Paper Menu >>
Journal Menu >>
 Vol.2, No.9, 1120-1133 (2010) Health doi:10.4236/health.2010.29165 Copyright © 2010 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ The need for a new framework for the economic evaluation of health services in a national health scheme Jeff R. Richardson*, John McKie, Kompal Sinha Centre for Health Economics, Monash University, Melbourne, Australia; *Corresponding Author: Jeff.richardson@buseco.monash.edu.au Received 29 April 2010; revised 20 May 2010; accepted 25 May 2010. ABSTRACT The normative theory of economic evaluation and its welfare theoretic basis are deeply prob- lematical and result in recommendations which are potentially unfair. The root cause of the problem is the set of assumptions behind the theory which posit behaviours and motivations that are not universal, and which exclude other behaviours and motivations that are potentially important. As falsification of assumptions may be evaded indefinitely this paper presents an alternative critique. We commence with six an- omalies with the theory which are attributable to the assumptions. The first three—the net pre- sent value criterion, the willingness to pay cri- terion and moral hazard—arise from welfare theory. The remaining three are associated with the present definition of cost, the concept of efficiency and the omission of sharing, which are common to most economic evaluation. We argue that these anomalies are indicative of a defective core theory and that they are equiva- lent to observations that conflict with a positive theory. In the final section we outline and illus- trate a more general framework for decision making that is capable of overcoming the ano- malies we discuss. Keywords: Economic Evaluation; Economic Costs; Welfare Theory; Empirical Ethics; Cost Benefit Analysis 1. INTRODUCTION Between 1990 and 2003 public expenditures on health per capita in the OECD doubled. Unsurprisingly this has resulted in closer scrutiny of the services provided. Commencing with Australia in January, 1993, an in- creasing number of countries have passed legislation to ensure the economic evaluation of pharmaceuticals be- fore receiving subsidy. Economic evaluation is also in- creasingly adopted for other public health services, a trend which is likely to be of increasing importance in rationing health services, even in the USA where current legislation prevents its full use in Medicare. Given this scenario, the relatively low level of self- criticism of fundamental elements of the theory of eco- nomic evaluation is of concern. In the financial sector the recent world-wide crash signalled the existence of defects in both practice and theory. The doubtful activi- ties of many financial managers are now well known. Less publicised is that in the 1960s Mandelbrot demon- strated that a fundamental tenet of financial theory was wrong [1]: movements in the stock exchange follow a power function and deviations are not normally distrib- uted. Sometime earlier, Keynes had argued that the re- turn on assets was often subject to uncertainty, not risk (i.e., there is not enough information to justify assuming a particular distribution of expected returns) [2]. Both observations strike at the basis of the theory which un- derpinned the financial structures of recent times, but both have been largely ignored. The recent crash will, hopefully, provoke introspection and error learning. In contrast, there are no external events that could en- courage examination of the theory and practice of eco- nomic evaluation. However, there are anomalies in its use in the health sector and elsewhere which are at least as important as and much more obvious than those iden- tified by Mandelbrot and Keynes. Some of these are out- lined in Section 2 below. Those relating to the health sector are largely associated with the neglect of fairness and the drive to find technical answers to questions re- lating to social values. The proximate reasons for this outcome are discussed in Section 3. To increase analytical rigour, assumptions have been made in economic theory that oversimplify or seriously distort reality (cf. risk versus uncertainty).  J. R. Richardson et al. / HEALTH 2 (2010) 1120-1133 Copyright © 2010 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ 1121 Equally damaging is the application of the standard “ce- teris paribus”—all else equal—caveat. Especially in the health sector, conclusions are often context-specific and neglect of some elements may be as damaging as the misrepresentation of others. Finally, in Section 4 we out- line and illustrate some principles for the construction of a better framework for economic evaluation. The existing framework is broadly concerned with the comparison of benefits and opportunity costs where the latter are the benefits foregone by using resources in one way rather than another. A key criterion in evaluation theory is that the present value of benefits exceeds cost (B > C), or that net present value is positive (B – C > 0). A necessary condition for this is that the benefit-to-cost ratio exceeds unity (B/C > 1), or the cost per unit of benefit is less than unity (C/B < 1). This criterion defines efficiency. If there is a constraint, such as a fixed budget, then ‘unity’ is replaced by a threshold reflecting the op- portunity cost of capital or use of the constrained re- source. In the health sector, however, there is tension about the application of this broad principle. In more orthodox ‘welfare theory’ (WT) benefits are equated with indi- vidual ‘utility’ where this, in turn, is equated with the strength of a person’s preferences. While it is argued (following Robbins [3]) that these subjective preferences cannot be directly compared, they can be revealed by a person’s willingness to pay [4], and social welfare—the welfare of society—is a function only of individual utili- ties: the doctrine of “welfarism”. The more orthodox arm of health economics attempts to implement these princi- ples. For example, the gold standard for benefit meas- urement is revealed preferences, but in its absence the second best approach is to use stated preferences and/or stated willingness to pay. This includes the willingness to pay for life itself, or at least a ‘statistical life’, which is often inferred from an individual’s willingness to pay for a reduction in the risk of death or the willingness to ac- cept compensation for assuming a risk of death [5,6]. In contrast, in Cost-Effectiveness Analysis (CEA) benefits are “external” and measured in physical terms, either as lives saved, life years or “quality-adjusted life years” (QALYs). The term “extra welfarism” has been used to describe the theory that the only—or only rele- vant—benefit which needs inclusion in CEA in the health sector is health outcome [7]. While this ‘external benefit’ or ‘material welfare’ tradition is the earlier his- torically, welfare theory and welfarism are widely re- garded as a gold standard with various attempts being made to either reconcile CEA with them or to show the special circumstances when CEA provides a consistent ‘theoretically correct’ solution to economic problems [8]. Some of the anomalies with the theory of economic evaluation are unique to welfare theory. However, there are anomalies which it shares with extra-welfarism based CEA. 2. SOME ANOMALIES 2.1. Net Present Value: The Wrong Criterion Welfare theory evolved from the context of the private sector in which individuals chose whether or not to pur- chase a commodity for their own benefit. Unsurprisingly, it is assumed in WT that well-informed and rational in- dividuals will apply the criterion that (personal) benefits should equal or exceed (personal) costs—the positive net present value criterion. If costs equal benefits plus $1 there will be, or should be, no transaction. This theoreti- cal point has been transferred to the health sector: if total costs as described by WT exceed total benefits as de- scribed by WT no service should be provided even if the patient dies. Welfare theory allows for compassionate externalities—others may obtain utility if the patient lives, but if not, then the patient should die as greater utility can be gained if the resources are used elsewhere. However, changing