C. M. Moore et al. / Open Journal of Gastroenterology 3 (2013) 1-4 3
Table 2. Calculated portal vein pressures (mmHg).
Pre-TIPS Post-TIPS Normal value
Hepatic vein 19 20 <5
Wedged portal vein 32 27 5 - 10
Gradient 13 7 0 - 5
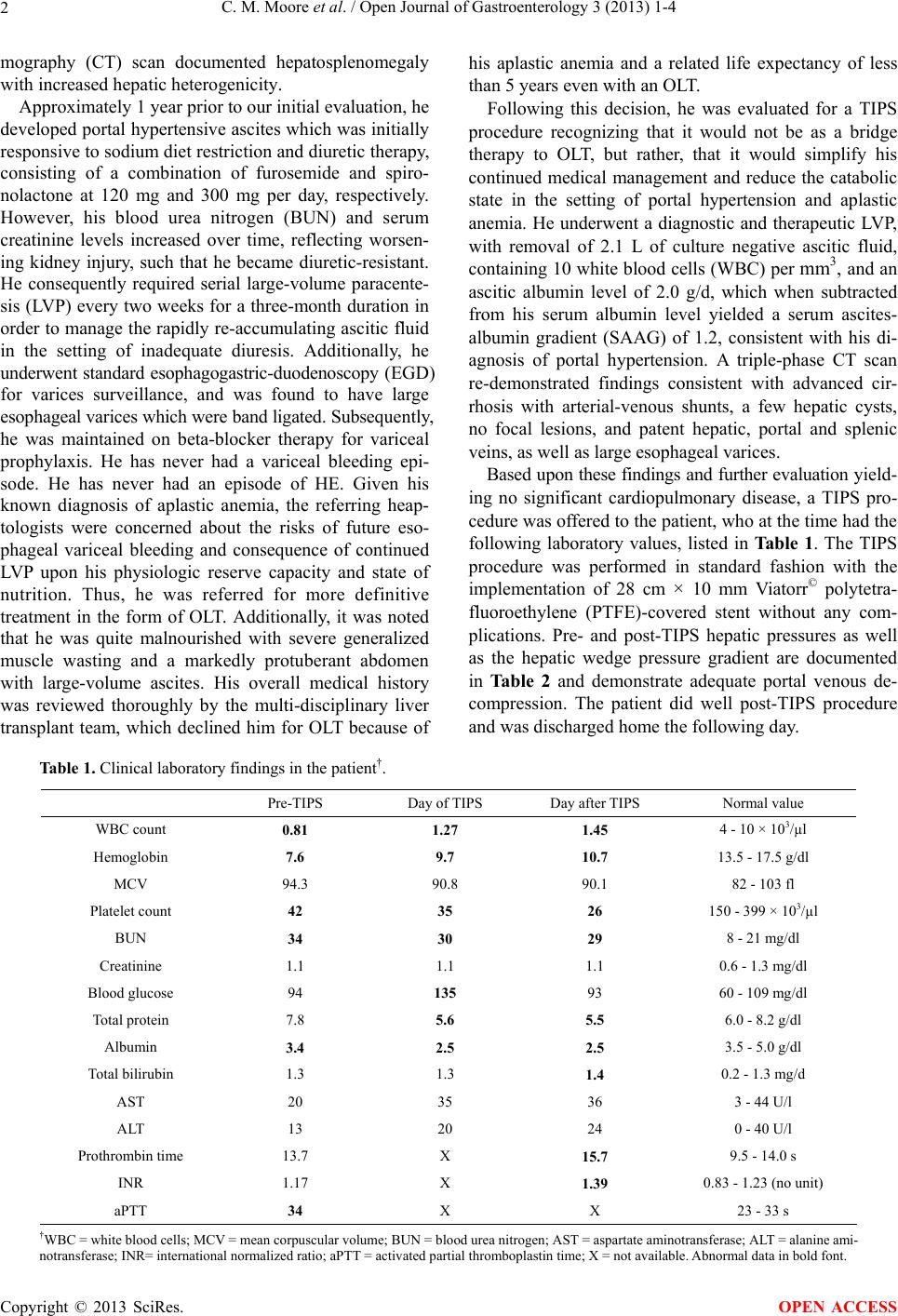
At a follow-up outpatient visit two weeks later, an ab-
dominal ultrasound (US) with a complete duplex Dop-
pler study was performed and documented peak systolic
velocities at the portal vein end of the TIPS, mid TIPS,
and hepatic vein end of the TIPS of 57, 163 and 119
cm/sec with no high velocity jets, respectively. In the
following weeks, the patient’s ascites resolved, and his
diuretic requirements were reduced to 20 mg furosemide
and 50 mg spironolactone per day in the setting of stable
kidney disease and an adequate diuresis. In the post-TIPS
state, he no longer required paracentesis, his esophageal
varices were decompressed, his nutritional state and
overall clinical appearance improved. Most importantly,
he did not develop any complications of his TIPS proce-
dure and survived an additional 2.5 years at which time
he died as a result of severe leucopenic sepsis.
