Paper Menu >>
Journal Menu >>
 Vol.2, No.9, 1093-1096 (2010) Health doi:10.4236/health.2010.29161 Copyright © 2010 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ A new device for the identification of lymph nodes removed during different types of neck dissection Imre Gerlinger1*, Tamás Ferenc Molnár2, Tamás Járai1, Péter Móricz1, Gábor Ráth1, Gyula Göbel1 1Department of Otorhinolaryngology & Head and Neck Surgery, Medical School, University of Pécs, Pécs, Hungary; *Corresponding Author: i.gerlinger@freemail.hu 2Department of Otorhinolaryngology & Surgery, Medical School, University of Pécs, Pécs, Hungary Received 9 January 2010; revised 21 January 2010; accepted 1 February 2010. ABSTRACT Meticulous mapping of the lymph node status is a general principle in present-day head and neck surgery. The removal of a certain number of lymphatic levels during neck dissection may well be therapeutic in intent, but it is also mandatory for correct tumour staging. We pre- sent a precise lymph node mapping during dif- ferent types of neck dissection in the course of major head and neck surgery by a sterile plastic tray moulded in the shape of the neck. This de- vice makes lymph node mapping simpler, safer, quicker and methodically more structured than any of the present methods. It facilitates the work of the pathologist and the flow of reliable information along the surgeon-pathologist- oncologist chain. With this device, a more stru- ctured, methodical means of lymph node re- moval has become possible. Keywords: Head and Neck Surgery; Lymph Node Mapping; Neck Dissection 1. INTRODUCTION In 1906, George Crile published a report on what is now considered the first surgical procedure for the en bloc resection of cervical nodes [1]. Until the 1950s, his radical neck dissection technique underwent only modest technical improvements and there was little clarification of the indications for the procedure. During the 1960s, the ideas of Suarez and Ballantyne led to advances in the technique of conservative neck dissection [2]. For the first time the non-lymphatic structures (the spinal acces- sory nerve, the internal jugular vein and the sternoclei- domastoid muscle) were preserved, and only the lymph nodes between the aponeurotic compartments of the neck were removed [3]. Today, a variety of different types of neck dissection are available that are considered on- co- logically, functionally and cosmetically effective in the therapeutic or prophylactic treatment of the neck in pa- tients with head and neck cancers. These less radical surgical procedures are often performed bilaterally, and may be followed by postoperative radiotherapy with a very similar recurrence ratio as observed after radi- cal/modified radical neck dissections [4,5]. Meticulous mapping of the lymph node status is a general principle in present-day head and neck surgery. The removal of a certain number of