the context from a private market to a national health service (NHS) may have profound consequences for almost all aspects of evaluation in- cluding the comparison of costs and benefits. At present, the bulk of health costs are borne by ‘society’ (in the form of tax or premium payments) and benefits are ob- tained by an individual who will not bear (at least the full) cost. Different principles almost certainly apply to the willingness to provide benefits, or else the NHS would have been unnecessary and if the scheme is suc- cessful then the demands upon the national health sys- tem will differ from the demands upon the private sys- tem. With full knowledge of the magnitude of the utili- ties involved those making decisions for society may elect to save life, or improve life, when it is ‘uneco- nomic’ according to WT. There are well known ethical and rational reasons for this, including those appealing to ‘sympathy’, ‘reciprocal altruism’, and ‘process utility’ (fairness). More significantly, there may be ‘counter- preferential’ reasons, based on ‘duty’ or ‘commitment’. A well-known argument against duty and commitment, to which we return below, is that they may simply be another source of utility: they are only superficially ‘counter-preferential’. More fully, since utility is re- vealed by decisions, the decision to carry out one’s duty indicates that the decision maker must have received utility. However, while the revealed preference criterion is potentially useful in a context where an individual is well-informed and known to be only self interested, this interpretation of the revealed preference definition of  J. R. Richardson et al. / HEALTH 2 (2010) 1120-1133 Copyright © 2010 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ 1122 utility converts the argument into a tautology: all action, by definition, reflects utility. Some people may, indeed, gain utility from fulfilling their duties, but as Sen has pointed out [9], other motivations are clearly possible. 2.2. Willingness to Pay: An Unwanted Element Private willingness to pay (WTP) is still widely used and vigorously promoted in the literature as a method for evaluating improvements in quality of life (QoL), and the value of life itself [6,10]. However, the wedge be- tween recipients and funders of health services invali- dates the logical connection between social goals and private WTP and makes the interpretation of WTP data problematical. As noted, if there was no difference be- tween an individual’s WTP for a service for themself and the WTP of the society, then it is unlikely that there would be significant support for an NHS. Private, risk- based insurance would probably satisfy the need for en- suring health. But the great appeal of an NHS is that it promotes fair access to health services. That is, the ap- peal relates to the use, or potential use, of services spe- cifically by those who would not otherwise have access through lack of financial resources. Restated, the pur- pose of an NHS is to ensure that services are available to people when their private WTP is less than the cost. That is, the purpose of an NHS is to ensure that the ‘optimal outcome’ described by welfare theory does not occur. Adopting the WTP criterion of benefit results in a fur- ther paradox for the orthodox economist attempting to achieve economic efficiency. For every additional dollar that an individual is willing to spend on themself, the NHS should also be willing to spend an additional dollar on this person. With WTP benefits determined by in- come, taxpayers would have to subsidise the wealthy, who are willing to pay more for their own health care, and spend less on the poor, who are the usual target group. A final defence of the WTP criterion is more ad hoc. Since economists have not devised a better method for determining the dollar value of health services, the WTP may indicate the order of magnitude of appropriate spending in the health sector. Some have adjusted the WTP to take account of an individual’s wealth, but this remains an ad hoc approach as it does not overcome the theoretical problems outlined above [11,12]. The ad hoc solution may, indeed, be the best available, but it has the theoretical status of an opinion poll and should not claim greater authority. 2.3. Moral Hazard: Replacing Normative with Technical Objectives Disagreement exists about the benefits of health insur- ance and at least part of this has arisen because of the different lenses through which the protagonists have viewed the issue. Following Pauly [13], economists have almost universally accepted that health insurance is sub- ject to ‘moral hazard’. That is, it causes an ‘excess bur- den’—an inefficient use of resources, where the benefit (determined by willingness to pay, or the area under the demand curve) is less than cost. This arises because the price to the patient has been reduced (by the insurance rebate) to be less than the cost (possibly zero in a ‘free’ scheme). Patients are therefore willing to pay the re- duced (or zero) cost of additional care for which society pays the full cost. It is usually concluded that insurance therefore induces the use of resources where costs ex- ceed benefits and that this inefficiency should be limited by the use of patient co-payments to reduce the “excess burden”. The argument appears, prima facie, a good example of value free social science. However, social welfare groups and supporters of universal health insurance tend to have a different focus. The demand curve used in the economist’s argument is a simplification. There are, in fact, many demand curves determined primarily by lev- els of illness and ability to pay. The demand of the wealthiest will be relatively unresponsive to prices, with responsiveness, or ‘elasticity’, increasing as family in- come falls and price becomes a larger real burden. As the patient co-payment rises (to reduce the excess burden) the reduction in health care will be determined very largely by income. The savings to a tax-financed NHS will primarily benefit wealthy taxpayers. In the extreme, the ‘excess burden’ may be interpreted not as a measure of pure inefficiency, but as a measure of the extent of the redistribution of income from the wealthy and healthy to the poor and unhealthy, and it is to the former group that there is an “excess burden”. In Australia, at least, co- payments have been supported for reasons of sectional interest by doctors (to give some control over incomes), by government (to shift costs to patients) and by social welfare groups (to protect the poor). Economists alone have perceived co-payments to be primarily related to efficiency. The literature on moral hazard is an example of the consequences of the previous error of treating the net present value (NPV) as a gold standard criterion. Be- cause behaviour changes as a result of an NHS the de- viation from the (NPV) criterion is considered to be a source of inefficiency, and to be avoided, even if from a social perspective this deviation was the purpose of the scheme. Of less relevance here, the moral hazard anomaly also applies in a private market with an additional error caused by an omission from the theory, namely utility obtained in  J. R. Richardson et al. / HEALTH 2 (2010) 1120-1133 Copyright © 2010 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ 1123 the “pre outcome” period before a person knows whether or not they will be sick [14]. The disutility of risk induces the purchase of insurance in the knowledge and with the purpose of altering realised spending in the case of illness. The moral hazard argument defines this deviation as inef- ficiency reflecting the analytical weakness of orthodox economics’ treatment of time. 2.4. Economic Costs: The Wrong Comparator The problems outlined above arise in cost-benefit analy- sis (CBA) where both benefits and costs are reduced to dollars. In practice, the predominant form of economic evaluation in the health sector is cost-effectiveness analysis, or cost minimisation analysis, which seeks to rank services according to their cost-per-unit of benefit (lives, life years, or quality adjusted life years in the case of cost-utility analysis). Cost-effectiveness analysis can be justified independently of welfare