Q. Y. DAI ET AL. 27
symptoms were varies from mild chest not comfortable
to syncope or heart failure, the lack of serious symptoms
besides well-developed collateral vessels, may also been
due in part to systemic hypertension, which preserved
antegrade blood flow in the RCA [4]. Occurrence is gen-
erally no predilection in sex or race, and is not consid-
ered an inheritable congenital heart defect. In our study,
all 8 patients are Chinese, female predominant and with-
out combined with intra-cardiac disease.
ECG-gated MDCT angiography findings of ALCAPA
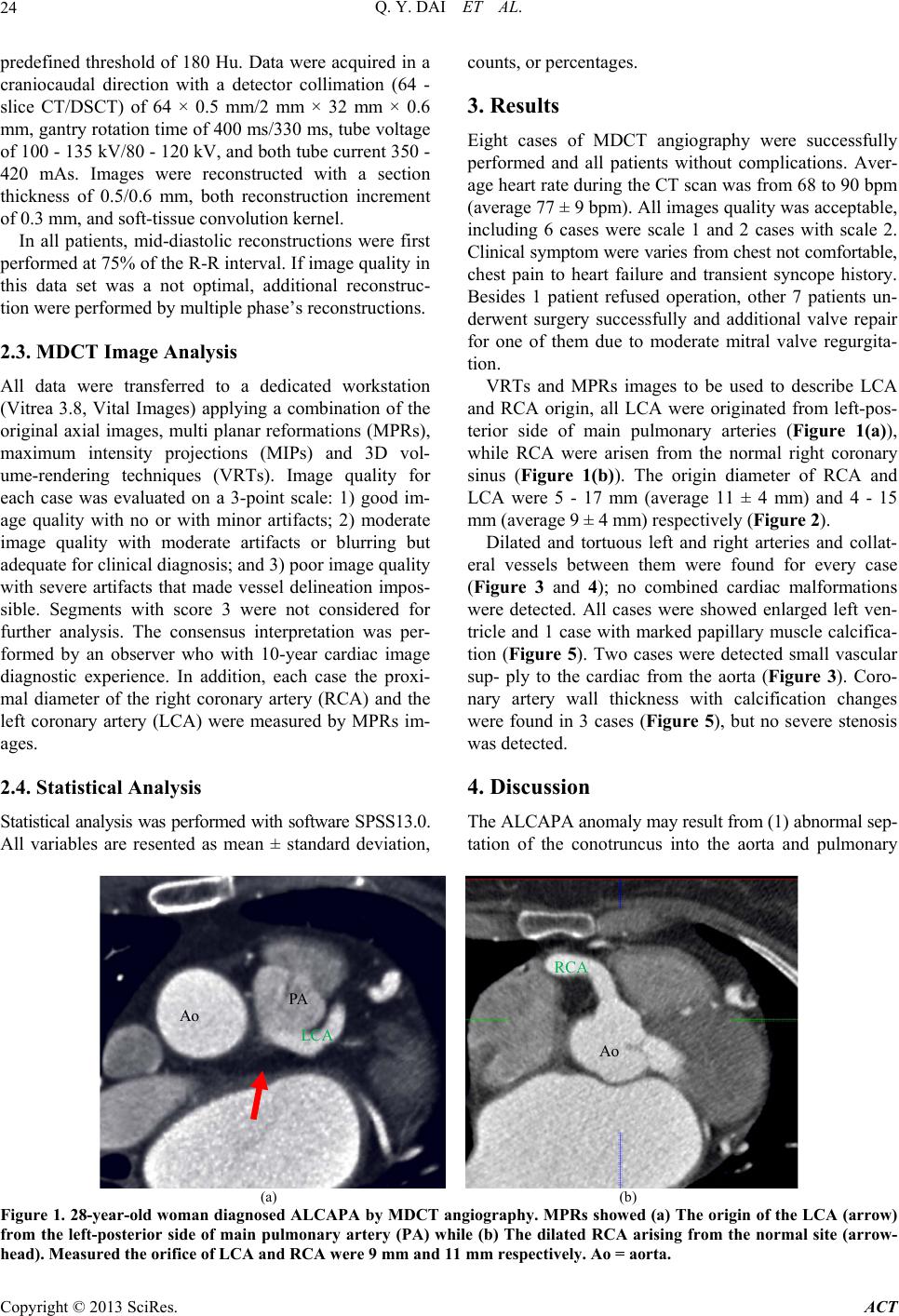
in adults include direct visualization of the LCA original
from the main pulmonary artery, which is the diagnostic
key point viewed by MIPs and VRTs, the LCA typically
arises from the left-posterior aspect of the main pulmo-
nary artery beyond the pulmonary valve (Figure 1(a)),
which were the most common position, however, its po-
sition within the sinus is extremely variable, particularly
it may be very close to a valvular commissure (Figure
5(a)). Rarely, the anomalous ostium originates from the
right posterior sinus or even one of the main pulmonary
arteries. To know the exact LCA origin position may
help the surgical doctor to determine the optional opera-
tion method. In our study, 7 of 8 cases allowed operation
successfully, including direct re-implantation (n = 3) and
Takeuchi (n = 4) surgery. Such images give the surgeons
a better understanding of the complex anatomy before re-
pair.