3. DISCUSSION
Cirrhosis is manifested by an extensive fibronodular re-
placement of the liver parenchyma with resultant portal
hypertension and progressive synthetic dysfunction [4].
The development of portal hypertension leads to a num-
ber of complications including HE, ascites and variceal
bleeding, which are each associated with an increased
morbidity and mortality rate [2-5]. Ascites is treated with
a combination of dietary sodium restriction and diuretics,
primarily consisting of furosemide and spironolactone. In
approximately 10% of ascites patients, a diagnosis of
refractory ascites develops wherein they no longer re-
spond to or cannot tolerate these diuretic therapies. In
such cases, LVP is instituted, and while efficacious, is
associated with complications consisting of peritoneal
bleeding, infection, and increased catabolic rate. Fur-
thermore, there are ongoing concerns of long-term cost
and quality-of-life issues [2,3,6].
It is within this setting that the theory and implementa-
tion of TIPS arose. TIPS provides a non-surgical method
of delivering blood from the portal to hepatic venous
system through the utilization of a transhepatic bypass
stent [3]. It is generally accepted that a TIPS procedure is
utilized best in patients having been classified as CTP
class A patient or with a MELD score < 14 who is await-
ing OLT, and who has experienced a number of portal
hypertensive complications consisting of refractory as-
cites or variceal bleeding. Other indications for a TIPS
include the development of a hepato-hydrothorax, al-
though experience with this problem is less-well docu-
mented [3-5]. Furthermore, given the expected physiol-
ogic effect of TIPS a number of contra-indications to its
implementation have been identified such as congestive
heart failure and severe pulmonary hypertension. While
TIPS has been successful in ameliorating the complica-
tions of portal hypertension, its long-term effectiveness,
effect on quality-of-life, and health-care cost have also
been matters of debate when compared to serial LVP [2,3,
6]. In part, some of these issues revolv e around the stud-
ies of uncovered TIPS stent compared to LVP, whereas in
the current period covered TIPS stents, which are less
likely to become occluded, are the standard-of-care [7].
In this case report, the patient had several common
portal hypertensive sequelae of his PBC, including eso-
phageal varices and refractory ascites. Furthermore, the
ascites required serial LVP, which despite being a fairly
common procedure, is nevertheless associated with com-
plications and costs that are substantial over time. Worse
still is the patient’s underlying aplastic anemia, a d isease
process itself manifested by pancytopenia including
symptomatic anemia, hemorrhage, and a risk of infection.
In addition, there is also an increased risk for the devel-
opment of hematologic cancer [8]. It was this underlying
disease process and its associated morbidity and mortal-
ity that both excluded the patient from OLT considera-
tion and made continued LVP a prohibitive option given
the well-recognized probability of complications over
time.
Given these facts, the present case report is interesting
for several reasons. Firstly, it is as best as we can deter-
mine the only case in which a TIPS procedure has been
performed in a cirrhotic individual with underlying apla s-
tic anemia. Importantly, the TIPS procedure was suc-
cessful in reducing his ascites and the need for repetitive
LVP as well as decompressing his esophageal varices.
Importantly, no complications were experienced in the
procedure or experienced in his post-procedural follow-
up. Moreover, he was able to reduce his diuretic re-
quirements and reduce his catabolic state. The benefits to
his esophageal varices were important, as any future
bleeding episodes would be complicated not only by his
baseline anemia and thrombocytopenia, but also in the
difficulty of finding an appropriate blood match given
the number of anti-platelet antibodies he had developed
over the preceding years of transfusion.
As he no longer required LVP, his nutrition status, as
assessed by physical appearance improved. LVP results
in significant ascitic fluid protein losses when compared
to diuretic therapy [9]. Additionally, in the post-TIPS
setting in the absence of ascites there is an associated
increased mobility, energy and protein intake compared
to continued LVP [10]. Post-TIPS, his quality-of-life im-
proved, a general finding well-documented in the litera-
Copyright © 2013 SciRes. OPEN ACCESS