theory as it indi- cates how benefits, somehow measured, may be maxi- mised given resources or from a given budget. Benefits need not be measured by individual utility. Nevertheless it encounters problems which also apply to CBA. A simple extension of the earlier arguments indicates that the ‘costs’ that are relevant in evaluation studies may not be the resource costs of economic theory, i.e. the value of the resources expended (labour, time, capital, stock depleted, etc). The ‘social willingness to pay’ - the amount an individual is willing to contribute to an NHS (or the willingness of the individual’s “agents” on their behalf)—depends upon their “social generosity”. This may or may not be closely related to an individual’s perception of their personal benefits from the NHS. Of greater relevance here, it will not depend upon net use of resources but upon the amount of money lost personally through the taxes and premiums that finance the NHS. These are not the same. The net resource cost of a medi- cal service is equal to the direct cost minus indirect benefits, where the latter is the value of employment gained (or not lost) by a patient’s return to the workforce. But the chief beneficiary of this is the employer or pa- tient not the taxpayer. Consequently, an increase in taxes or premiums which resulted in increased employment and in ‘negative real costs’ would still impose a personal cost on the taxpayer. If willingness to pay and cost are to be equated to achieve the usual notion of efficiency, it is this personal cost to the taxpayer, not the net resource cost, which should be compared with the social willing- ness to pay. The argument is even clearer if the scope of govern- ment services is broadened to include pensions. In prin- ciple every person with a chronic illness could be of- fered a compensatory pension in exchange for their ac- cess to the NHS. As normally understood, pensions are a “transfer” (from the taxpayer to the recipient) and omit- ted from the calculation of “costs” as no real resources are consumed. Consequently, the compensatory pension would generate similar satisfaction but no real cost. It would always be the better strategy. But the strategy would impose a (possibly much higher) personal cost on taxpayers and the optimal strategy could not avoid tak- ing this into account. 2.5. Equity and Efficiency: A Misleading Distinction To a greater or lesser extent every country endorses eq- uity of access to needed services (somehow defined). But the cost of providing needed services varies. Patients in inaccessible locations are more costly to treat than those close to major hospitals and medical facilities. Even a partial concession to equity therefore implies the provision of services with higher costs per unit of benefit than might be provided to patients in large cities. Mini- mising cost or cost-per-unit of benefit will not, therefore, achieve social goals efficiently. Stated simply, when there are two objectives—cost and equity—social goals cannot be achieved by focusing only upon one of these. In principle this is acknowledged and formalised in textbooks by recognising the existence of an equity- efficiency trade-off. In practice the evidence reveals lit- tle concern with equity, with most studies providing no evidence relevant for its assessment. By contrast, attention has been given to what is easily measured, while the various elements of fairness and its inclusion in empirical studies have been neglected [15]. The somewhat emasculated concept of fairness—“equity” —has been largely consigned to the realm of theory. But even the concept of an equity-efficiency trade-off is un- satisfactory. This may be seen by considering a well- defined category of patients, viz, those with a ‘difficult disease’, where costs are high and the effectiveness of treatment is low because of the type of disease and cur- rent state of medical technology. There is no obvious logical or ethical reason why the principle of equal ac- cess for equal need should allow an increased cost threshold because of, say, a person’s geographical loca- tion, but no similar increase because of a person’s medi- cal problems. To the contrary, those who live in remote locations do so voluntarily. Those contracting difficult diseases generally do so through bad luck. From behind a veil of ignorance we would therefore expect to give higher priority to the latter, not former group. Of course, not all treatments can be provided irrespective of cost. But just as those who have been historically singled out  J. R. Richardson et al. / HEALTH 2 (2010) 1120-1133 Copyright © 2010 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ 1124 as beneficiaries in the equity-efficiency trade-off (e.g. rural patients) receive some (incomplete) compensation, so it might be expected that those with difficult diseases would similarly receive some consideration possibly at the expense of those with “lucky” illnesses. In practice this commonly occurs. Few are left to suffer in a severe condition because all of the options are cost-ineffective: those with only days to live are accommodated in a high-cost hospital minimally receiving palliative care which is highly “cost-ineffective” as judged by the crite- rion of cost-per-life year gained or cost-per-quality ad- justed life year gained. However economic theory has not caught up with practice. The efficiency goal of minimising the cost of achiev- ing objectives becomes problematical, as one of the ob- jectives is—all else equal—the (part) provision of ser- vices to those with inefficient-to-treat diseases. The concept of a trade-off between cost/QALY (efficiency) and cost/QALY (fairness) therefore becomes, at best, ambiguous. 2.6. Sharing: Ignored Social Objectives Perhaps the greatest anomaly with economic evaluation theory is the theoretical framework itself. The frame- work is based upon an analysis of the individual and the way each individual maximises their utility or wellbeing. Prima facie, however, this is almost the opposite of the perspective embodied in the rhetoric of an NHS. The latter social perspective relies heavily upon the concepts of “community”, “solidarity”, “sharing” and emphasises the need to off-set the barriers to uneven access caused by price and income inequalities—which are precisely the variables that drive the allocation of resources and define benefits in the orthodox economic model. Indeed, while in theory the vocabulary of the entire English lan- guage is available to economists, in practice orthodox welfare economists rarely speak about “community”, “sharing”, “duty” etc. This can have damaging conse- quences, as described by George Orwell [16] in an ap- pendix to his classic novel on tyranny, “Nineteen Eighty- Four”. He observes that in the absence of appropriate vocabulary the conceptualisation of ideas becomes very difficult1. It is arguable that this has happened in ortho- dox welfare economics in which these important con- cepts play no role. (For exceptions see the advocacy of communitarianism, in particular, by Mooney [17,18], sympathy and justice by Sen (2009), also discussions of “sharing”, “fairness”, “altruism” and “trust” in the ex- perimental economics literature [19-22]. This truncation of the available language is, in fact, facilitated by the core definitions of welfare theory. Us- ing Samuelson’s revealed preference criterion, it might be argued that if any action, including voting, was ob- served because of any possible motive, then this would indicate that individuals were obtaining utility from that motive, otherwise they would not have done it. There- fore, the reason for self-sacrifice is that it maximises utility. In the extreme case of one person giving their life for another, this must be construed as utility maximising. However, the logic is vacuous. As illustrated in Figure 1, the answer to the question “why does an individual take a particular action”, is that “this action maximises util- ity”. But the answer to the question “how do we know that this action maximises utility”, is that ‘they have taken the action’. The more defensible argument offered by orthodox economics is that its framework includes “externalities” —the utility which people obtain from something exter- nal to the market. There is a long and detailed literature demonstrating how, in theory, “fairness”, “reciprocity”, “participation”, and so on, understood as externalities, can be employed to “shoehorn” the elements of a com- munitarian framework into an orthodox framework (see particularly the works of Culyer [7,23]. In practice this theory is never operationalised. Rarely are measure- ments of the benefit of this type of externality included in economic evaluations. Rather, it has been used to jus- tify the retention of the narrow focus of current practice. Behaviour Obser ved Motivation Utility Maximisation Evidence Figure 1. Revealed preferences and the resur- rected primacy of utility. 