lymphatic levels during neck dissection may well be therapeutic in intent, but it is also mandatory for correct tumour staging [6]. Te decisions concerning the prognosis, postoperative adjuvant therapy at the individual level and the audit at the departmental level are impossible without proper TNM staging [7]. As in other manual specialities, the identification, handling, collecting and appropriate labelling of the in- dividual lymph nodes according to their origin during different types of neck dissection is a time-consuming procedure all participants concerned. This seemingly minor problem is customarily solved by the usage of labelled individual vials or small bottles. The routine of individual ENT surgeons practising neck dissections is determined by a long list of factors, but it is clear that lymph node mapping is not ideally standardized and integrated into the daily routine [6]. Deficiencies and substandard attitudes towards the im- portance of the mapping can not be dealt with here, but it is perfectly obvious that after a neck dissection, careful attention and an extra workload are needed on the part of all the theatre staff. Their number, quality and level of enthusiasm are frequently underestimated potential sour- ces of the misplacing and mishandling of specimens. Over noisy verbal instructions given in the course of 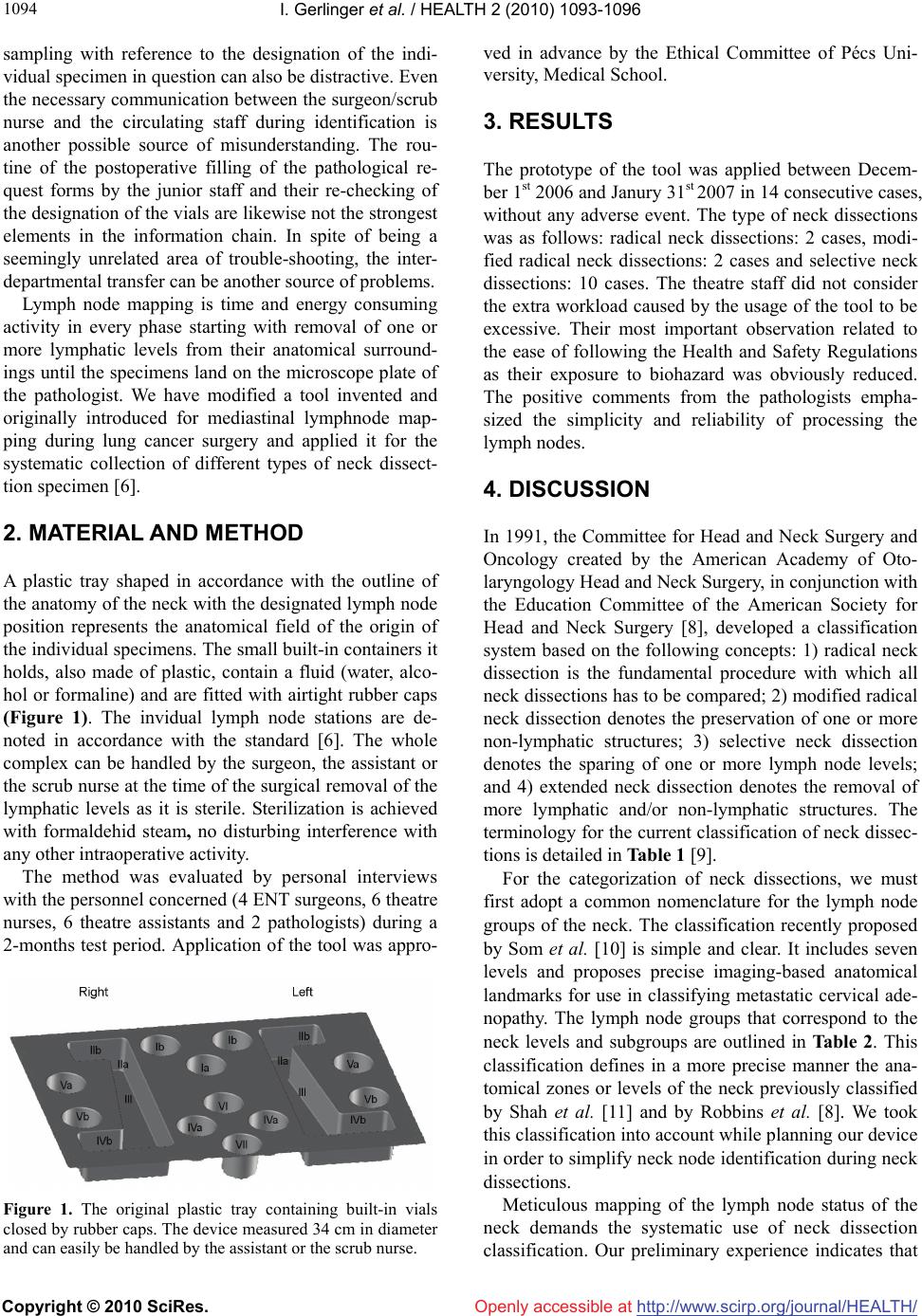 I. Gerlinger et al. / HEALTH 2 (2010) 1093-1096 Copyright © 2010 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ 1094 sampling with reference to the designation of the indi- vidual specimen in question can also be distractive. Even the necessary communication between the surgeon/scrub nurse and the circulating staff during identification is another possible source of misunderstanding. The rou- tine of the postoperative filling of the pathological re- quest forms by the junior staff and their re-checking of the designation of the vials are likewise not the strongest elements in the information chain. In spite of being a seemingly unrelated area of trouble-shooting, the inter- departmental transfer can be another source of problems. Lymph node mapping is time and energy consuming activity in every phase starting with removal of one or more lymphatic levels from their anatomical surround- ings until the specimens land on the microscope plate of the pathologist. We have modified a tool invented and originally introduced for mediastinal lymphnode map- ping during lung cancer surgery and applied it for the systematic collection of different types of neck dissect- tion specimen [6]. 