Low Levels of Complement Factor C4 Not Always Implicate Disease Activity in Systemic Lupus Erythematosus
100
strongly positive (1: >640; IIF on HEP2 cells) as were
anti-dsDNA antibodies (Farr assay; 742 IU/ml).
A diagnosis was made of (idiopathic) active systemic
lupus erythematosus (SLE) and the patient was treated
with 1000 mg methylprednisolone iv followed by oral
prednisone 40 mg a day with a good clinical response
while proteinuria disappeared and CRP levels normalized.
After stopping diclofenac transaminases normalized. After
dismission prednisone was gradually tapered to 5 mg a
day and hydro xyc hl o r oquine 400 m g a day was ad ded .
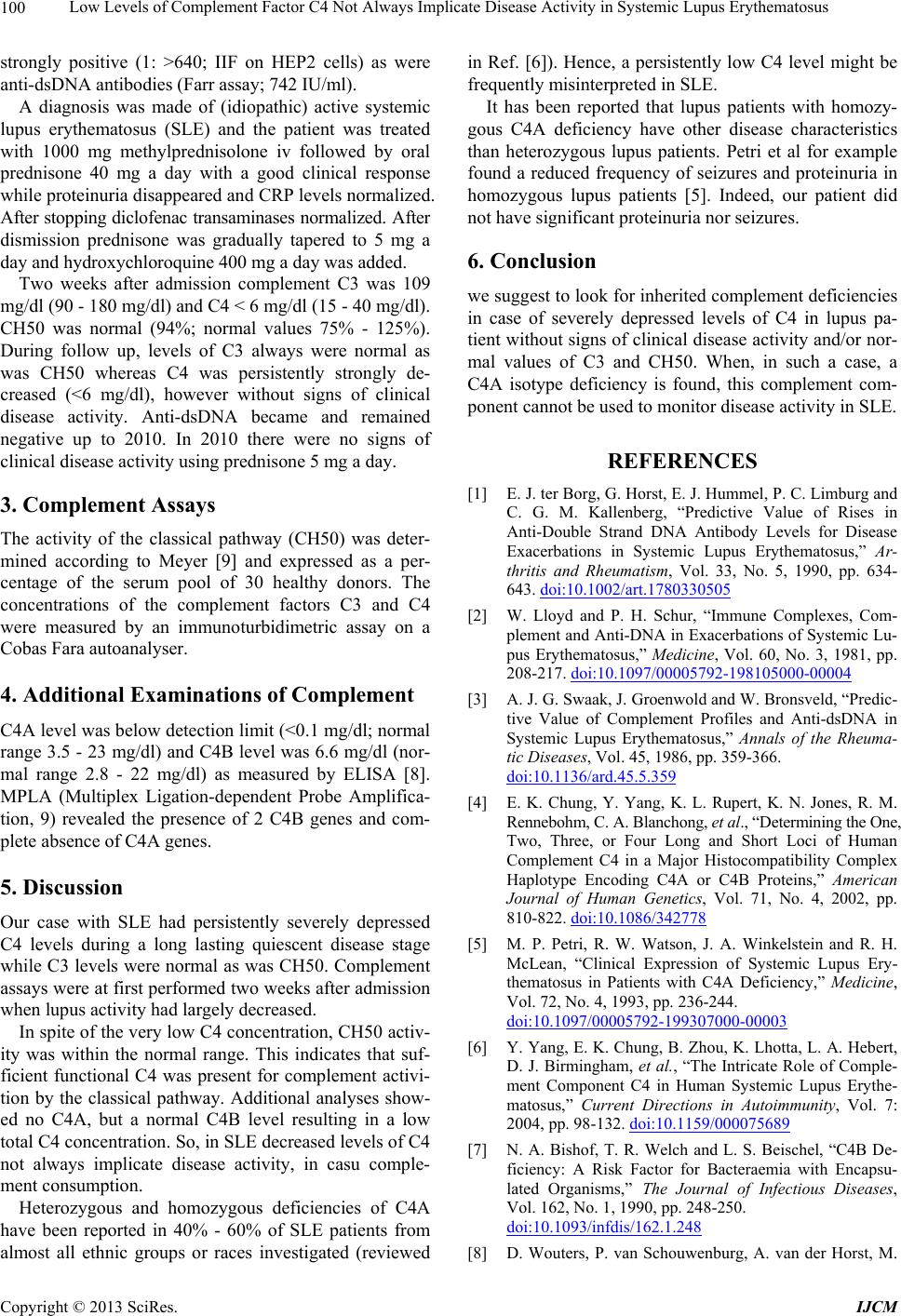
Two weeks after admission complement C3 was 109
mg/dl (90 - 180 mg/dl) and C4 < 6 mg/dl (15 - 40 mg/dl).
CH50 was normal (94%; normal values 75% - 125%).
During follow up, levels of C3 always were normal as
was CH50 whereas C4 was persistently strongly de-
creased (<6 mg/dl), however without signs of clinical
disease activity. Anti-dsDNA became and remained
negative up to 2010. In 2010 there were no signs of
clinical disease activity using prednisone 5 mg a day.