1In ‘1984’ the control of thought was achieved by the truncation o f language ‘It was intended that when Newspeak had been adopted once and for all ... heretical thought ... should b e literally unthinkable, at least so far as it is dependent upon words. This was done ... chiefly by elimi- nating undesirable words ... countless other words such as honour, j ustice, morality, internationalism, democracy, science and religion had simply ceased to exist. A few blanket words covered them, and in cov- ering them, abolished them. What was required in a party member was an outlook similar to that of the ancient Hebrew who knew, without knowing much else, that all nations other than his own worshiped “false gods” ... he knew Jehovah and the commandments of Jehovah; he knew, therefore, that all gods, with other names or other attributes were “false gods”.’ [16] pp. 317-319.  J. R. Richardson et al. / HEALTH 2 (2010) 1120-1133 Copyright © 2010 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ 1125 The defensive logic of the argument is effectively that other motivations may (possibly) be attributable to (self- ish) externalities and other, non-selfish motives may (possibly) not exist. Alternatively, if they exist, that they are of no interest to economics. Therefore we may treat them as if they do not exist or are irrelevant. External- ities are a satisfactory explanation for altruism and commitment; orthodox theory and therefore current practices are justified. However, there is strong evidence that people have additional motivations to selfish utility maximisation and that these can be behaviourally significant. Bein- hocker [24] for example, summarises a large body of evidence obtained from experiments and anthropology which indicates that human beings are conditional co- operators and altruistic punishers, behaviour some- times described as “strong reciprocity”. This results in a predisposition to cooperate with others and punish (even at personal cost if necessary) those who violate the norms of cooperation, even when it is implausible to expect these costs to be recovered at a later date [25]. One of the most widely replicated experiments de- monstrating strong reciprocity is the so-called ultima- tum game. Using real money, one individual divides the money between themselves and a second person who has the ability to either accept the money or reject the offer. In the latter case neither person receives any money. The utility maximising strategy for the second person is to accept what they are offered, however small it is. However, the universal observation is that the second person will reject the offer if it is too small, in order to punish the first person. In countries as var- ied as the USA, Mongolia and Zimbabwe it has been found that most individuals divide the money more or less equally and that the second person will reject the offer when it is less than about 30 per cent of the total [24]. One group of respondents has been found to be- have in the way predicted by economic theory, namely those who have a disorder related to autism in which they have little capacity to empathise with others [26]. Alternatively, people could derive from such behaviour benefits that go beyond the monetary payoff - e.g. the ‘warm glow’ that derives from sharing, defending jus- tice, etc. [27,28]. The prevalence and importance of motivations apart from utility maximisation are apparent in the results from two research projects undertaken at the Centre for Health Economics at Monash University. In the first, 501 Australians were asked to indicate their agreement or disagreement with a series of statements relating, inter alia, to their motivation. Results reported in Table 1 indicate that the majority of respondents care about relative and not just absolute income levels (Question 1) and an even larger number rejected the view that the maximisation of happiness is the most important ethical principle (Question 2). An overwhelming majority re- jected the view that they, personally, fulfilled their duty to achieve happiness (Question 3,4) and less than 1 in 5 believe that other people help one another only if they gain something personally (Question 5). This is not conclusive however. For example, 84.2 per cent of re- spondents also agreed with the statement: “I fulfil my duties to individuals and organisations (to family, country etc) because doing so will make me happier in the long run”. This suggests that motivations may not be clearly separated in people’s minds. People may fulfil their duties out of genuine self-sacrifice (which conflicts with utility maximisation as a psychological hypothesis) or it may be because it will enhance their own well-being, or both. The second study was web based. Individuals were asked to allocate a block of money to one of four pa- tients, each of whom would die without treatment. Pa- tients were identical except for the cost of treating their disease, which led to a different outcome. One block of money could produce 12, 8, 6 or 4 additional years of life. After allocating the first block of money respon- dents were asked to allocate a second, third and fourth block, etc, to any of the patients. This left respondents with a choice of allocating resources where they pro- Table 1. Results from the monash ethics survey. Questions/Statements % (Strongly) agree% Neutral % (Strongly) disagree 1. Australia is better off if the wealthy receive even higher incomes so long as the income of the poor does not fall. 22.8 22.8 57.4 2. Maximising happiness is more important than any other ethical principle. 14.3 19.8 65.9 3. I have some duties that I must fulfil even if doing so makes me a little less happy. 91.5 4.7 3.9 3. I fulfil my duties to individuals and organisations (to family, country etc) not primarily because it will make me or others happy, but because it is my role (e.g. as a mother, father, employee etc). 77.8 5.6 16.7 4. People help others only because they gain something personally. 18.2 21.2 60.7 Source: [44] 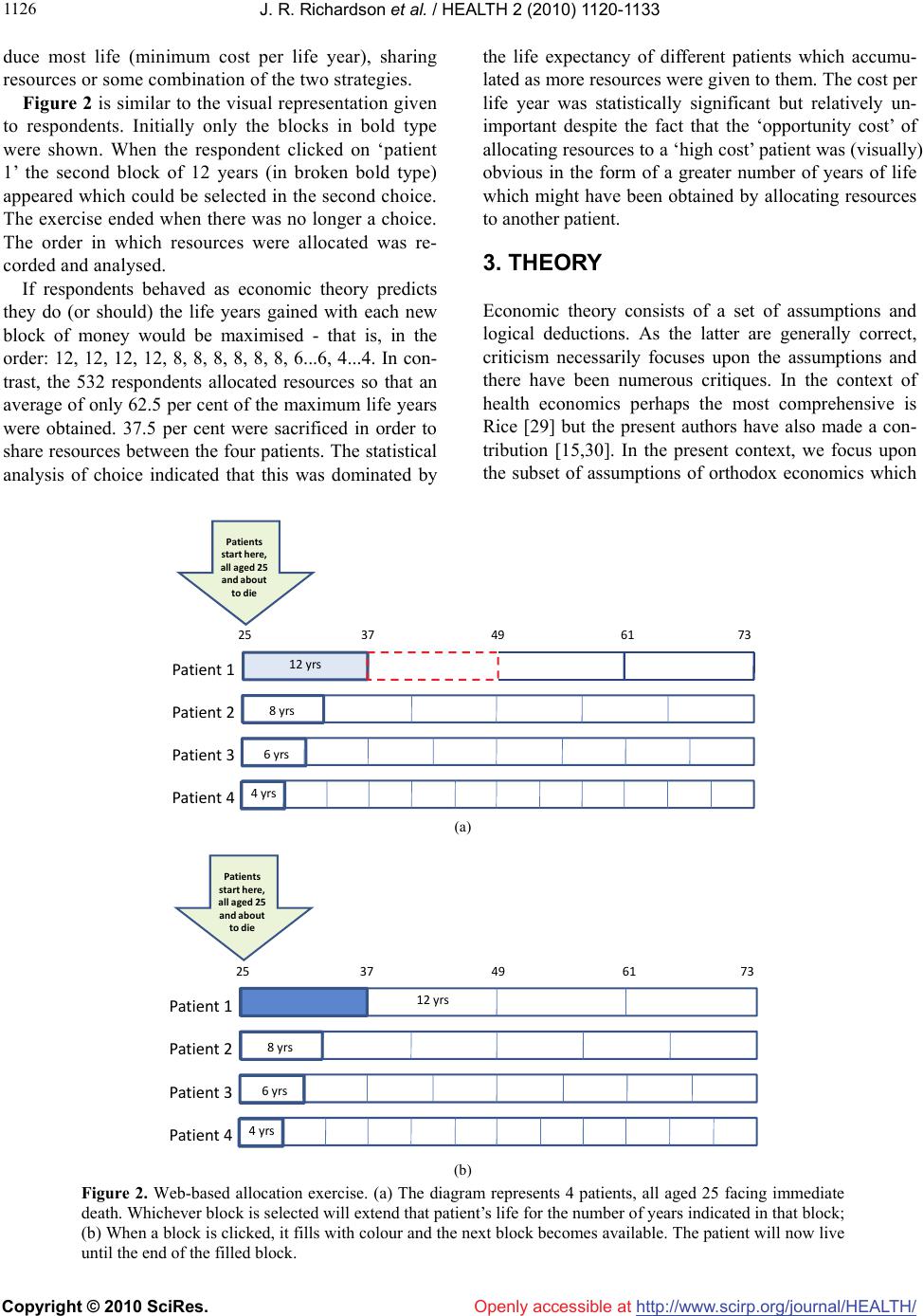 J. R. Richardson et al. / HEALTH 2 (2010) 1120-1133 Copyright © 2010 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ 1126 duce most life (minimum cost per life year), sharing resources or some combination of the two strategies. Figure 2 is similar to the visual representation given to respondents. Initially only the blocks in bold type were shown. When the respondent clicked on ‘patient 1’ the second block of 12 years (in broken bold type) appeared which could be selected in the second choice. The exercise ended when there was no longer a choice. The order in which resources were allocated was re- corded and analysed. If respondents behaved as economic theory predicts they do (or should) the life years gained with each new block of money would be maximised - that is, in the order: 12, 12, 12, 12, 8, 8, 8, 8, 8, 8, 6...6, 4...4. In con- trast, the 532 respondents allocated resources so that an average of only 62.5 per cent of the maximum life years were obtained. 37.5 per cent were sacrificed in order to share resources between the four patients. The statistical analysis of choice indicated that this was dominated by the life expectancy of different patients which accumu- lated as more resources were given to them. The cost per life year was statistically significant but relatively un- important despite the fact that the ‘opportunity cost’ of allocating resources to a ‘high cost’ patient was (visually) obvious in the form of a greater number of years of life which might have been obtained by allocating resources to another patient. 