2. MATERIAL AND METHOD A plastic tray shaped in accordance with the outline of the anatomy of the neck with the designated lymph node position represents the anatomical field of the origin of the individual specimens. The small built-in containers it holds, also made of plastic, contain a fluid (water, alco- hol or formaline) and are fitted with airtight rubber caps (Figure 1). The invidual lymph node stations are de- noted in accordance with the standard [6]. The whole complex can be handled by the surgeon, the assistant or the scrub nurse at the time of the surgical removal of the lymphatic levels as it is sterile. Sterilization is achieved with formaldehid steam, no disturbing interference with any other intraoperative activity. The method was evaluated by personal interviews with the personnel concerned (4 ENT surgeons, 6 theatre nurses, 6 theatre assistants and 2 pathologists) during a 2-months test period. Application of the tool was appro- Figure 1. The original plastic tray containing built-in vials closed by rubber caps. The device measured 34 cm in diameter and can easily be handled by the assistant or the scrub nurse. ved in advance by the Ethical Committee of Pécs Uni- versity, Medical School. 3. RESULTS The prototype of the tool was applied between Decem- ber 1st 2006 and Janury 31st 2007 in 14 consecutive cases, without any adverse event. The type of neck dissections was as follows: radical neck dissections: 2 cases, modi- fied radical neck dissections: 2 cases and selective neck dissections: 10 cases. The theatre staff did not consider the extra workload caused by the usage of the tool to be excessive. Their most important observation related to the ease of following the Health and Safety Regulations as their exposure to biohazard was obviously reduced. The positive comments from the pathologists empha- sized the simplicity and reliability of processing the lymph nodes. 4. DISCUSSION In 1991, the Committee for Head and Neck Surgery and Oncology created by the American Academy of Oto- laryngology Head and Neck Surgery, in conjunction with the Education Committee of the American Society for Head and Neck Surgery [8], developed a classification system based on the following concepts: 1) radical neck dissection is the fundamental procedure with which all neck dissections has to be compared; 2) modified radical neck dissection denotes the preservation of one or more non-lymphatic structures; 3) selective neck dissection denotes the sparing of one or more lymph node levels; and 4) extended neck dissection denotes the removal of more lymphatic and/or non-lymphatic structures. The terminology for the current classification of neck dissec- tions is detailed in Table 1 [9]. For the categorization of neck dissections, we must first adopt a common nomenclature for the lymph node groups of the neck. The classification recently proposed by Som et al. [10] is simple and clear. It includes seven levels and proposes precise imaging-based anatomical landmarks for use in classifying metastatic cervical ade- nopathy. The lymph node groups that correspond to the neck levels and subgroups are outlined in Table 2. This classification defines in a more precise manner the ana- tomical