had a previous cardiac procedure. Moreover, most of our study participants were referred by their pri- mary care physicians or cardiologists for their cardiac interventions. These two key characteristics of our study participants suggest that knowledge among participants may have varied depending on when in the course of their disease they interacted with a physician or subspe- cialist, or due to a systematic factor related to patient communication. Alternatively, the lower education level may have led to health illiteracy leading to lack of access to or integration of available knowledge. These variables warrant further study. This study has limitations. We surveyed participants at one academic institution, thus our results may have lim- ited generalizability. We did not detect significant dif- ferences in knowledge among the represented sociode- mographic groups regarding CABG and PTCA. A larger sample size may have shed light on this uncertainty. While we only found significant sociodemographic differences in levels of knowledge for coronary an- giography and not for the revascularization procedures (CABG and PCTA) surveys, it is important to consider the nature of the questions we asked our study partici- pants. While we tried to administer questions with a similar range of difficulty in all surveys, we cannot be fully confident that our questions offered a most precise gauge of knowledge for each procedure. 5. Conclusions In this study, sociodemographic variables appeared to be associated with knowledge levels in individuals under- going coronary angiography. These same variables did not produce significant differences in knowledge levels of individuals undergoing revascularization procedures. Earlier findings that knowledge of cardiovascular disease itself is low among under-educated sociodemographic groups may support our finding that these groups demon- strate low knowledge levels of related cardiac procedures. Disparity in knowledge among individuals undergoing coronary angiography warrants further study. Moreover, empowering individuals with CHD with greater knowl- edge of life-style or procedural treatments for CHD should enhance health promotion, which may improve individu- als’ quality of life before and after cardiac interventions. Adequate access to and integration of available knowl- edge becomes particularly important for individuals with CHD who may benefit from more timely access to medical care. REFERENCES [1] Center for Disease Control, “Heart Disease Facts: America’s Heart Disease Burden,” 2006. [2] L. Mosca, W. K. Jones, K. B. King, P. Ouyang, R. F. Redberg, M. N. Hill, et al., “Awareness, Perception, and Knowledge of Heart Disease Risk and Prevention among Women in the United States,” Archives of Family Medicine, Vol. 9, No. 6, 2000, pp. 506-515. [3] A. H. Christian, W. Rosamond, A. R. White and L. Mo- sca, “Nine-Year Trends and Racial and Ethnic Disparities in Women’s Awareness of Heart Disease and Stroke: An American Heart Association National Study,” Journal of Womens Health, Vol. 16, No. 1, 2007, pp. 68-81. [4] H. M. Prendergast, E. B. Bunney, T. Roberson and T. Davis, “Knowledge of Heart Disease among Women in an Urban Emergency Setting,” Journal of the National Medical Association, Vol. 96, No. 8, 2004, pp. 1027-1031. [5] K. B. DeSalvo, J. Gregg, M. Kleinpeter, B. R. Pedersen, A. Stepter and J. Peabody, “Cardiac Risk Underesti- mation in Urban, Black Women,” Journal of General Internal Medicine, Vol. 20, No. 12, 2005, pp. 1127-1131. [6] J. M. Barnhart and S. Wassertheil-Smoller, “The Effect of Race/Ethnicity, Sex, and Social Circumstances on Coro- nary Revascularization Preferences: A Vignette Compari- son,” Cardiology in Review, Vol 14, No. 5, 2006, pp. 215-222. [7] E. H. Bradley, S. A. McGraw, L. Curry, A. Buckser, K. L. King, S. V. Kasl, et al., “Expanding the Andersen Model: The Role of Psychosocial Factors in Long-Term Care Use,” Health Services Research, Vol. 37, 2002, No. 5, pp. 1221-1242. [8] L. Campeau, “Grading of Angina-Pectoris,” Circulation, Vol. 54, No. 3, 1976, pp. 522-523. [9] N. R. Kressin, J. A. Clark, J. Whittle, M. East, E. D. Pe- terson, B. H. Chang, et al., “Racial Differences in Health- Related Beliefs, Attitudes, and Experiences of VA Car- diac Patients: Scale Development and Application,” Med- ical Care, Vol. 40, No. 1, 2002, pp. 72-85. [10] N. R. Kressin, B. H. Chang, J. Whittle, E. Peterson, J. A. Clark, A. K. Rosen, et al., “Racial Differences in Cardiac Catheterization as a Function of Patients’ Beliefs,” American Journal of Public Health, Vol. 94, No. 12, 2004, pp. 2091-2097. [11] L. Cooper-Patrick, J. J. Gallo, J. J. Gonzales, H. T. Vu, N. R. Powe, C. Nelson, et al., “Race, Gender, and Part- nership in the Patient-Physician Relationship,” Journal of the American Medical Association, Vol. 282, No. 6, 1999, pp. 583-589. |