3. THEORY Economic theory consists of a set of assumptions and logical deductions. As the latter are generally correct, criticism necessarily focuses upon the assumptions and there have been numerous critiques. In the context of health economics perhaps the most comprehensive is Rice [29] but the present authors have also made a con- tribution [15,30]. In the present context, we focus upon the subset of assumptions of orthodox economics which Pat i e n t 1 Pat i e n t 2 Pat i e n t 3 Pat i e n t 4 25374961 73 12yrs 8yrs 6yrs Patients starthere, allaged25 andabout todie 4yrs (a) Pat i e nt 1 Pat i e nt 2 Pat i e nt 3 Pat i e nt 4 2537496173 12yrs 8yrs 6yrs Patients starthere, allaged25 andabout todie 4yrs (b) Figure 2. Web-based allocation exercise. (a) The diagram represents 4 patients, all aged 25 facing immediate death. Whichever block is selected will extend that patient’s life for the number of years indicated in that block; (b) When a block is clicked, it fills with colour and the next block becomes available. The patient will now live until the end of the filled block.  J. R. Richardson et al. / HEALTH 2 (2010) 1120-1133 Copyright © 2010 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ 1127 facilitate the normative conclusions of economic evalua- tion theory, namely that in an NHS services should be offered ideally when their net present value is positive and, when budgets are constrained, according to the ratio of costs to benefits as these terms are defined. Using Sen’s terminology, the most fundamental as- sumptions behind welfarism economics are these: A.1 Individuals are motivated only by utility which they seek to maximise; A.2 Utility is only derived from the consequences of actions (consequentialism); and; A.3 Social welfare—the wellbeing of society—is a function of (only) individual utility; However, these assumptions are insufficient to allow applied evaluation studies and, in practice, some ancil- lary assumptions are also made. These are that; A.4 If one person’s utility is increased without a re- duction in the utility of anyone else—a ‘Pareto im- provement’ - then society may be presumed to be better off; A.5 People are ‘rational’ and well-informed implying that their choices reveal their utility maximising strate- gies; A.6 A net increase in utility increases social welfare, even if there are winners and losers, provided it is theo- retically possible for the former to fully compensate the latter; The final assumption—the potential compensation or Kaldor-Hicks criterion—permits each dollar to be treated as of equal value since it may be redistributed and dol- lars may therefore be added to obtain potential benefits and costs; To a greater or lesser extent each of these assumptions is necessary to justify the practice of cost benefit analy- sis (CBA) as shown in Box 1. If a willingness to pay (WTP) methodology is used to reduce benefits to dollars (the defining characteristic of CBA) a positive net pre- sent value (NPV) assures a surplus, as measured in dol- lars, which might, in principle, be redistributed (step 2 Box 1). In principle no one need have fewer dollars while leaving the beneficiary better off. In the case of health economics, the WTP is for a final health state (consequentialism) and from the revealed (stated) pref- erence criterion the surplus indicates an increase in the person’s utility. Consequently the positive NPV is ‘Pareto efficient’ (step 3) and social welfare will be in- creased (step 4). Note that only rarely are relative costs and benefits taken into account, although they can sig- nificantly affect social welfare via envy. With CEA the role of utility in this argument is largely replaced by an explicit target, commonly the life year (LY) or quality adjusted life year (QALY). Consequentialism is more explicit and social welfare is implicitly a linear function of the number and quality of life years deflated by a rate of time preference. The causal sequence is represented in Box 2. As benefits cannot be reduced to dollars, the cost/LY of different Service Benefit>Cost (WTP)>(OC.) Re d istribution noneworseoff Socialwelfare increase d Pareto efficiency = Indiv idual utilitie s; consequences Thisdo e s not/cannot occur Definition(only) Onlyifallnon‐ utilityobjectives ignored Box 1. The logic of cost benefits analysis. Step2 (Individual ) LY Step4 Socialwelfare increased Step3 Netgain Otherunitsof benefitposs ible eg QALYs Onlyif costs=budg etary, noteconomiccosts Onlyifvalue LY>costs OnlyifallnonLY obj ectivesig nored Step1 (Cost/LY) i <(co s t/ LY z ) Box 2. The logic of cost effectiveness analysis.  J. R. Richardson et al. / HEALTH 2 (2010) 1120-1133 Copyright © 2010 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ 1128 services are compared (step 1). Selecting the service with the minimum cost/LY allows more life years to be produced (step 2) which is considered to be a net gain (step 3) which increases social welfare (step 4). As with CBA, social welfare is only affected by total life years or QALYs (consequentialism), not by relative gains and losses. The explicit view in CBA that a dollar should be treated as a dollar due to potential compen- sation is replaced by the view that all QALYs should be treated equally [31]. As this cannot be judged by the potential to compensate those who do not receive QALYs (and are therefore dead) the judgement is an ethical assumption. Box 1 and Box 2 highlight the reliance of the two forms of economic evaluation upon the various as- sumptions. In Box 1 benefits are reduced to dollars (normally) by assuming that revealed preferences are the result of rational well-informed choice (step 1). But only the utility of the final health states, and util- ity-based indirect benefits and externalities, are in- cluded in the evaluation. Non-utility consequences and processes are excluded. The redistribution of benefits to ensure that no one is worse off in step 2 never occurs in practice in the health sector and often cannot occur - e.g. when people die [30,32]. Pareto efficiency need not result in an increase in social welfare if any of the ob- jectives assumed irrelevant by welfarism (e.g. those relating to equity which are independent of utility ef- fects) are in fact quantitatively important. The logic of CEA side-steps the initial problems of CBA typically by assuming that some spending will occur or that there is a fixed budget and that the prob- lem is how best to spend the resources. But this justifi- cation alters the logical sequence. Life years (or QA- LYs) (step 2) are only maximised if the ‘cost’ in step 1 is the constrained (budgetary) cost not resource cost. To illustrate this consider a project with small benefits but with no resource cost because the exceedingly high cost-to-budget is off-set by indirect benefits—cost sav- ings through an early return to work by patients. With costs/LY = 0 the project would be prioritised, exhaust- ing the budget and crowding out projects with a lower budget cost-to-benefit ratio which would achieve greater net benefits. In the UK the National Institute for Clinical Excel- lence (NICE) has recognised this problem and its guidelines specify that the relevant costs are those that relate to the NHS; that is, economic evaluation for the NHS longer employs economic costs. Similarly, NICE has sanctioned a (particular type of) QALY (based upon the EQ-5D QoL instrument) for cost utility analysis [33]; that is, it no longer employs the usual concept of economic benefits. The latter change has commonly been justified by an appeal to extra-welfarism. Coast et al. [34] note that ‘the apparent success of the extra-welfa- rist approach ... in the UK ... might lead to the view that there is general satisfaction with the theoretical ap- proach in health economics’ (p 1994). (The authors then express concern with this view.) However, the chief characteristic of extra-welfarism, on one interpretation [7], is its minimalism. (Other in- terpretations of extra-welfarism, which allow a place for health, utility, capabilities, and other factors, are also possible (Hurley 2000). It amounts to the assump- tion that the only purpose of the health sector, or at least an NHS, is the maximisation