zones or levels of the neck previously classified by Shah et al. [11] and by Robbins et al. [8]. We took this classification into account while planning our device in order to simplify neck node identification during neck dissections. Meticulous mapping of the lymph node status of the neck demands the systematic use of neck dissection classification. Our preliminary experience indicates that 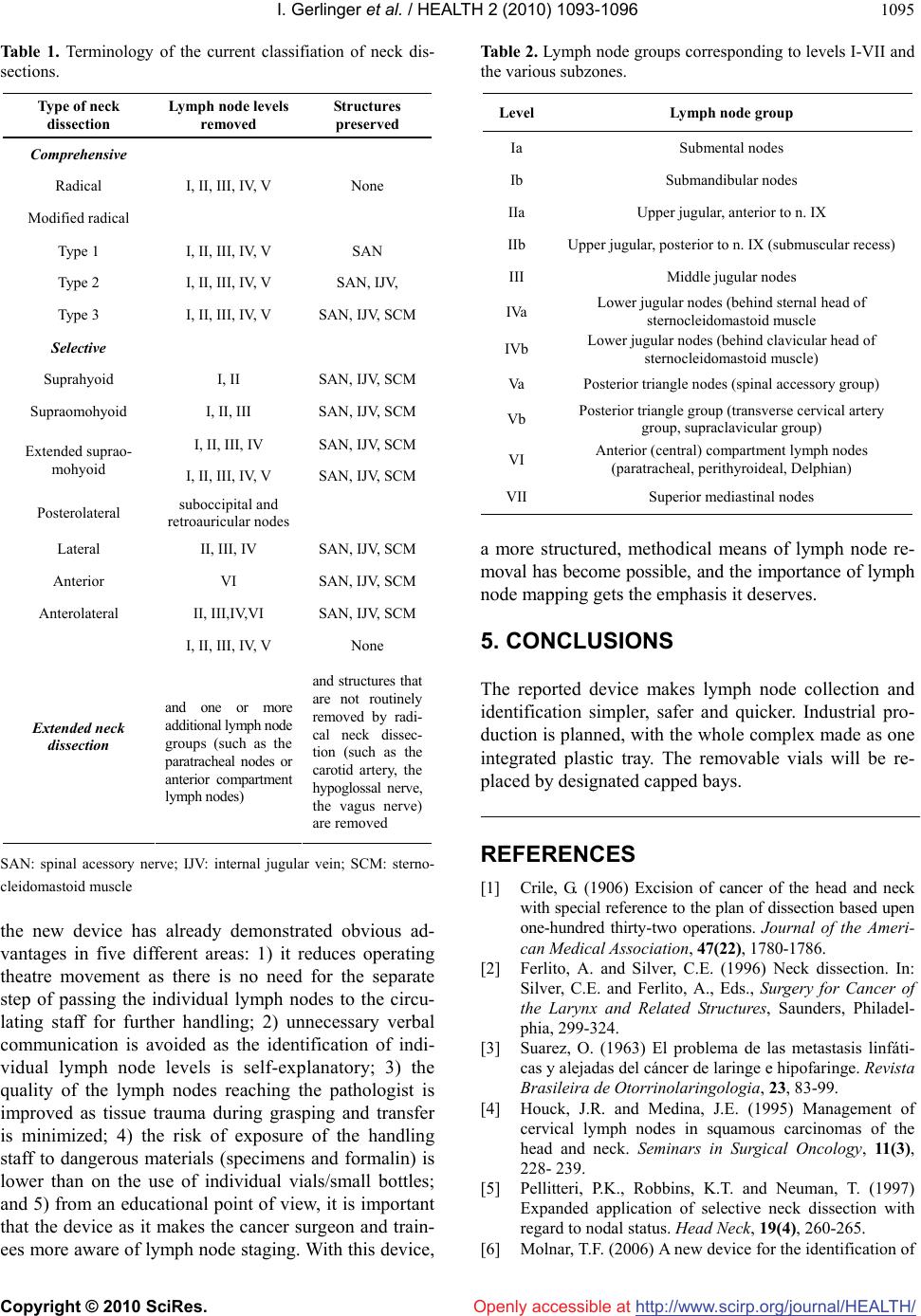 I. Gerlinger et al. / HEALTH 2 (2010) 1093-1096 Copyright © 2010 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ 1095 Table 1. Terminology of the current classifiation of neck dis- sections. Type of neck dissection Lymph node levels removed Structures preserved Comprehensive Radical I, II, III, IV, V None Modified radical Type 1 I, II, III, IV, V SAN Type 2 I, II, III, IV, V SAN, IJV, Type 3 I, II, III, IV, V SAN, IJV, SCM Selective Suprahyoid I, II SAN, IJV, SCM Supraomohyoid I, II, III SAN, IJV, SCM I, II, III, IV SAN, IJV, SCM Extended suprao- mohyoid I, II, III, IV, V SAN, IJV, SCM Posterolateral suboccipital and retroauricular nodes Lateral II, III, IV SAN, IJV, SCM Anterior VI SAN, IJV, SCM Anterolateral II, III,IV,VI SAN, IJV, SCM I, II, III, IV, V None Extended neck dissection and one or more additional lymph node groups (such as the paratracheal nodes or anterior compartment lymph nodes) and structures that are not routinely removed by radi- cal neck dissec- tion (such as the carotid artery, the hypoglossal nerve, the vagus nerve) are removed SAN: spinal acessory nerve; IJV: internal jugular vein; SCM: sterno- cleidomastoid muscle the new device has already demonstrated obvious ad- vantages in five different areas: 1) it reduces operating theatre movement as there is no need for the separate step of passing the individual lymph nodes to the circu- lating staff for further handling; 2) unnecessary verbal communication is avoided as the identification of indi- vidual lymph node levels is self-explanatory; 3) the quality of the lymph nodes reaching the pathologist is improved as tissue trauma during grasping and transfer is minimized; 4) the risk of exposure of the handling staff to dangerous materials (specimens and formalin) is lower than on the use of individual vials/small bottles; and 5) from an educational point of view, it is important that the device as it makes the cancer surgeon and train- ees more aware of lymph node staging. With this device, Table 2. Lymph node groups corresponding to levels I-VII and the various subzones. Level Lymph node group Ia Submental nodes Ib Submandibular nodes IIa Upper jugular, anterior to n. IX IIb Upper jugular, posterior to n. IX (submuscular recess) III Middle jugular nodes IVa Lower jugular nodes (behind sternal head of sternocleidomastoid muscle IVb Lower jugular nodes (behind clavicular head of sternocleidomastoid muscle) Va Posterior triangle nodes (spinal accessory group) Vb Posterior triangle group (transverse cervical artery group, supraclavicular group) VI Anterior (central) compartment lymph nodes (paratracheal, perithyroideal, Delphian) VII Superior mediastinal nodes a more structured, methodical means of lymph node re- moval has become possible, and the importance of lymph node mapping gets the emphasis it deserves. 