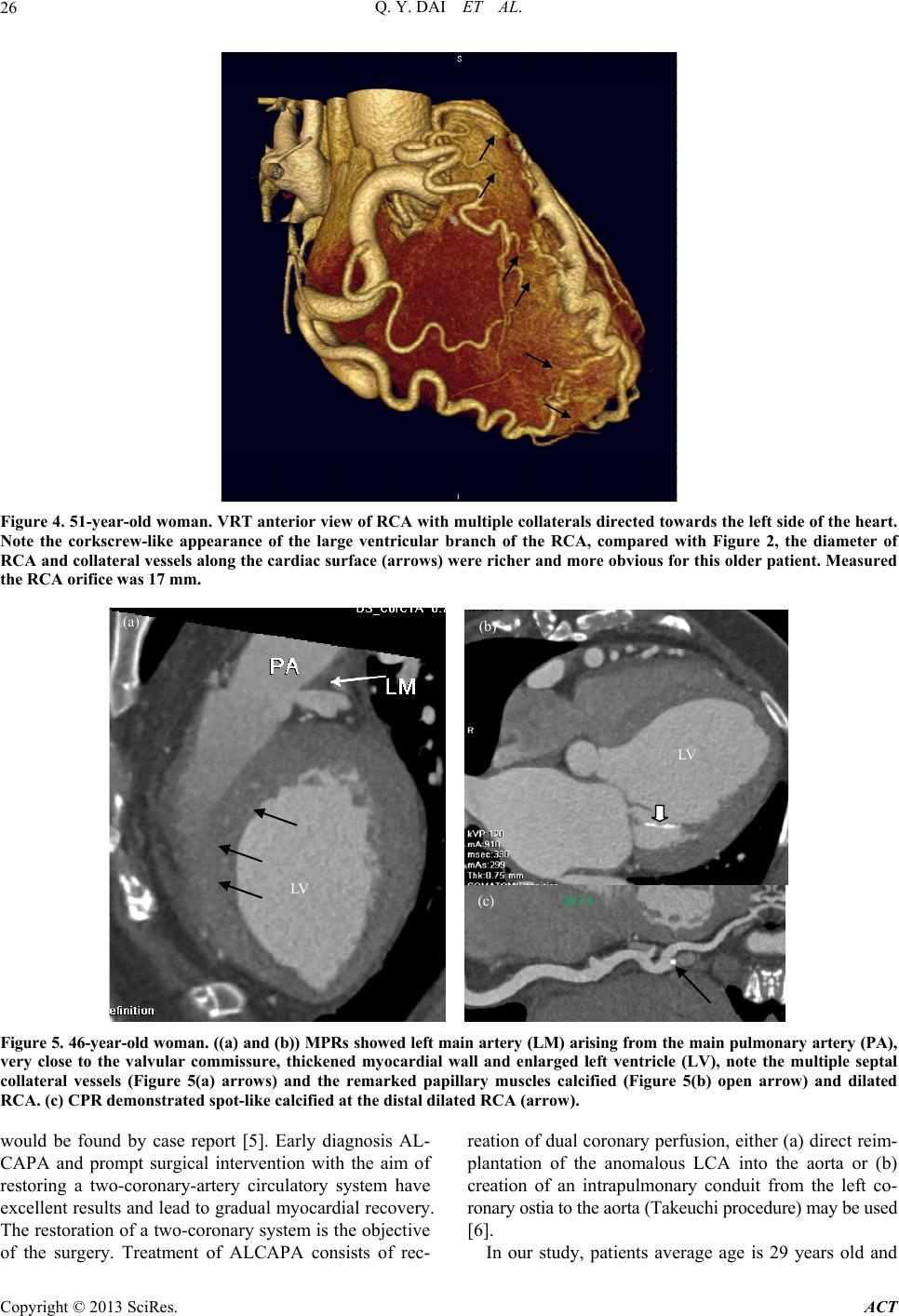
The remarkable secondary imaging finding is the RCA
and the LCA dilated and tortuous, and dilated intracoro-
nary collateral arteries are seen along the epicardial sur-
face of the heart by VRTs (Figure 3(a)) or within the
interventricular septum by MIPs or MPRs (Figure 5(a)).