of health. The NICE directive to employ NHS costs may be considered a consequence of this theory/assumption. The unique feature of extra-welfarism - on its mini- malist interpretation - is its assertion that only health is of concern for economic evaluation, and the number of issues excluded by this form of extra-welfarism makes it highly contentious and, indeed, far more restrictive than welfare theory in which, in principle, no objec- tives are excluded as long as they are consequences which affect utility. The importance of health may in- deed be implied by Sen’s capabilities approach (and by other social philosophies [35]) but this does not estab- lish it as being the exclusive objective for an NHS. The assumptions that are necessary for the validity of the theory of CBA and CEA and the causal pathways shown in Boxes 1 and 2 are responsible for the anoma- lies that started this paper. The relationships between the anomalies, the (chief) assumptions from which they arise, and the (chief) problems with the assumptions are summarised in Table 2. A problem which emerges in the context of each anomaly is that the assumptions do not permit a satisfactory treatment of the distribution of costs and benefits. In effect, they extinguish the need for considerations of fairness and, more generally, any normative judgement with the sole exception of the assumption that social welfare as a function of utilities (in CBA) and that health is the only benefit of interest (in CEA). With the doctrine of revealed/stated prefer- ences or the assumption of a single objective, economic evaluation becomes a purely technical matter of ob- serving preferences or the assumed maximand and fol- lowing through the implications for costs and benefits. Other social judgements are unnecessary. Two assumptions are of particular importance in this process of excluding matters of fairness. First is the key assumption of welfarism stated above that only utility matters for social welfare. Apart from the circular ar- gument summarised in Figure 1 there is no satisfactory argument for believing that welfarism is true. The ex- istence of other ethical theories - including the deon-  J. R. Richardson et al. / HEALTH 2 (2010) 1120-1133 Copyright © 2010 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ 1129 Table 2. Anomalies and justifying assumptions. Are of anomaly Justifying assumption Problem* NPV Potential Pareto efficiency; potential compensation; validity of WTP Different persons receive benefits, costs; and no com- pensation occurs Benefits are redistributed Procedural and deontological goals are excluded WTP Benefits = (selfish) utility (only) Individualism, rationality Benefits (objectives) not restricted to selfish utility Communitarianism Non-rational behaviour Unwanted distribution of benefits Moral hazard Consequentialism Potential compensation Individualism Ex-ante (pre-outcome) benefits/costs Non transferable benefits Communitarianism Inequitable distribution of benefits Economic costs Sacrifice by a person = resource loss Health budgets not resources are the constraints in an NHS Tax burden to an individual = transfer, not a resource cost Equity and efficiency Separability of equity, efficiency Consequentialism Unfair to high CB patients Sharing, duty, procedural justice Distribution of benefits excludes high CB patients Sharing Individualism Communitarianism Non welfarist goals motivation Distribution of benefits unfair *Some of these are practical problems rather than theoretical - e.g. no compensation occurs in practice, procedural goals (‘process utility’) are not included in practice, etc. tology and religiously-based views, which are nomi- nally endorsed by the vast majority of the population - at least suggests the need for more than a bold assertion of welfarism. The compatibility of observations with welfarism is of lesser significance for its universality than the incompatibility of other observations (i. e. anomalies). The second key assumption is the Kaldor-Hicks po- tential compensation principle. It permits abstraction from the distribution of costs and benefits. Once NPV is positive it is as if it were ‘disembodied’ - unattached to any particular person - and can be shifted at will from person to person. But the principle is misleading. Firstly, ‘potential’ is not the same as ‘actual’. No amount of persuasion is likely to convince a person who has suffered a financial catastrophe that this out- come is desirable because another person has obtained a windfall from the same event that is more than suffi- cient to compensate the first person for their loss even though they will not do so. They may agree that the new situation is “efficient” according to the Kaldor- Hicks criterion. They could not disagree since the cri- terion is treated as a definition. But they might cer- tainly object that the outcome is unfair. Secondly when patients are left in a state of extreme disability or allowed to die, compensation is impossible even in principle and the Kaldor-Hicks criterion is ir- relevant. Finally, in the context of an NHS the argu- ment for potential compensation conflicts with the purpose of the NHS. This is to redistribute the cost of illness from those who are sick to the taxpayer: the taxpayer is the final loser (if only money and health are taken into account). Compensation would involve a reversal of this redistribution. The unhealthy who benefit from the NHS would be taxed in order to com- pensate the healthy. But this conflicts with the purpose of the scheme implying the irrelevance of the Kaldor- Hicks principle (again, unless “process utility”, “par- ticipatory utility”, “duty utility”, etc, are taken into account, which does not happen in practice). In CEA the assumption of welfarism is replaced with the adoption of a stated objective (LY, QALYs). There is no explicit equivalent to the Kaldor-Hicks criterion as the theory has been less developed than welfare the- ory. As noted, theoretical concerns have focused upon its consistency with the assumptions of orthodox eco- nomics rather than the development of an independent rationale for its methods. However, like CBA it has no satisfactory method for resolving issues associated with the distribution of benefits, and generally there is an implicit assumption that social welfare rises directly with the number of life years or QALYs gained. The assumption plays the same role as the Kaldor-Hicks principle in abstracting evaluation from issues of dis- tributive justice. 3.1. Empirical Ethics and a General Framework In both its practice and underlying theory economic evaluation based upon welfarism or extra welfarism  J. R. Richardson et al. / HEALTH 2 (2010) 1120-1133 Copyright © 2010 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ 1130 may be described as “efficiency focused”. As discussed above, assumptions largely purge the theory of the need for ethical decisions and, in practice, measurement fo- cuses upon efficiency. However, the evidence over- whelmingly suggests that the raison d’être for an NHS is not the maximisation of individual utility as defined in orthodox welfare economics—i.e. the maximisation of self-interested preferences. Nor does it suggest that maximising health is the only goal. Rather, the empiri- cal evidence, based on community surveys, suggest that the purpose of an NHS is to ensure fair treatment in health related matters, and this should be an important focus of the framework. The difficulty encountered in progressing beyond this point and developing the framework is that there is no objective basis for demonstrating the truth or supe- riority of a normative rule. There is a sufficient con- sensus about the importance of health, social justice and costs to conclude that the framework must include these, especially when they remain as abstract notions. But it is not possible to determine what other goals should be included or excluded and, when included, how they should be measured and weighted. With re- spect to this problem the literature is unhelpful. Welfa- rism might be considered an exception only because of its longevity and the elegance of the model woven from its troubled assumptions. 