3. Complement Assays
The activity of the classical pathway (CH50) was deter-
mined according to Meyer [9] and expressed as a per-
centage of the serum pool of 30 healthy donors. The
concentrations of the complement factors C3 and C4
were measured by an immunoturbidimetric assay on a
Cobas Fara autoanalyser.
4. Additional Examinations of Complement
C4A level was below detection li mit (<0.1 mg/d l; normal
range 3.5 - 23 mg/dl) and C4B level was 6.6 mg/dl (nor-
mal range 2.8 - 22 mg/dl) as measured by ELISA [8].
MPLA (Multiplex Ligation-dependent Probe Amplifica-
tion, 9) revealed the presence of 2 C4B genes and com-
plete absence of C4A genes.
5. Discussion
Our case with SLE had persistently severely depressed
C4 levels during a long lasting quiescent disease stage
while C3 levels were normal as was CH50. Complement
assays were at first performed two weeks after admission
when lupus activity had largely decreased.
In spite of the very low C4 concentration , CH50 activ-
ity was within the normal range. This indicates that suf-
ficient functional C4 was present for complement activi-
tion by the classical pathway. Additional analyses show-
ed no C4A, but a normal C4B level resulting in a low
total C4 concentration . So , in SLE decreased lev els of C4
not always implicate disease activity, in casu comple-
ment consumption.
Heterozygous and homozygous deficiencies of C4A
have been reported in 40% - 60% of SLE patients from
almost all ethnic groups or races investigated (reviewed
in Ref. [6]). Hence, a persistently low C4 level might be
frequently misinterpreted in SLE.
It has been reported that lupus patients with homozy-
gous C4A deficiency have other disease characteristics
than heterozygous lupus patients. Petri et al for example
found a reduced frequency of seizures and proteinuria in
homozygous lupus patients [5]. Indeed, our patient did
not have significant proteinuria nor seizures.
6. Conclusion
we suggest to look for inherited complement deficiencies
in case of severely depressed levels of C4 in lupus pa-
tient without signs of clinical disease activity and/or nor-
mal values of C3 and CH50. When, in such a case, a
C4A isotype deficiency is found, this complement com-
ponent cannot be used to monitor disease activity in SLE.
REFERENCES
[1] E. J. ter Borg, G. Horst, E. J. Hummel, P. C. Limburg and
C. G. M. Kallenberg, “Predictive Value of Rises in
Anti-Double Strand DNA Antibody Levels for Disease
Exacerbations in Systemic Lupus Erythematosus,” Ar-
thritis and Rheumatism, Vol. 33, No. 5, 1990, pp. 634-
643. doi:10.1002/art.1780330505
[2] W. Lloyd and P. H. Schur, “Immune Complexes, Com-
plement and Anti-DNA in Exacerbations of Systemic Lu-
pus Erythematosus,” Medicine, Vol. 60, No. 3, 1981, pp.
208-217. doi:10.1097/00005792-198105000-00004
[3] A. J. G. Swaak, J. Groenwold and W. Bronsveld, “Predic-
tive Value of Complement Profiles and Anti-dsDNA in
Systemic Lupus Erythematosus,” Annals of the Rheuma-
tic Diseases, Vol. 45, 1986, pp. 359-366.
doi:10.1136/ard.45.5.359
[4] E. K. Chung, Y. Yang, K. L. Rupert, K. N. Jones, R. M.
Rennebohm, C. A. Blanchong, et al., “Determining the One,
Two, Three, or Four Long and Short Loci of Human
Complement C4 in a Major Histocompatibility Complex
Haplotype Encoding C4A or C4B Proteins,” American
Journal of Human Genetics, Vol. 71, No. 4, 2002, pp.
810-822. doi:10.1086/342778
[5] M. P. Petri, R. W. Watson, J. A. Winkelstein and R. H.
McLean, “Clinical Expression of Systemic Lupus Ery-
thematosus in Patients with C4A Deficiency,” Medicine,
Vol. 72, No. 4, 1993, pp. 236-244.
doi:10.1097/00005792-199307000-00003
[6] Y. Yang, E. K. Chung, B. Zhou, K. Lhotta, L. A. Hebert,
D. J. Birmingham, et al., “The Intricate Role of Comple-
ment Component C4 in Human Systemic Lupus Erythe-
matosus,” Current Directions in Autoimmunity, Vol. 7:
2004, pp. 98-132. doi:10.1159/000075689
[7] N. A. Bishof, T. R. Welch and L. S. Beischel, “C4B De-
ficiency: A Risk Factor for Bacteraemia with Encapsu-
lated Organisms,” The Journal of Infectious Diseases,
Vol. 162, No. 1, 1990, pp. 248-250.
doi:10.1093/infdis/162.1.248
[8] D. Wouters, P. van Schouwenburg, A. van der Horst, M.
Copyright © 2013 SciRes. IJCM