5. CONCLUSIONS The reported device makes lymph node collection and identification simpler, safer and quicker. Industrial pro- duction is planned, with the whole complex made as one integrated plastic tray. The removable vials will be re- placed by designated capped bays. REFERENCES [1] Crile, G. (1906) Excision of cancer of the head and neck with special reference to the plan of dissection based upen one-hundred thirty-two operations. Journal of the Ameri- can Medical Association, 47(22), 1780-1786. [2] Ferlito, A. and Silver, C.E. (1996) Neck dissection. In: Silver, C.E. and Ferlito, A., Eds., Surgery for Cancer of the Larynx and Related Structures, Saunders, Philadel- phia, 299-324. [3] Suarez, O. (1963) El problema de las metastasis linfáti- cas y alejadas del cáncer de laringe e hipofaringe. Revista Brasileira de Otorrinolaringologia, 23, 83-99. [4] Houck, J.R. and Medina, J.E. (1995) Management of cervical lymph nodes in squamous carcinomas of the head and neck. Seminars in Surgical Oncology, 11(3), 228- 239. [5] Pellitteri, P.K., Robbins, K.T. and Neuman, T. (1997) Expanded application of selective neck dissection with regard to nodal status. Head Neck, 19(4), 260-265. [6] Molnar, T.F. (2006) A new device for the identification of  I. Gerlinger et al. / HEALTH 2 (2010) 1093-1096 Copyright © 2010 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ 1096 lymph nodes at lung surgery. European Journal of Car- dio-Thoracic Surgery, 31(2), 311-312. [7] Ferlito, A., Som, P.M., Rinaldo, A. and Mondin, V. (2000) Classification and terminology of neck dissections. ORL: Journal for Oto-Rhino-Laryngology and Its Related Spe- cialties, 62(4), 212-216. [8] Robbins, K.T., Medina, J.E., Wolfe, G.T., Levine, P.A., Sessions, R.B. and Pruet, C.B. (1991) Standardizing neck dissection terminology. Offical report of the academy’s committee for head and neck surgery and oncology. Ar- chives of Otolaryngology - Head & Neck Surgery, 117(6), 601-605. [9] Ferlito, A. and Rinaldo, A. (1998) Selective lateral neck dissection for laryngeal cancer in clinically negative neck: Is it justified? Journal of Laryngology & Otology, 112 (10), 921-924. [10] Som, P.M., Curtin, H.D. and Mancuso, A.A. (1999) An imaging based classification for the cervical nodes de- signed as an adjunct to recent clinically based nodal clas- sifications. Archives of Otolaryngology - Head & Neck Surgery, 125(4), 388-396. [11] Shah, J.P., Strong, E., Spiro, R.H. and Vikram, B. (1981) Neck dissection: Current status and future possibilities. Clinic Bull, 11(1), 25-33. |