12 3 /1/ ii CostLYbabBudgetb LEbX We cannot offer a final solution to these problems. As argued elsewhere, there can be no objectively cor- rect metric - that is, no metric that everyone will agree upon [36]. Further, drawing normative conclusions di- rectly from objective evidence is a well-known error (the ‘naturalistic fallacy’). Nevertheless, for the solution of social problems it is important to know what the public thinks. This has been described elsewhere as empirical ethics [37,38]. It is little more than the suggestion that population values should be taken into account in the final decision algo- rithm or at least understood through empirical inquiry. Prima facie the proposition is trivial. Nevertheless, the suggestion has not been adopted and the volume of literature investigating population values and the prob- lems with basing normative conclusions on them re- mains negligible. Another literature, however, is helpful in this context. The broad principles of decision theory provide a flexi- ble and ‘commonsense’ approach to decision making. [39]. In this, objectives or dimensions of the choice set are independently obtained and weighted to reflect their relative importance. CBA can be viewed as an example of its simplest application. The two objectives, maxi- mising benefits and minimising costs are each given a unitary weight. However, weights need not be unitary and the objective function need not be additive. In the context of multi-attribute utility instruments for com- bining dimensions of a health state - the independently determined objectives—both the Health Utility Index (HUI) and Assessment of Quality of Life (AQoL) in- struments employ multiplicative models [40,41]. Eco- nometric methods may also be used including the new advanced methods of discrete choice modelling [42]. A major challenge to modelling is the inclusion of sharing as an objective. In the sharing study described in Section 2 Richardson et al. employed the economet- ric approach (a logit model) to predict the probability that a particular life-extending service would be se- lected from the four options when each option favoured a different person. The model took the form: 123 /1 /ii LnppabCostLYbBudgetbLEb X Where b is the probability of a person/disease receiving resources; LE is the person’s life expectancy (severity of condition) and Xi included variables for the share of the budget already received and life expectancy relative to that of others in the choice set. If the selection crite- rion for a service is a 50 per cent or more probability that it will be selected by the panel of respondents, the left hand side, LN p/(1-p) = 0, and a threshold cost/LY, may be calculated as: If LE and Xi were unimportant—as in CEA—then b3 = bi = 0 and the threshold at which there was a 50 per- cent chance of service selection would be 12 /1/CostLYbab Budget That is, the threshold would depend entirely upon the budget. When other variables are important, cost/LY is a function of these variables. Thus in the problematical case discussed in Section 2, where orthodox theory would leave a person to die (LE=0) if the cost/LY ex- ceeded the threshold, the effect of the imminent death would increase cost/LY threshold according to the weight b3/b1. Results from the analysis of 41,000 observations generated from 544 subjects indicated that the impor- tance of LE resulted in very significant sharing. The results, more generally, show respondents, adopting a social perspective, were prepared to sacrifice almost one third of potential life years to achieve optimal sharing. This exercise was illustrative. A wider range of so- cial values could be tested and different combination rules employed. The general result would be the re- placement of the fixed cost-effectiveness threshold of present CEA with a variable threshold which was de-  J. R. Richardson et al. / HEALTH 2 (2010) 1120-1133 Copyright © 2010 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ 1131 pendent upon the attributes of these receiving the ser- vice and the extent of sharing. The chief obstacle to the development of such a framework, of course, is agreement upon health-related social goals and the creation of instruments for their measurement. The task is problematical in large part because, to date, there has been virtually no discussion in the mainstream literature of how social goals should be determined—i.e. what should be the criteria for the adoption of objectives. 4. CONCLUSIONS There is an adage that for every complex problem there is always a simple solution which is wrong. The eco- nomic evaluation of health services is a complex prob- lem and welfare theory is simple, elegant and beguiling. Minimalist extra-welfarism and CEA as practised en- capsulate a single assumption with respect to the pur- pose of an NHS. We have argued here that this simplic- ity is, at best, misleading. Its perpetuation is undoubt- edly related to three factors. First, there is an obvious need to ration the use of finite resources and current economic evaluation methods provide one way of do- ing this. Second, the implied methods and rationale incorporate elements that are undoubtedly important. Costs, budgetary costs and benefits, as presently de- fined, must clearly play a very large role in the decision process. Third, and as noted in the introduction, errors in theory will not lead to dramatic events. Bridges will not fall down and the stock exchange will not collapse. Rather, we will treat people unfairly but neither deci- sion makers or patients will notice this. Very few Aus- tralians are aware of the huge discrepancies in the pro- vision of services across the country but their distribu- tion is nevertheless unfair. We have argued that the root problem is a method- ology based upon misleading and over-restrictive as- sumptions. The assumptions of welfare theory purport to be universally true and therefore applicable to the health sector. But direct evidence contradicts the uni- versality of the behavioural assumptions and other as- sumptions needed to operationalise the theory are deeply problematical. The assumption of only health maximisation in extra-welfarism is even more restric- tive than the assumptions of Welfare Theory. It is sim- ply easier to operationalise. However, in this article we have not focused primarily upon the assumptions. Rather, the article has challenged the validity of the current approach another way. It has looked at some of the consequences of the assumptions and demonstrated that they are anomalous. As Popper [43] notes, theories may, in principle, be falsified not verified and the iden- tification of anomalies is therefore an important chal- lenge to a theory. However he also notes in practice, falsification can always be avoided by changing defini- tions, objectives or by making ad hoc repairs. The ar- gument embedded in Figure 1 for example and varia- tions of it can allow welfare theory to evade falsifica- tion indefinitely, if that is the objective. However this will result in the type of disjunction between theory and practice which, we argue, already occurs as decision- makers approve services with a high cost/LY for a vari- ety of “pragmatic reasons”. Finally, our critique does not imply that current work is worthless. The variables included in economic evaluation costs and benefits as measured are evidently of some importance. Rather, our criticism is that they are based upon a bad theory which is highly restrictive in the elements that it permits to be considered and which claim a universality that is not justified. We have suggested that a more pluralistic framework based upon some of the insights of decision theory will be less co- ercive and more flexible. Many- and possibly the ma- jority of the recommendations of economic evaluation would remain unchanged. A more realistic framework could also overcome the anomalies discussed here. A theory that is not true in one context may be appli- cable in another. In particular, a theory that is satisfac- tory in the supermarket (based upon self-interest, will- ingness to pay and consumer sovereignty) cannot simply be assumed to be true in the health sector. Deriving the authority of economic evaluation from the authority of ‘economic theory’ is unsatisfactory if the assumptions are not universally true in the context of positive analy- sis and if they lead to anomalies in normative theory. Despite this, present methods and theory satisfy the im- mediate goals of theorists and decision makers and are unlikely to change quickly. Policy makers want answers; their advisors benefit from the authority they have ac- creted from the theory. However, for the reasons outlined here, we believe that a better approach to theory exists and that decision makers should retain their pragmatism and treat with scepticism assertions that they should be guided exclusively by the net present value or cost/ QALY rule. The evidence and argument here suggests that the underlying assumptions have implications that conflict with people’s moral preferences and, in some instances are absurd. REFERENCES [1] Mandelbrot, B.B. (1997) Fractals and scaling in finance. Springer, New York. [2] Skidelsky, A. (2009) Keynes: The return of the master. Allen Lane, London. 