All cases represent the well-developed collateral path-
ways between the RCA and the LCA, MDCT images
offers excellent spatial resolution, which is required to
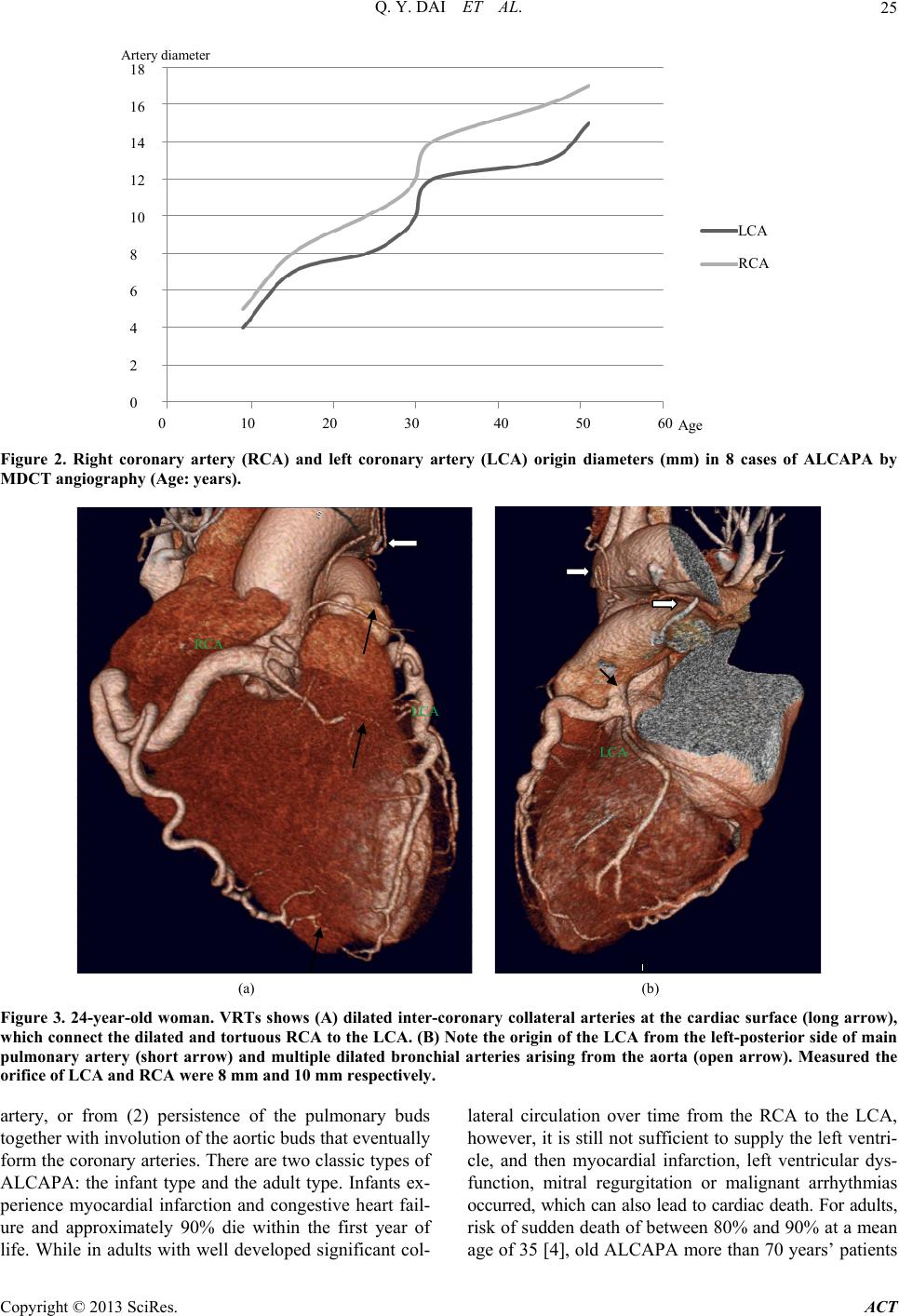
assess small vessels such as the coronary arteries. In our
study, the dilated degree of both the RCA and the LCA
marked with ages, the diameter of RCA for each case