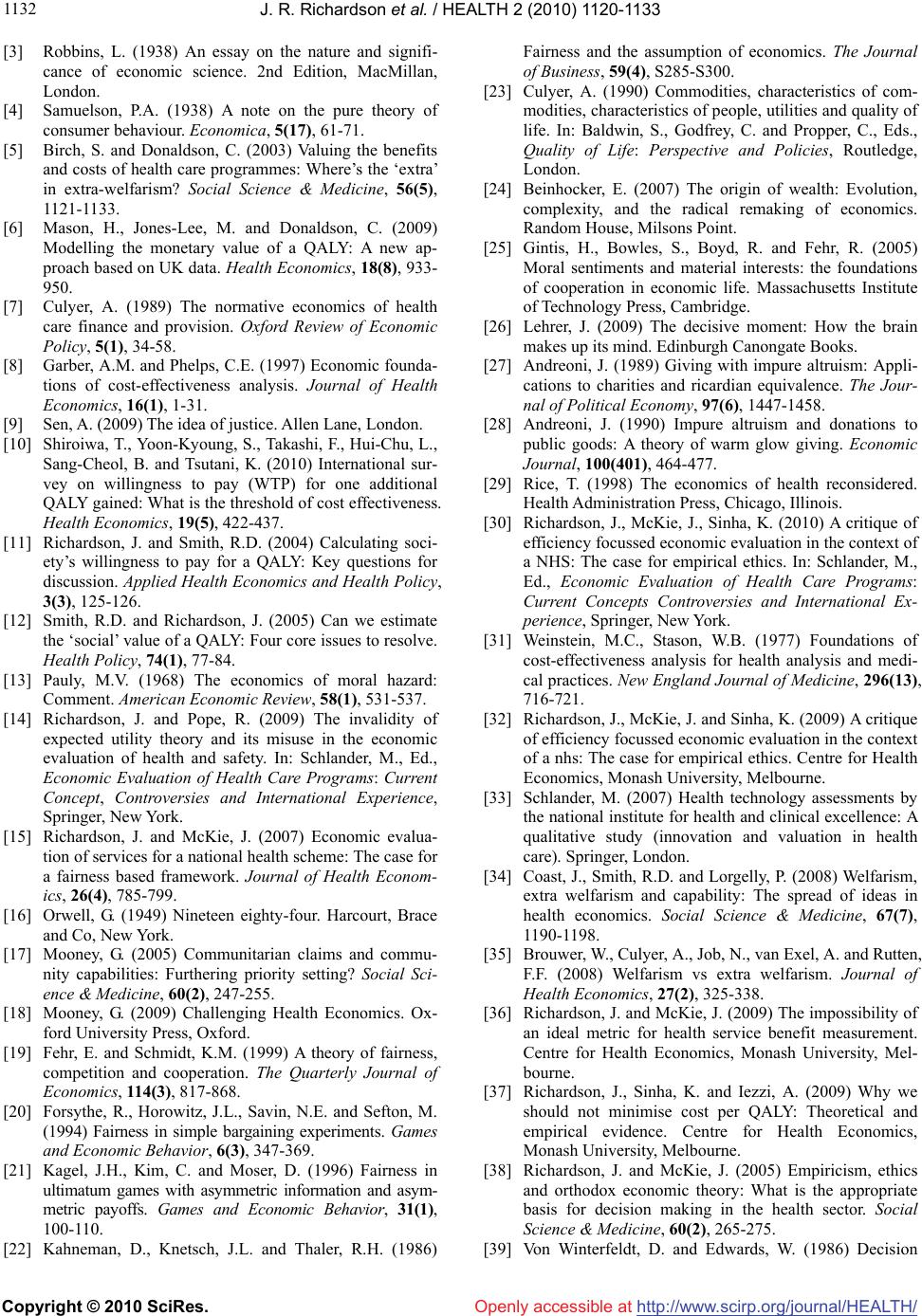 J. R. Richardson et al. / HEALTH 2 (2010) 1120-1133 Copyright © 2010 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ 1132 [3] Robbins, L. (1938) An essay on the nature and signifi- cance of economic science. 2nd Edition, MacMillan, London. [4] Samuelson, P.A. (1938) A note on the pure theory of consumer behaviour. Economica, 5(17), 61-71. [5] Birch, S. and Donaldson, C. (2003) Valuing the benefits and costs of health care programmes: Where’s the ‘extra’ in extra-welfarism? Social Science & Medicine, 56(5), 1121-1133. [6] Mason, H., Jones-Lee, M. and Donaldson, C. (2009) Modelling the monetary value of a QALY: A new ap- proach based on UK data. Health Economics, 18(8), 933- 950. [7] Culyer, A. (1989) The normative economics of health care finance and provision. Oxford Review of Economic Policy, 5(1), 34-58. [8] Garber, A.M. and Phelps, C.E. (1997) Economic founda- tions of cost-effectiveness analysis. Journal of Health Economics, 16(1), 1-31. [9] Sen, A. (2009) The idea of justice. Allen Lane, London. [10] Shiroiwa, T., Yoon-Kyoung, S., Takashi, F., Hui-Chu, L., Sang-Cheol, B. and Tsutani, K. (2010) International sur- vey on willingness to pay (WTP) for one additional QALY gained: What is the threshold of cost effectiveness. Health Economics, 19(5), 422-437. [11] Richardson, J. and Smith, R.D. (2004) Calculating soci- ety’s willingness to pay for a QALY: Key questions for discussion. Applied Health Economics and Health Policy, 3(3), 125-126. [12] Smith, R.D. and Richardson, J. (2005) Can we estimate the ‘social’ value of a QALY: Four core issues to resolve. Health Policy, 74(1), 77-84. [13] Pauly, M.V. (1968) The economics of moral hazard: Comment. American Economic Review, 58(1), 531-537. [14] Richardson, J. and Pope, R. (2009) The invalidity of expected utility theory and its misuse in the economic evaluation of health and safety. In: Schlander, M., Ed., Economic Evaluation of Health Care Programs: Current Concept, Controversies and International Experience, Springer, New York. [15] Richardson, J. and McKie, J. (2007) Economic evalua- tion of services for a national health scheme: The case for a fairness based framework. Journal of Health Econom- ics, 26(4), 785-799. [16] Orwell, G. (1949) Nineteen eighty-four. Harcourt, Brace and Co, New York. [17] Mooney, G. (2005) Communitarian claims and commu- nity capabilities: Furthering priority setting? Social Sci- ence & Medicine, 60(2), 247-255. [18] Mooney, G. (2009) Challenging Health Economics. Ox- ford University Press, Oxford. [19] Fehr, E. and Schmidt, K.M. (1999) A theory of fairness, competition and cooperation. The Quarterly Journal of Economics, 114(3), 817-868. [20] Forsythe, R., Horowitz, J.L., Savin, N.E. and Sefton, M. (1994) Fairness in simple bargaining experiments. Games and Economic Behavior, 6(3), 347-369. [21] Kagel, J.H., Kim, C. and Moser, D. (1996) Fairness in ultimatum games with asymmetric information and asym- metric payoffs. Games and Economic Behavior, 31(1), 100-110. [22] Kahneman, D., Knetsch, J.L. and Thaler, R.H. (1986) Fairness and the assumption of economics. The Journal of Business, 59(4), S285-S300. [23] Culyer, A. (1990) Commodities, characteristics of com- modities, characteristics of people, utilities and quality of life. In: Baldwin, S., Godfrey, C. and Propper, C., Eds., Quality of Life: Perspective and Policies, Routledge, London. [24] Beinhocker, E. (2007) The origin of wealth: Evolution, complexity, and the radical remaking of economics. Random House, Milsons Point. [25] Gintis, H., Bowles, S., Boyd, R. and Fehr, R. (2005) Moral sentiments and material interests: the foundations of cooperation in economic life. Massachusetts Institute of Technology Press, Cambridge. [26] Lehrer, J. (2009) The decisive moment: How the brain makes up its mind. Edinburgh Canongate Books. [27] Andreoni, J. (1989) Giving with impure altruism: Appli- cations to charities and ricardian equivalence. The Jour- nal of Political Economy, 97(6), 1447-1458. [28] Andreoni, J. (1990) Impure altruism and donations to public goods: A theory of warm glow giving. Economic Journal, 100(401), 464-477. [29] Rice, T. (1998) The economics of health reconsidered. Health Administration Press, Chicago, Illinois. [30] Richardson, J., McKie, J., Sinha, K. (2010) A critique of efficiency focussed economic evaluation in the context of a NHS: The case for empirical ethics. In: Schlander, M., Ed., Economic Evaluation of Health Care Programs: Current Concepts Controversies and International Ex- perience, Springer, New York. [31] Weinstein, M.C., Stason, W.B. (1977) Foundations of cost-effectiveness analysis for health analysis and medi- cal practices. New England Journal of Medicine, 296(13), 716-721. [32] Richardson, J., McKie, J. and Sinha, K. (2009) A critique of efficiency focussed economic evaluation in the context of a nhs: The case for empirical ethics. Centre for Health Economics, Monash University, Melbourne. [33] Schlander, M. (2007) Health technology assessments by the national institute for health and clinical excellence: A qualitative study (innovation and valuation in health care). Springer, London. [34] Coast, J., Smith, R.D. and Lorgelly, P. (2008) Welfarism, extra welfarism and capability: The spread of ideas in health economics. Social Science & Medicine, 67(7), 1190-1198. [35] Brouwer, W., Culyer, A., Job, N., van Exel, A. and Rutten, F.F. (2008) Welfarism vs extra welfarism. Journal of Health Economics, 27(2), 325-338. [36] Richardson, J. and McKie, J. (2009) The impossibility of an ideal metric for health service benefit measurement. Centre for Health Economics, Monash University, Mel- bourne. [37] Richardson, J., Sinha, K. and Iezzi, A. (2009) Why we should not minimise cost per QALY: Theoretical and empirical evidence. Centre for Health Economics, Monash University, Melbourne. [38] Richardson, J. and McKie, J. (2005) Empiricism, ethics and orthodox economic theory: What is the appropriate basis for decision making in the health sector. Social Science & Medicine, 60(2), 265-275. [39] Von Winterfeldt, D. and Edwards, W. (1986) Decision  J. R. Richardson et al. / HEALTH 2 (2010) 1120-1133 Copyright © 2010 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ 1133 analysis and behavioral research. Cambridge University Press, Cambridge. [40] Feeny, D., Furlong, W., Torrance, G., Goldsmith, C., Zhu, Z., DePaw, S., et al. (2002) Multiattribute and single-attr- ibute utility functions for the Health Utility Index Mark 3 system. Medical Care, 40(2), 113-128. [41] Feeny, D.H., Torrance, G.W. and Furlong, W.J. (1996) Health utilities index. In: Spilker, B., Ed., Quality of Life and Pharmacoeconomucs in Clinical Trials, Lippin- cott-Raven Publishers, Philidelphia. [42] Burgess, L., Street, D.J., Viney, R. and Louviere, J. (2007) Design of hoice experiments in health economics. The Elgar Companion to Health Economics. Edward Elgar, Cheltenham. [43] Popper, K. (1959) The logic of scientific discovery. Hut- chinson, London. [44] Richardson, J., McKie, J. and Sinha, K. (2009) A critique of efficiency-focused economic evaluation in the context of a NHS: The case for empirical ethics. In: Schlander, M., Ed., Economic Evaluation of Health Care Programs: Current Concepts Controversies and International Ex- perience, Springer, New York. |