were a mild wider than that of left one (Table 2, Figure
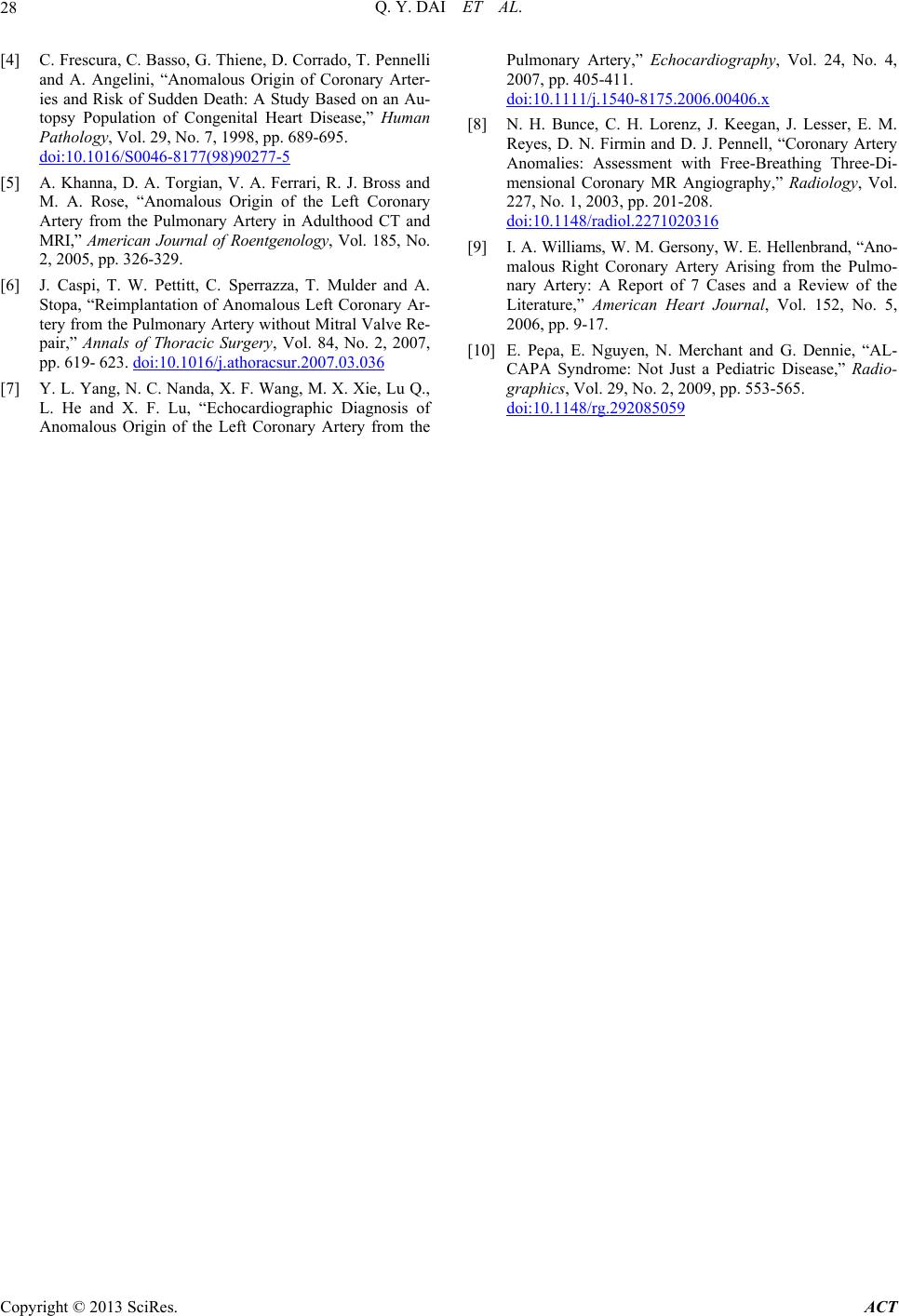
1 and 3), and collateral vessels along the cardiac surface
were richer for older patients (Figure 4). Moreover, the
dilated bronchial arteries from the aorta (Figure 3),
which act as systemic collateral vessels to the LCA
area’s blood supply, are best depicted at ECG-gated
MDCT angiography because of their small size.
Besides, left ventricular hypertrophy and dilatation
result from chronic myocardial ischemia also be seen in
MDCT images (Figure 5), may be used to assess left
ventricular function. If ischemia of the papillary muscles
happened and adjacent myocardium may cause mitral
insufficiency, as a finding, papillary muscles calcified
can easily be seen at MPRs besides left ventricle en-
larged (Figure 5(b)).
Due to the marked dilatation develops over time as
blood is rapidly shunted from the RCA into the LCA and
then into the low-pressure pulmonary circulation, the de-
generation change of the coronary artery could be found
in our mean age 29 years ALCAPA group (Figure 5(c)).
2D echocardiography with Doppler color flow map-
ping in some situations replaces angiography [7], echo is
sensitive to determine the mitral valve and left ventricle
function, which is also a convenient method used for fol-
low-up. Another technique used to non-invasively image
the coronary arteries is MR angiography, MR could ac-
curately depict the origin and proximal course of anoma-
lous coronary arteries [8] and no radiation exposure, even
more crucial for MR is the ability to assess myocardial
viability, which can be used as an important prognostic
factor to consider by the surgical doctor. Conventional
coronary angiography still remains as a gold standard for
the diagnosis of anomalous coronary arteries; however, it
is invasive and limited to a projection two-dimensional
view of the complex coronary artery system [9], especial-
ly for the retrograde ostium.
ALCAPA should be different with other disease which
may cause coronary artery dilated, such as Kawasaki di-
sease, coronary artery fistula or secondary to the athe-
rosclerosis change, the essential feature is to show and
determine the LCA origin area.
ECG-gated MDCT angiography plays an important
role as a first-line modality in assessment of ALCAPA,
and MDCT angiography also would be a valuable evalu-
ated post-operation condition [10]. But our study is lim-
ited both by its retrospective nature and a relatively small
number of patients. Because of potential drawbacks of
MDCT such as radiation exposure and contrast medium-
related complications, performing MDCT should be limi-
ted to patients presenting symptoms suggesting the pres-
ence of anomalous coronary arteries.
REFERENCES
[1] H. Brooks, “Two Cases of an Abnormal Coronary Artery
of the Heart Arising from the Pulmonary Artery: With
Some Remarks upon the Effect of This Anomaly in Pro-
ducing Circoid Dilation of the Vessels,” Journal of Anat-
omy and Physiology, Vol. 20, No. 1, 1885, pp. 26-29.
[2] J. C. Post, A. C. van Rossum, J. G. Bronzwaer, C. C. de
Cock, M. B. Hofman and J. Valk, “Magnetic Resonance
Angiography of Anomalous Coronary Arteries. A New
Gold Standard for Delineating the Proximal Course?”
Circulation, Vol. 92, No. 11, 1995, pp. 3163-3171.
doi:10.1161/01.CIR.92.11.3163
[3] T. Horisaki, T. Yamashita, H. Yokoyama, K. Urasawa
and A. Kitabatake, “Three-Dimensional Reconstruction
of Computed Tomographic Images of Anomalous Origin
of the Left Main Coronary Artery from the Pulmonary
Trunk in an Adult,” American Journ al of Cardiology, Vol.
92, No. 7, 2003, pp. 898-899.
doi:10.1016/S0002-9149(03)00913-5
Copyright © 2013 SciRes. ACT